Aminaglycoside its intro, pharmacokinetics, pharmacodynamics, mechanism of action, classification, individual drugs explanation with important point, adverse effects
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have all the key information I need. I have the full chapter content from Katzung covering introduction, mechanism, PK/PD, resistance, adverse effects, and individual drugs. Now I can write the comprehensive answer.
Aminoglycosides - A Complete Overview
Source: Katzung's Basic and Clinical Pharmacology, 16th Edition
1. Introduction
Aminoglycosides are a class of potent bactericidal antibiotics derived from soil actinomycetes bacteria. Streptomycin was the first aminoglycoside, discovered in 1943 from Streptomyces griseus, and it was the first antibiotic effective against tuberculosis. The class is characterized by:
- Polycationic, polar molecules - poor lipid solubility
- Bactericidal activity (concentration-dependent killing)
- Activity primarily against aerobic gram-negative bacilli and some gram-positive organisms
- Narrow therapeutic window - significant toxicity potential
Chemical Structure: All aminoglycosides consist of an aminocyclitol ring (2-deoxystreptamine or streptamine) linked to amino sugars by glycosidic bonds. The multiple amino groups confer a positive charge at physiologic pH, which is critical for binding to bacterial ribosomes.
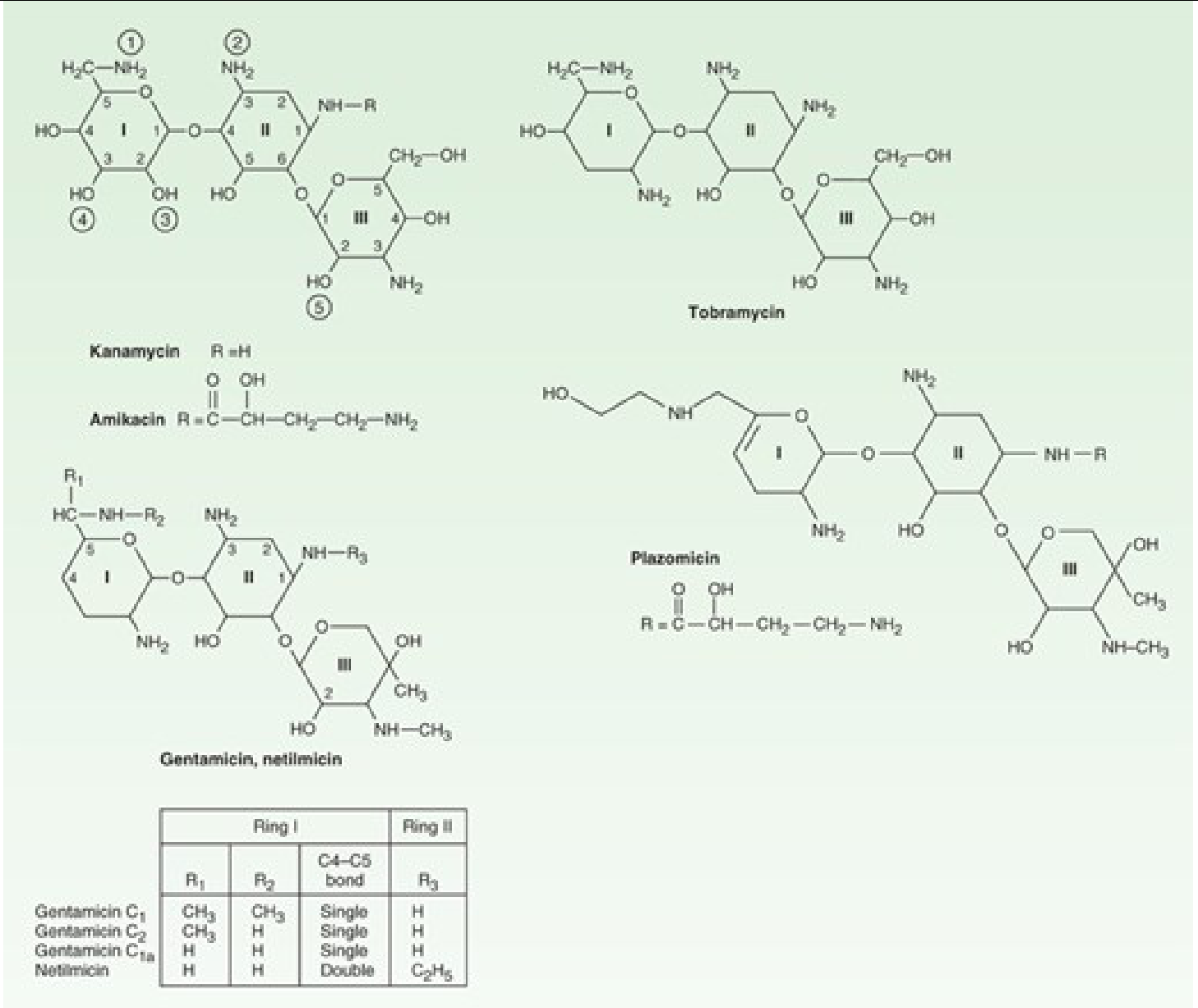
Chemical structures of major aminoglycosides - Katzung's Basic and Clinical Pharmacology, 16e
2. Classification
By Source:
| Source | Drugs |
|---|---|
| Streptomyces griseus | Streptomycin, neomycin, kanamycin, tobramycin |
| Micromonospora spp. | Gentamicin, sisomicin, netilmicin |
| Semi-synthetic | Amikacin (derived from kanamycin), plazomicin, netilmicin |
Naming tip: Drugs from Streptomyces end in -mycin; drugs from Micromonospora end in -micin.
By Generation / Clinical Use:
| Group | Drugs | Key Use |
|---|---|---|
| Prototype | Streptomycin | TB, plague, brucellosis |
| Broad-spectrum | Gentamicin, Tobramycin, Amikacin | Gram-negative infections, sepsis |
| Limited/topical | Neomycin, Kanamycin | Topical, pre-op bowel prep |
| Newer | Plazomicin | MDR gram-negative infections |
3. Mechanism of Action
The mode of action of streptomycin has been studied most closely, but all aminoglycosides act similarly.
Step 1 - Entry into the bacterial cell:
- Passive diffusion across the outer membrane via porin channels
- Active transport across the inner (cell) membrane driven by the transmembrane electrochemical gradient (oxygen-dependent proton pump mechanism)
- Low pH and anaerobic conditions reduce this gradient and impair transport - this is why aminoglycosides are ineffective against anaerobes
- Cell wall-active drugs (penicillin, vancomycin) enhance aminoglycoside uptake, forming the basis of synergy
Step 2 - Ribosomal binding and protein synthesis inhibition:
Once inside, aminoglycosides bind to 30S ribosomal subunit proteins and inhibit protein synthesis by three simultaneous mechanisms:
- Interference with initiation complex formation - blocks the start of translation
- mRNA misreading - causes incorporation of incorrect amino acids into the growing peptide chain, producing nonfunctional or toxic proteins
- Polysome breakup - polysomes fragment into nonfunctional monosomes
These effects are irreversible and lead directly to cell death (bactericidal effect).
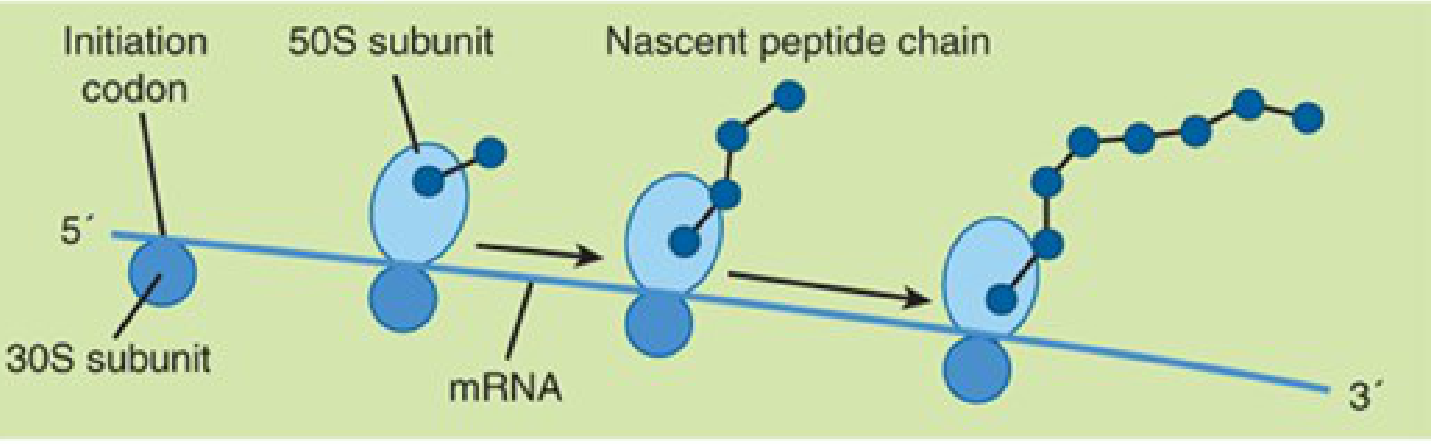
Normal bacterial cell protein synthesis (30S + 50S ribosome translating mRNA) - Katzung's Basic and Clinical Pharmacology, 16e
Important note: The misread proteins insert into the cell membrane, increasing membrane permeability, which allows even more aminoglycoside to enter - creating a self-amplifying lethal cycle.
4. Pharmacokinetics
| Parameter | Detail |
|---|---|
| Absorption | Poorly absorbed from intact GI tract; almost all of oral dose excreted in feces. Can be absorbed if GI ulcerations present. |
| Route | IV infusion (30-60 min) or IM. Not given orally for systemic infections. |
| After IM | Peak blood concentration in 30-90 minutes |
| Half-life | 2-3 hours (normal renal function); rises to 24-48 hours in renal impairment |
| Distribution | Highly polar - do not enter cells readily. Excluded from CNS and eye under normal conditions. In active CNS inflammation, CSF levels reach ~20% of plasma. Renal cortex accumulates highest concentrations. |
| Protein binding | Low (<10%) |
| CSF penetration | Poor - intrathecal/intraventricular injection needed for high CNS levels |
| Bile levels | ~30% of serum levels |
| Pleural/synovial fluid | 50-90% of plasma with prolonged therapy |
| Elimination | Renal excretion - directly proportional to creatinine clearance |
| Dialysis | Partially removed by hemodialysis (40-60% for gentamicin); even less by peritoneal dialysis |
Dosing Strategy - Once-Daily vs. Traditional:
Aminoglycosides exhibit concentration-dependent killing plus a significant post-antibiotic effect (PAE) lasting several hours. This means higher peak concentrations kill bacteria faster and better, and antibacterial activity persists after drug levels fall.
Once-daily dosing (ODD):
- Preferred in most clinical situations
- Gentamicin/tobramycin: 5-7 mg/kg once daily (if CrCl >60 mL/min)
- Amikacin/plazomicin: 15 mg/kg once daily
- Check levels between 18-24 hours; goal trough <1 mcg/mL
- Avoid in: renal failure (CrCl <60), pregnancy, neonates, enterococcal/staphylococcal prosthetic valve endocarditis
Traditional dosing (divided doses q8h):
- Peak target: 5-10 mcg/mL (8-10 mcg/mL for serious infections)
- Trough target: <2 mcg/mL (<1 mcg/mL optimal)
- Required for endocarditis combination therapy
5. Pharmacodynamics
| Property | Detail |
|---|---|
| Killing pattern | Concentration-dependent (higher peak = greater kill rate) |
| PK/PD index | Peak:MIC ratio (target >8-10 for gram-negative) |
| Post-antibiotic effect | Several hours - allows once-daily dosing |
| Synergy | With beta-lactams or vancomycin against enterococci, streptococci (important in endocarditis) |
| Toxicity index | AUC/time above threshold - trough >2 mcg/mL predicts toxicity |
| Spectrum | Aerobic gram-negative bacilli (Enterobacteriaceae, Pseudomonas); NOT effective against anaerobes or streptococci (monotherapy) |
Key PD concept: Toxicity is time-dependent (time above threshold concentration), while efficacy is concentration-dependent. This paradox is why once-daily dosing maximizes peak (efficacy) while minimizing time above toxic trough (safety).
6. Mechanisms of Resistance
Three established mechanisms:
-
Enzymatic inactivation (most common clinically) - transferase enzymes modify aminoglycosides by:
- Adenylation (adenylyltransferases - ANTs)
- Acetylation (acetyltransferases - AACs)
- Phosphorylation (phosphotransferases - APHs)
- These act on amino and hydroxyl groups of the drug
-
Impaired entry - mutation/deletion of porin proteins or disruption of the electrochemical gradient (also occurs under anaerobic conditions)
-
Altered 30S ribosomal receptor - mutation or deletion of the target protein
Amikacin advantage: Amikacin has a bulky side chain (HABA - 2-hydroxy-4-aminobutyric acid) that sterically protects most enzymatic modification sites, making it active against many gentamicin-resistant strains.
Plazomicin advantage: Plazomicin is designed to overcome most aminoglycoside-modifying enzyme resistance.
7. Individual Drugs
A. Gentamicin
- Source: Micromonospora purpurea (note: -micin ending)
- Spectrum: Broad gram-negative (E. coli, Klebsiella, Enterobacter, Pseudomonas, Serratia, Proteus); gram-positive synergy (Staph, Enterococcus)
- Indications: Serious gram-negative infections (septicemia, UTI, pneumonia, endocarditis with penicillin, osteomyelitis)
- Dosing (traditional): Peak 5-10 mcg/mL, trough <2 mcg/mL
- Key points:
- Most widely used aminoglycoside
- Activity against Pseudomonas aeruginosa
- Topical use for eye/ear infections
- Synergy with ampicillin for Enterococcus endocarditis
B. Tobramycin
- Source: Streptomyces tenebrarius
- Spectrum: Similar to gentamicin; superior activity against Pseudomonas aeruginosa
- Indications:
- Serious Pseudomonas infections
- Inhaled tobramycin (TOBI) - chronic Pseudomonas infection in cystic fibrosis
- Eye drops for bacterial conjunctivitis
- Key points:
- Drug of choice for CF pulmonary exacerbations
- Similar nephrotoxicity/ototoxicity to gentamicin
- Cross-resistance with gentamicin is common
C. Amikacin
- Source: Semi-synthetic, derived from kanamycin
- Spectrum: Broadest of the aminoglycosides; active against many gentamicin/tobramycin-resistant strains
- Indications: MDR gram-negative infections, nontuberculous mycobacteria (NTM), TB (second-line)
- Dosing: 15 mg/kg once daily; peaks 20-30 mcg/mL, troughs <10 mcg/mL
- Key points:
- Reserved for MDR organisms - do NOT use as first-line to preserve activity
- Also available as inhaled formulation (Arikayce) for NTM lung disease
- Resistant to most aminoglycoside-modifying enzymes due to HABA side chain
D. Streptomycin
- Source: Streptomyces griseus (first aminoglycoside discovered, 1943)
- Spectrum: M. tuberculosis, Francisella tularensis (tularemia), Yersinia pestis (plague), Brucella, Enterococcus (with penicillin)
- Indications:
- Tuberculosis (second-line, in resistant cases or initial intensive phase)
- Plague, tularemia, brucellosis
- Enterococcal and streptococcal endocarditis (with penicillin)
- Streptomycin is still first-line for plague and tularemia
- Key points:
- High rate of resistance in M. tuberculosis now
- Given IM only (no IV formulation widely available)
- Most vestibulotoxic of all aminoglycosides (preferentially damages vestibular apparatus)
E. Neomycin
- Source: Streptomyces fradiae
- Spectrum: Gram-negative enteric organisms, some gram-positives
- Indications:
- Topical only (too toxic for systemic use)
- Pre-operative bowel preparation (oral - not absorbed, sterilizes gut)
- Hepatic encephalopathy (oral - reduces ammonia-producing gut bacteria)
- Triple antibiotic ointments (with polymyxin B and bacitracin)
- Key points:
- Most nephrotoxic and ototoxic aminoglycoside - contraindicated systemically
- Contact dermatitis/sensitization is common with topical use
- Small amounts absorbed orally can cause toxicity if renal failure present
F. Kanamycin
- Source: Streptomyces kanamyceticus
- Spectrum: Gram-negative bacilli; second-line TB activity
- Indications:
- Pre-op bowel sterilization (oral)
- Second-line drug for MDR-TB (now largely replaced by amikacin)
- Limited clinical use
- Key points:
- Cross-resistance with neomycin
- Largely superseded by amikacin in clinical practice
G. Paromomycin
- Source: Streptomyces rimosus
- Unique: Antiparasitic aminoglycoside
- Indications:
- Intestinal amoebiasis (Entamoeba histolytica)
- Giardiasis, Cryptosporidiosis
- Leishmaniasis (parenteral)
- Hepatic encephalopathy (similar to neomycin)
- Key points:
- Not absorbed orally - acts locally in gut
- Only aminoglycoside with significant antiparasitic use
H. Plazomicin (Zemdri)
- Source: Semi-synthetic, derived from sisomicin
- Spectrum: Designed for carbapenem-resistant Enterobacteriaceae (CRE), including KPC-producing strains
- Indications: Complicated UTI and pyelonephritis caused by CRE
- Dosing: 15 mg/kg IV once daily (extended-interval strategy only)
- Key points:
- Newest aminoglycoside approved by FDA
- Designed to overcome most aminoglycoside-modifying enzymes
- Does NOT overcome 16S rRNA methyltransferase resistance
- Reserved for drug-resistant gram-negative infections
8. Adverse Effects
All aminoglycosides are ototoxic and nephrotoxic. These are the most clinically significant adverse effects.
A. Nephrotoxicity
- Mechanism: Aminoglycosides concentrate in renal cortex proximal tubule cells. They bind to phospholipids, cause membrane damage, lysosomal disruption, and proximal tubular cell necrosis.
- Manifestation: Non-oliguric acute kidney injury; rise in serum creatinine; decreased creatinine clearance
- Onset: After 5-7 days of therapy typically
- Risk factors: Pre-existing renal disease, prolonged therapy, high trough levels, advanced age, volume depletion, concurrent nephrotoxins (NSAIDs, amphotericin B, cisplatin, vancomycin), liver disease
- Monitoring: BUN/creatinine regularly; keep troughs <2 mcg/mL (gentamicin/tobramycin) or <10 mcg/mL (amikacin)
- Key point: Usually reversible on discontinuation. ODD (once-daily dosing) is less nephrotoxic.
- Most nephrotoxic: Neomycin > gentamicin = tobramycin > amikacin > streptomycin
B. Ototoxicity
Aminoglycosides accumulate in the endolymph and perilymph of the inner ear, causing irreversible destruction of cochlear hair cells and/or vestibular hair cells.
Two subtypes:
| Type | Affected Drug(s) | Symptom |
|---|---|---|
| Cochleotoxicity (hearing loss) | Amikacin, neomycin, kanamycin | Tinnitus, high-frequency hearing loss (begins with high frequencies, progressing inward) |
| Vestibulotoxicity | Streptomycin, gentamicin | Vertigo, nausea, nystagmus, loss of balance |
- Damage is often irreversible - cochlear hair cells cannot regenerate
- Risk factors: High doses, prolonged therapy, renal failure, pre-existing hearing loss, concurrent ototoxins (loop diuretics - furosemide, ethacrynic acid, cisplatin), genetic susceptibility (mitochondrial 12S rRNA mutations)
- High-frequency hearing loss may go undetected until advanced
- Audiometric monitoring recommended for prolonged courses
C. Neuromuscular Blockade
- Mechanism: Aminoglycosides inhibit presynaptic acetylcholine release and block postsynaptic nicotinic receptors
- Risk: When given rapidly IV or during surgery; enhanced by neuromuscular blocking agents (curare, succinylcholine)
- Manifestation: Acute flaccid paralysis, respiratory arrest
- Treatment: IV calcium gluconate reverses blockade
- Caution: Avoid or use extreme care in myasthenia gravis patients
D. Other Effects
- Hypersensitivity: Rare; contact dermatitis with topical neomycin is common
- Hypomagnesemia: Prolonged therapy causes renal magnesium wasting
- Fetal toxicity: Cross placenta - can cause irreversible VIII nerve damage in fetus (vestibular and cochlear); Category D in pregnancy
- Superinfection: Oral neomycin/kanamycin can cause candidal overgrowth
Summary Table
| Drug | Main Use | Unique Feature | Toxic Preference |
|---|---|---|---|
| Gentamicin | Gram-neg sepsis, endocarditis synergy | Most widely used | Both oto + nephro |
| Tobramycin | Pseudomonas, CF | Best anti-Pseudomonas, inhaled form | Both |
| Amikacin | MDR gram-neg, NTM, TB | Broadest, resistant to modifying enzymes | Cochleotoxic |
| Streptomycin | TB, plague, tularemia | First aminoglycoside | Vestibulotoxic |
| Neomycin | Topical, bowel prep | Most toxic systemically; antiparasitic use | Most nephrotoxic |
| Paromomycin | Amoebiasis, Giardia | Antiparasitic | GI (oral) |
| Plazomicin | CRE infections | Newest; overcomes most resistance | Both |
Sources: Katzung's Basic and Clinical Pharmacology, 16th Edition, pp. 1285-1296; Jawetz Melnick & Adelberg's Medical Microbiology, 28th Edition; Goodman & Gilman's The Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.