Rheumatoid arthritis treatment
Reading File
Finding Sources
Searching PubMed
"rheumatoid arthritis"[MeSH Terms] AND "therapy"[MeSH Terms]
Reading File
Reading File
Searching PubMed
"rheumatoid arthritis" AND "biologic" AND "treatment"
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed to write a comprehensive answer. Let me compile the complete response.
Rheumatoid Arthritis - Treatment
Overview & Goals
RA has no known cure, but modern therapy can achieve remission or low disease activity in the majority of patients when started early and aggressively. The central principle is "treat to target" - continually adjusting therapy until the target (remission or low disease activity, defined by composite scores like DAS-28 or SDAI <3.3) is met.
Keys to optimizing outcomes (Goldman-Cecil Medicine):
- Early, accurate diagnosis
- Early DMARD therapy - all patients should receive a DMARD
- Strive for remission in all patients
- Monitor carefully for treatment toxicities
- Address comorbidities (cardiovascular disease, infection risk, osteoporosis)
Treatment Algorithm
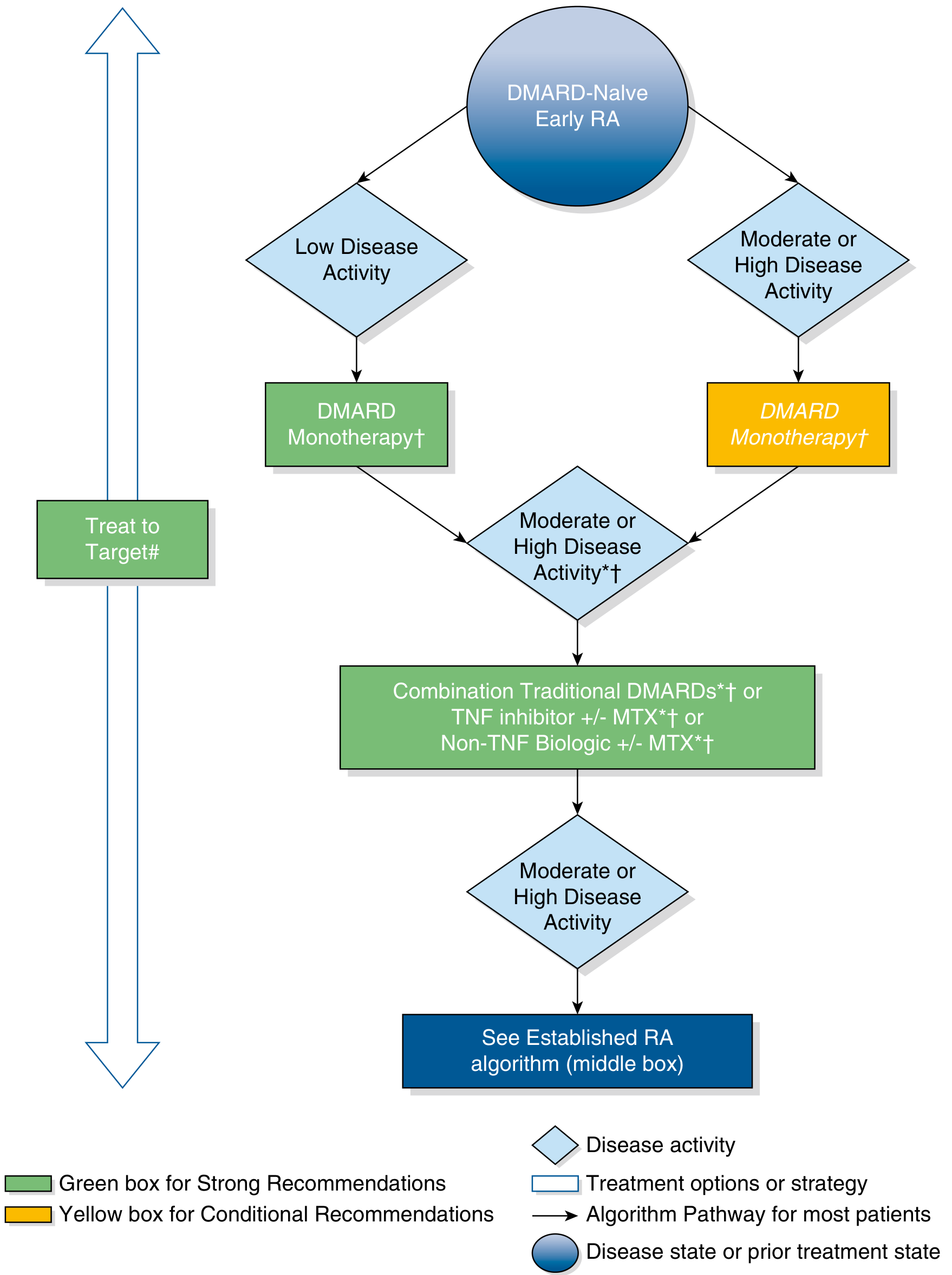
ACR recommendations for early RA: start with DMARD monotherapy, escalate based on disease activity. - Swanson's Family Medicine Review / ACR 2015 Guidelines
The 2021 ACR Guidelines (referenced in Harrison's 22e) updated this by removing the early/established RA distinction and reinforcing treat-to-target with a clear step-up approach:
- Methotrexate monotherapy - first choice for moderate-to-severe RA
- If inadequate response after 3-6 months - step up to:
- Oral triple therapy (MTX + sulfasalazine + hydroxychloroquine), or
- MTX + anti-TNF biologic, or
- MTX + non-TNF biologic
- If still inadequate - switch biologic class or add a targeted synthetic DMARD (JAK inhibitor)
Three Drug Categories
1. NSAIDs
Used for symptomatic relief only - they do not alter the disease course. Should never be used without a concomitant DMARD.
| Drug | Dose |
|---|---|
| Celecoxib (COX-2 selective) | 100 mg twice daily or 200 mg daily |
| Naproxen | 500 mg twice daily |
| Ibuprofen | 400 mg four times daily |
| Diclofenac/misoprostol | 50/200 mg 2-4x daily |
- COX-2 inhibitors cause less GI bleeding but carry cardiovascular risk (especially concerning in RA patients already at elevated CV risk)
- In PRECISION trial, celecoxib was non-inferior to naproxen/ibuprofen for CV outcomes
- Co-prescribe a proton pump inhibitor for GI protection when using NSAIDs
2. Glucocorticoids
Provide rapid, dramatic relief and reduce radiographic progression, but extensive long-term toxicities limit their use.
- Prednisone is most common; rarely exceed 10 mg/day for articular manifestations
- A 25% increased risk of serious infection exists even at 5 mg/day; risk doubles at 5-10 mg/day
- Ideal as a bridge while slower DMARDs take effect (onset 6-12 weeks)
- Goal: taper to zero or minimal dose once DMARDs achieve control
- Higher doses may be needed for extra-articular manifestations (vasculitis, scleritis)
- Prevent glucocorticoid-induced osteoporosis with bisphosphonates (alendronate, risedronate, zoledronic acid), denosumab, or teriparatide based on risk factors
3. DMARDs (Disease-Modifying Antirheumatic Drugs)
All RA patients should receive a DMARD. Three subtypes:
A. Conventional (csDMARDs)
| Drug | Dose | Key Toxicities | Monitoring |
|---|---|---|---|
| Methotrexate (anchor drug) | 7.5-25 mg/week PO or SQ + folic acid 1 mg/day | Hepatotoxicity, myelosuppression, pneumonitis, teratogen | CBC, LFTs, creatinine every 2-3 months |
| Hydroxychloroquine | 200-400 mg/day (≤5 mg/kg) | Irreversible retinal damage, cardiotoxicity | Annual optical coherence tomography + visual fields |
| Sulfasalazine | 500 mg twice daily → 1000-1500 mg/day | Granulocytopenia, hemolytic anemia (G6PD deficiency) | CBC every 2-4 weeks x 3 months, then q3 months |
| Leflunomide | 10-20 mg/day | Hepatotoxicity, myelosuppression, teratogen (Category X) | CBC, LFTs, creatinine every 2-3 months |
| Azathioprine | 1-2.5 mg/kg/day | Myelosuppression | CBC, LFTs |
Methotrexate is the cornerstone DMARD of choice. It is the anchor drug for combination regimens. Its anti-inflammatory effect in RA works partly by stimulating adenosine release.
Oral Triple Therapy (hydroxychloroquine + sulfasalazine + methotrexate): an effective, cost-conscious combination for patients preferring oral agents or with cost concerns. Can be used as initial therapy or as a step-up from methotrexate monotherapy.
Hydroxychloroquine does not delay radiographic progression and is not a "true" DMARD - used for mild/early disease or as adjunctive therapy.
B. Biologic DMARDs (bDMARDs)
First biologics (anti-TNF) approved in 1999. Several classes now available:
Anti-TNF Agents (5 original innovator drugs + multiple biosimilars):
| Drug | Route & Dose |
|---|---|
| Infliximab | 3 mg/kg IV at weeks 0, 2, 6, then every 8 weeks (up to 10 mg/kg q4w) |
| Etanercept | 25 mg SQ twice weekly or 50 mg SQ weekly |
| Adalimumab | 40 mg SQ every 2 weeks |
| Certolizumab pegol | 200 mg SQ every 2 weeks or 400 mg monthly |
| Golimumab | 50 mg SQ monthly |
Non-TNF Biologics:
| Drug | Mechanism | Route & Dose |
|---|---|---|
| Abatacept (CTLA4-Ig) | T-cell co-stimulation blockade | 500-1000 mg IV q4 weeks; or 125 mg SQ weekly |
| Rituximab (anti-CD20) | B-cell depletion | 1000 mg IV x2 doses, 2 weeks apart; repeat every 6-12 months |
| Tocilizumab (anti-IL-6R) | IL-6 receptor blockade | 4-8 mg/kg IV q4 weeks; or 162 mg SQ weekly/q2 weeks |
| Sarilumab (anti-IL-6R) | IL-6 receptor blockade | 200 mg SQ q2 weeks |
| Anakinra (IL-1Ra) | IL-1 receptor antagonist | 100 mg SQ daily |
Key toxicities across all biologics: serious infections (bacterial, fungal, TB reactivation), increased lymphoma risk (controversial), drug-induced lupus (anti-TNF). Screen for latent TB before starting any biologic.
Biosimilars - demonstrated similar efficacy and safety to reference biologics; increasingly used to reduce costs.
Switching strategy: If an anti-TNF fails, consider switching to:
- Another anti-TNF agent, or
- A biologic with a different mechanism of action (e.g., abatacept - evidence suggests this may be more effective than switching anti-TNFs)
C. Targeted Synthetic DMARDs (tsDMARDs) - JAK Inhibitors
Oral small molecules targeting intracellular JAK-STAT signaling pathways. Advantage over biologics: oral administration.
| Drug | JAK Selectivity | Dose |
|---|---|---|
| Tofacitinib | JAK1/JAK3 (minor JAK2/TYK2) | 5 mg twice daily or 11 mg extended-release daily |
| Baricitinib | JAK1/JAK2 (moderate TYK2) | 2 mg or 4 mg daily |
| Upadacitinib | Predominantly JAK1 | 15 mg daily |
Side effects: increased infections (including herpes zoster), elevated liver enzymes, neutropenia, hypercholesterolemia, hypertension, elevated creatinine. Tofacitinib specifically shows increased risk of thrombosis, major adverse cardiovascular events (MACE), and malignancies vs. TNF inhibitors - risk highest in elderly patients. This has influenced regulatory guidance to use JAK inhibitors with caution, particularly in patients over 65, with CV risk, or with malignancy history.
Each JAK inhibitor can be used as monotherapy or in combination with methotrexate.
Multidisciplinary & Non-Pharmacologic Care
- Rheumatologist referral: all RA patients should be evaluated early and followed closely
- Physical therapy: range-of-motion exercises, joint protection techniques
- Occupational therapy: assistive devices, splinting
- Orthopedic surgery: for severe joint destruction (hand surgery, joint replacement)
- Patient education: disease course, treatment importance, self-management
- Treat comorbidities: cardiovascular risk reduction, infection prevention (vaccinations), bone protection
Treatment of Extra-Articular Manifestations
- Aggressive RA control generally improves extra-articular disease
- RA-ILD (interstitial lung disease): challenging because MTX and leflunomide can worsen pulmonary disease. Treat with high-dose corticosteroids + azathioprine, mycophenolate mofetil, or rituximab
- Vasculitis, scleritis: may require higher-dose glucocorticoids
- Cervical spine instability (C1-C2): occurs in 30-40% of RA patients; 5% develop myelopathy - surgical evaluation if symptomatic
- Felty syndrome (late RA): splenomegaly, neutropenia, positive RF - manage underlying RA
Recent Evidence (2024-2025)
- A 2024 network meta-analysis (PMID 39198829) reviewed therapies for difficult-to-treat RA, providing updated head-to-head comparisons of biologics and JAK inhibitors
- A 2024 meta-analysis (PMID 39605094) confirmed biosimilars of etanercept have similar efficacy, safety, and immunogenicity to the reference biologic
- A 2025 systematic review (PMID 40633795) examined combination targeted therapy (dual biologic/tsDMARD), which remains investigational but is gaining evidence in refractory cases
Sources: Harrison's Principles of Internal Medicine 22e (2025), Goldman-Cecil Medicine, Goodman & Gilman's Pharmacological Basis of Therapeutics, Swanson's Family Medicine Review; ACR 2021 Guidelines for RA Treatment
Medicines
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have all the pharmacology detail needed. Here is the comprehensive drug-by-drug breakdown:
Medicines Used in Rheumatoid Arthritis - Detailed Pharmacology
Drug Categories at a Glance
| Category | Role | Onset |
|---|---|---|
| NSAIDs | Symptom relief only | Hours |
| Glucocorticoids | Rapid bridge + symptom control | Hours-days |
| Conventional DMARDs (csDMARDs) | Disease modification | 6-12 weeks |
| Biologic DMARDs (bDMARDs) | Disease modification, targeted | 2-6 weeks |
| Targeted synthetic DMARDs / JAK inhibitors (tsDMARDs) | Oral disease modification | Weeks |
1. NSAIDs
NSAIDs provide symptomatic relief (pain, stiffness, swelling) but do not alter the underlying disease and must never be used as sole therapy.
Mechanism: Inhibit cyclooxygenase (COX-1 and/or COX-2), reducing prostaglandin synthesis and thus inflammation and pain.
| Drug | Dose | Notes |
|---|---|---|
| Celecoxib | 100 mg twice daily or 200 mg daily | COX-2 selective; less GI bleeding but CV risk |
| Naproxen | 500 mg twice daily | Non-selective |
| Ibuprofen | 400 mg four times daily | Non-selective |
| Diclofenac/misoprostol | 50/200 mg 2-4x daily | GI-protective combination |
Key warnings:
- COX-2 selective agents (celecoxib) carry cardiovascular risk - keep dose low in RA patients who already have elevated CV risk
- Co-prescribe a proton pump inhibitor with any NSAID in RA
- NSAIDs reduce renal blood flow and can raise blood pressure
- Low-dose aspirin co-therapy may increase GI toxicity
2. Glucocorticoids
Mechanism: Bind to intracellular glucocorticoid receptors, suppress NF-κB, reduce transcription of inflammatory cytokines (IL-1, IL-6, TNF-α), inhibit phospholipase A2 (blocking arachidonic acid cascade), suppress T-cell and macrophage activation.
| Drug | Dose | Use |
|---|---|---|
| Prednisone | ≤10 mg/day PO | Oral maintenance / bridge |
| Prednisolone | 5 mg/day | Preferred in older patients (>65 yrs) |
| Methylprednisolone | IM depot or IV | Acute flares, infusion pre-medication |
| Triamcinolone | Intra-articular | Localized flare control |
Key points:
- 25% increased risk of serious infection even at 5 mg/day; doubles at 5-10 mg/day
- Goal: taper to zero or lowest effective dose once DMARDs control disease
- Higher doses for extra-articular features (vasculitis, scleritis)
- Osteoporosis prevention: bisphosphonates (alendronate, risedronate, zoledronic acid), denosumab, or teriparatide based on risk profile
3. Conventional DMARDs (csDMARDs)
Methotrexate (MTX) - The Anchor Drug
Mechanism:
- Structurally related to folic acid
- Inhibits dihydrofolate reductase (DHFR) - the enzyme converting folic acid to its active coenzyme tetrahydrofolate (FH4), thereby blocking purine and pyrimidine synthesis
- Inhibition is reversed by leucovorin (folinic acid) or a 1000-fold excess of dihydrofolate
- At low RA doses, MTX also stimulates adenosine release from cells, producing an anti-inflammatory effect (distinct from its anti-proliferative effect in cancer)
- Specific for the S phase of the cell cycle
Dosing:
- 7.5-25 mg once weekly, orally or subcutaneously (not daily - weekly!)
- Folic acid 1 mg/day co-administered to reduce toxicities
Pharmacokinetics:
- Variable oral absorption at low doses; also given IM, IV, SQ
- Distributed to intestinal epithelium, liver, kidney, skin
- Excreted primarily in urine; keep patient well-hydrated and urine alkaline to prevent crystalluria from 7-OH-methotrexate metabolite
Toxicities:
| System | Effect |
|---|---|
| Hepatic | Hepatotoxicity, fibrosis with long-term use |
| Hematologic | Myelosuppression, pancytopenia |
| Pulmonary | Infectious pneumonitis, interstitial lung disease |
| GI | Nausea, diarrhea, stomatitis/mouth ulcers |
| Other | Alopecia, teratogen (Category X) |
Monitoring: CBC, LFTs, creatinine every 2-3 months; viral hepatitis panel; chest X-ray at baseline
Hydroxychloroquine (HCQ)
Mechanism:
- Antimalarial with immunosuppressant properties
- Increases pH of lysosomal and endosomal compartments, suppressing intracellular antigen processing and loading of peptides onto MHC class II molecules
- Decreases T-cell activation
- Does NOT delay radiographic progression - therefore not a "true" DMARD
Dose: 200-400 mg/day orally (≤5 mg/kg to reduce retinal risk)
Use: Early, mild RA; adjunctive in combination (oral triple therapy); SLE
Toxicities:
- Irreversible retinal damage (most feared) - annual optical coherence tomography + visual field testing required
- Cardiotoxicity, blood dyscrasias
- GI upset (nausea, diarrhea), headache, skin discoloration
Monitoring: Annual ophthalmology review; baseline exam if age ≥40 or prior ocular disease
Leflunomide
Mechanism:
- A prodrug, biotransformed to the active metabolite teriflunomide
- Reversibly inhibits dihydroorotate dehydrogenase (DHODH), a mitochondrial enzyme essential for de novo pyrimidine synthesis
- Pyrimidine-starved lymphocytes cannot proliferate - specifically arrests autoimmune lymphocyte activation
- Has both immunomodulatory and anti-inflammatory effects
Dose: 10-20 mg/day orally; start with a loading dose (100 mg/day x 3 days), then maintenance
Key points:
- Active metabolite has a very long half-life (weeks) - once-daily dosing after steady state
- Alternative to MTX when MTX is contraindicated or not tolerated; can combine with MTX for suboptimal responders
- Similar clinical efficacy to MTX
Toxicities:
- Hepatotoxicity (contraindicated in liver disease)
- Teratogen (Category X) - contraindicated in pregnancy; must use cholestyramine washout protocol before conception
- Myelosuppression, alopecia, diarrhea, hypertension
- Low-frequency cardiovascular effects (angina, tachycardia)
Monitoring: CBC, LFTs, electrolytes, creatinine every 2-3 months
Sulfasalazine
Mechanism: Mechanism in RA is unclear; cleaved in the colon to sulfapyridine and 5-aminosalicylic acid; believed to have anti-inflammatory and immunomodulatory effects; reduces radiographic progression
Dose: 500 mg twice daily initially → 1000-1500 mg/day maintenance
Toxicities: GI (nausea, vomiting, anorexia), rash, headache, granulocytopenia, hemolytic anemia (especially in G6PD-deficient patients)
Monitoring: CBC every 2-4 weeks for first 3 months, then every 3 months; check G6PD level before starting
Azathioprine
Mechanism: Purine antimetabolite; converted to 6-mercaptopurine, which inhibits purine synthesis and lymphocyte proliferation
Dose: 1-2.5 mg/kg/day
Use: Reserved for patients who fail other DMARDs or for RA-ILD
Toxicities: Myelosuppression, hepatotoxicity, increased infection risk, GI distress
4. Biologic DMARDs (bDMARDs)
Biologic DMARDs target specific cytokines and cell-surface molecules. Generally used after inadequate response to csDMARDs. Clinical response can appear within 2 weeks.
Class-wide warnings: Serious infections (TB, bacterial, fungal), hepatitis B reactivation. Screen for latent TB before starting any biologic. No live vaccines while on biologics. Do NOT combine two biologics (severe infection risk).
Anti-TNF-α Agents
Pathophysiology rationale: TNF-α is a critical upstream mediator secreted by synovial macrophages; stimulates synovial cell proliferation, collagenase synthesis, cartilage degradation, bone resorption, and inhibits proteoglycan synthesis.
| Drug | Type | Mechanism | Route & Dose | Notes |
|---|---|---|---|---|
| Adalimumab | Fully human mAb | Binds soluble + membrane TNF-α, blocks receptor interaction | 40 mg SQ every 2 weeks | Injection site reactions, headache, agranulocytosis |
| Certolizumab pegol | Pegylated humanized Fab fragment | Neutralizes TNF-α; no Fc portion (reduced placental transfer) | 200 mg SQ q2w or 400 mg monthly | May be safer in pregnancy among anti-TNFs |
| Etanercept | Fusion protein (TNF receptor-IgG1 Fc) | Soluble decoy receptor - binds and sequesters TNF-α | 50 mg SQ weekly (or 25 mg twice weekly) | MTX combination superior to either alone |
| Golimumab | Fully human mAb | Binds TNF-α, blocks receptor | 50 mg SQ monthly (with MTX) | May increase hepatic enzymes |
| Infliximab | Chimeric (human/murine) mAb | Binds soluble + membrane-bound TNF-α | 3 mg/kg IV at 0, 2, 6 weeks then q8w | Must use with MTX to prevent anti-drug antibodies; infusion reactions |
Additional warnings for anti-TNF class: increased risk of lymphoma (controversial), drug-induced lupus, caution/contraindication in moderate-severe heart failure (can worsen CHF)
IL-6 Receptor Antagonists
Pathophysiology rationale: IL-6 drives acute-phase response, synovial inflammation, osteoclast activation, and B-cell differentiation in RA.
| Drug | Mechanism | Route & Dose | Notable AEs |
|---|---|---|---|
| Tocilizumab | Recombinant mAb blocking membrane + soluble IL-6 receptors | 4-8 mg/kg IV q4w or 162 mg SQ weekly/q2w | Elevated LFTs, hyperlipidemia, neutropenia, hypertension, GI perforation |
| Sarilumab | Recombinant mAb blocking IL-6 receptor | 200 mg SQ q2w | Similar to tocilizumab |
Preferred in: patients with heart failure (safer CV profile than TNF inhibitors), elderly patients with frailty
T-Cell Co-stimulation Blocker
Drug: Abatacept (CTLA4-Ig)
Mechanism:
- T lymphocytes require TWO signals for full activation:
- Signal 1: Antigen-MHC complex binds T-cell receptor
- Signal 2 (co-stimulation): CD80/CD86 on antigen-presenting cell binds CD28 on T-cell
- Abatacept is a recombinant fusion protein of CTLA-4 + IgG1 Fc that competitively binds CD80/CD86, blocking the CD28 co-stimulatory signal
- Without signal 2, T-cells become anergic (unresponsive) rather than activated
- Reduces downstream inflammation driven by activated T-cells
Dose: 500-1000 mg IV at 0, 2, 4 weeks then monthly; or 125 mg SQ weekly
Use: After failure of MTX alone; evidence suggests switching to abatacept after TNF failure may be more effective than switching to another anti-TNF
AEs: Infusion reactions, headache, upper respiratory infections, nausea; lower infection risk than TNF inhibitors
Anti-CD20 (B-Cell Depletion)
Drug: Rituximab
Mechanism:
- B-lymphocytes perpetuate RA inflammation by: activating T-lymphocytes, producing autoantibodies and rheumatoid factor, and secreting TNF-α and IL-1
- Rituximab is a chimeric murine/human mAb directed against CD20 antigen on normal and malignant B-lymphocytes
- Results in rapid, sustained B-cell depletion
Dose: 1000 mg IV x 2 infusions, 2 weeks apart; repeat every 16-24 weeks
- Pre-medicate with methylprednisolone + acetaminophen + antihistamine to reduce infusion reactions
Use: After failure of TNF inhibitors; preferred in patients with previous malignancy (compared to TNF inhibitors); RA-ILD
AEs: Infusion reactions (urticaria, hypotension), increased infections, hepatitis B reactivation (screen before use), progressive multifocal leukoencephalopathy (rare)
IL-1 Receptor Antagonist
Drug: Anakinra
Mechanism: Recombinant form of endogenous IL-1 receptor antagonist (IL-1Ra); competitively blocks IL-1α and IL-1β binding to the IL-1 receptor
Dose: 100 mg SQ daily
Notes: Less commonly used than other biologics due to daily injection burden and modest efficacy; useful in Still's disease
5. Targeted Synthetic DMARDs - JAK Inhibitors
Mechanism (class):
- JAK (Janus kinase) family: JAK1, JAK2, JAK3, TYK2
- JAKs transduce signals from cytokine receptors (IL-2, -4, -6, -7, -15, -21, IFN-γ, IL-12, IL-23, hematopoietic growth factors) through the JAK-STAT pathway
- JAK inhibitors block this intracellular signaling, broadly suppressing multiple cytokine pathways simultaneously
- Oral administration - key advantage over injectable biologics
| Drug | JAK Selectivity | Dose | Key Notes |
|---|---|---|---|
| Tofacitinib | JAK1/JAK3 primarily; minor JAK2/TYK2 | 5 mg twice daily or 11 mg extended-release daily | First approved JAK inhibitor for RA; ↑ risk of MACE, thrombosis, malignancies vs. TNF inhibitors (especially elderly >65) |
| Baricitinib | JAK1/JAK2; moderate TYK2 | 2 mg or 4 mg once daily | Thromboembolism risk; also studied in COVID-19 |
| Upadacitinib | Predominantly JAK1 selective | 15 mg once daily | Greater JAK1 selectivity may improve therapeutic index |
Class-wide side effects:
- Serious infections (bacterial, herpes zoster - reactivation is common; consider zoster vaccination before starting)
- Neutropenia, elevated liver enzymes
- Hypercholesterolemia, hypertension
- Elevated serum creatinine
- Venous thromboembolism
Post-marketing safety signal: The ORAL Surveillance trial found tofacitinib associated with higher rates of MACE, malignancies, and thrombosis compared to TNF inhibitors in patients ≥50 years with CV risk factors. This led to regulatory label warnings for the entire JAK inhibitor class (use with caution in elderly, those with CV risk, prior malignancy, or thromboembolism).
Quick Reference: Class-by-Class Contraindications
| Drug/Class | Key Contraindications |
|---|---|
| MTX | Pregnancy, renal/hepatic impairment, alcoholism, immunodeficiency |
| Leflunomide | Pregnancy, hepatic disease |
| Hydroxychloroquine | Pre-existing retinopathy, G6PD deficiency (relative) |
| All biologics | Active serious infection, active TB, live vaccines |
| TNF inhibitors | Moderate-severe heart failure, active malignancy (relative), demyelinating disease |
| Rituximab | Active severe infection, hepatitis B (screen first) |
| JAK inhibitors | Active infection, age >65 + CV risk (caution), thrombophilia, malignancy history |
Sources: Lippincott Illustrated Reviews: Pharmacology, Katzung's Basic & Clinical Pharmacology 16e, Harrison's Principles of Internal Medicine 22e (2025), Goldman-Cecil Medicine, Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.