hernia ( elaborate)
Reading File
Finding Sources
Searching PubMed
"hernia"[MeSH Terms] AND "surgical repair"[MeSH Terms]
Searching Images
hernia types anatomy inguinal femoral umbilical
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is a thorough, well-structured answer on hernias.
Hernia — Comprehensive Overview
Definition
A hernia is the protrusion of any viscus (or part of a viscus) from its normal cavity through an abnormal or congenitally weak opening. In the abdomen, this most commonly means intra-abdominal contents (bowel, omentum, or fat) passing through a defect in the abdominal wall musculature or peritoneum.
— Roberts and Hedges' Clinical Procedures in Emergency Medicine
Epidemiology
- Hernias develop in approximately 5% of men and 2% of women
- 75% of all hernias occur in the groin (inguinal/femoral)
- In children and young adults, the majority are indirect inguinal hernias of congenital origin
- Direct hernias are acquired and become more prevalent with aging
- Incisional hernias complicate up to 20% of abdominal surgeries
Anatomy of Hernia Types
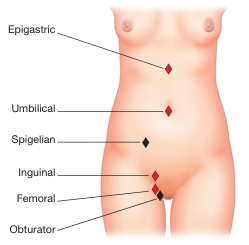
1. Inguinal Hernia (most common — ~75% of all hernias)
Located within the inguinal triangle (bounded by: inguinal ligament inferiorly, inferior epigastric artery superolaterally, lateral edge of rectus abdominis medially).
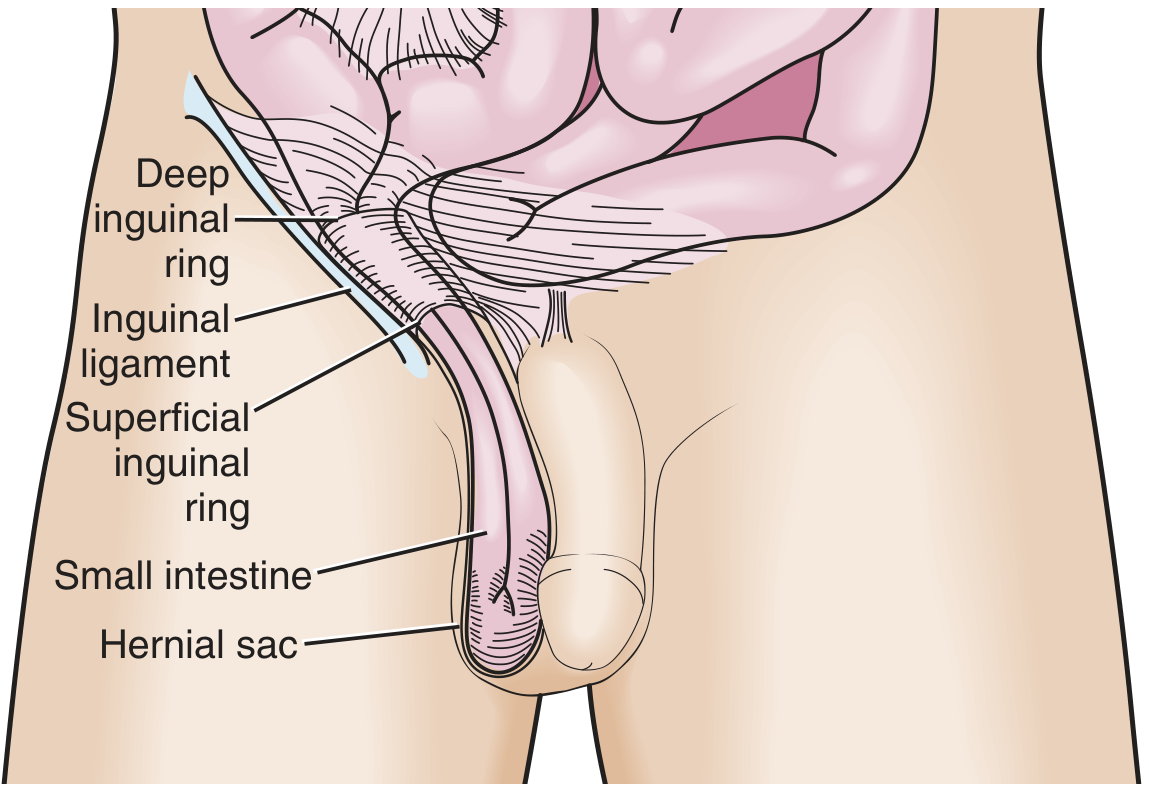
a) Indirect Inguinal Hernia
- Passes through the internal (deep) inguinal ring → travels down the inguinal canal → exits the external (superficial) ring → may enter the scrotum
- Runs lateral to the inferior epigastric artery
- Usually congenital: due to a patent processus vaginalis that fails to close
- Most common in children and young men; can occur at any age
- Physical exam: hernia contents strike the tip of the examining finger when palpating the canal
b) Direct Inguinal Hernia
- Protrudes directly through the posterior wall of the inguinal canal (Hesselbach's triangle), medial to the inferior epigastric artery
- Acquired — caused by weakness of the transversalis fascia from aging, heavy lifting, or increased intra-abdominal pressure
- More common in older men
- Exam: hernia contents push against the volar pad of the finger; pressure over the internal ring after reduction does NOT prevent recurrence on Valsalva (unlike indirect)
c) Pantaloon Hernia
- A combination of both direct and indirect hernias straddling the inferior epigastric artery — difficult to diagnose clinically, often found at surgery.
2. Femoral Hernia
- Protrudes inferior to the inguinal ligament through a defect in the transversalis fascia
- Contents enter the femoral canal — the space medial to the femoral vein and lateral to the lacunar ligament
- Presents as a medial thigh mass below where inguinal hernias are seen
- More common in women
- Has a narrow neck → high risk of incarceration: up to 45% are strangulated at presentation — the most dangerous groin hernia
3. Umbilical Hernia
- Traverses the fibrous umbilical ring
- In adults: acquired; associated with obesity, ascites, multiparity, and raised intra-abdominal pressure
- In neonates: usually closes spontaneously within 1–2 years
- Accounts for ~15% of emergency hernia surgery; up to 60% show strangulation at operation
4. Epigastric Hernia
- Through the linea alba above the umbilicus
- Usually contains pre-peritoneal fat; may be multiple
- Commonly tender and small
5. Incisional / Ventral Hernia
- Occurs at or near a previous surgical scar
- Complicates up to 20% of laparotomies; risk increased by wound infection, obesity, malnutrition, steroid use
- Recurrence rate after repair: 20–50%
- Larger defects paradoxically have lower incarceration risk (wide neck)
6. Spigelian Hernia
- Occurs along the lateral border of the rectus abdominis, just below the arcuate line
- Often occult — contents pass between muscle layers and may not be visible on surface exam
- CT is frequently required for diagnosis
7. Hiatal Hernia
- Herniation of the stomach (or other abdominal contents) through the esophageal hiatus of the diaphragm
- Type I (Sliding): The gastroesophageal junction slides into the chest — most common; strongly associated with GERD
- Type II (Rolling/Paraesophageal): The gastric fundus herniates alongside the esophagus; GEJ remains in place — risk of gastric volvulus
- Types III & IV: Mixed or large, containing multiple organs
- Mechanisms promoting GERD: reduced LES pressure, loss of intra-abdominal LES segment, enlarged "acid pocket" above the diaphragm, increased transient LES relaxations
8. Internal Hernias
- Congenital: Paraduodenal (most common congenital type), foramen of Winslow, transmesenteric
- Acquired/Iatrogenic: After Roux-en-Y gastric bypass, colectomy, Whipple procedure — bowel herniates through mesenteric defects
- Often only diagnosed at laparotomy
9. Other Rare Hernias
| Type | Location | Notes |
|---|---|---|
| Richter hernia | Any location | Only part of the bowel wall is trapped — can strangulate without complete obstruction |
| Obturator hernia | Obturator canal | Elderly women; Howship-Romberg sign (medial thigh pain) |
| Lumbar hernia | Petit/Grynfeltt triangles | Posterior abdominal wall |
| Paraduodenal hernia | Left > right | Congenital; most common internal hernia |
| Parastomal hernia | Around a stoma | Complicates up to 50% of stomas |
Classification by Reducibility
| State | Definition | Management |
|---|---|---|
| Reducible | Contents return to cavity spontaneously or manually | Elective outpatient repair |
| Incarcerated | Contents irreducible without surgery; blood supply intact | Urgent (not always emergency) surgical repair |
| Strangulated | Incarcerated + compromised blood supply → ischemia/necrosis | Surgical emergency |
Key principle: smaller neck = greater risk of strangulation. Femoral and umbilical hernias have the highest strangulation rates; large incisional hernias have the lowest.
Etiology and Risk Factors
Congenital factors:
- Patent processus vaginalis → indirect inguinal hernia
- Developmental defects in abdominal wall musculature
Acquired factors:
- Aging and loss of tissue elasticity
- Raised intra-abdominal pressure: chronic cough (COPD), constipation, straining (BPH), obesity, pregnancy, ascites, heavy lifting
- Failure of wound healing: infection, malnutrition, steroids, diabetes
- Collagen disorders (Marfan, Ehlers-Danlos)
Clinical Features
Symptoms
- Reducible hernia: intermittent bulge that appears on straining/standing, disappears on lying down; often painless
- Incarcerated hernia: non-reducible lump; constant dull ache; signs of bowel obstruction (nausea, vomiting, distension, obstipation)
- Strangulated hernia: severe local pain, tender, erythematous skin overlying; systemic sepsis (fever, tachycardia); peritonitis
Physical Examination (Groin Hernia)
- Examine in both standing and supine positions
- In males: invaginate scrotal skin and palpate inguinal canal; ask patient to cough or Valsalva
- Indirect vs. direct distinction:
- Indirect: starts lateral to inferior epigastric vessels; tip of finger impulse; occlusion of internal ring prevents recurrence
- Direct: medial to epigastric vessels; pad of finger impulse; internal ring occlusion doesn't prevent bulge
- A hernia descending into the scrotum is almost always indirect
Investigations
- Diagnosis is clinical in most cases
- Ultrasound: useful for groin hernias, especially in obese patients or equivocal examination; sensitivity ~86%
- CT scan: investigation of choice for suspected internal hernias, occult hernias (e.g., Spigelian), assessing complications (strangulation — bowel wall thickening, fat stranding, fluid within sac), and preoperative planning for large incisional hernias
- MRI: occasionally used for athletic pubalgia / groin pain differentiation
- Plain X-ray: may show dilated bowel loops in obstruction
Complications
- Incarceration — irreducibility; may lead to obstruction
- Strangulation — ischemia → gangrene; up to 75% of hernias causing SBO have intestinal ischemia; >25% have intestinal necrosis at surgery
- Bowel obstruction — hernias are second only to adhesions as causes of small bowel obstruction in Western countries
- Recurrence — after primary repair (tissue repairs: higher rate; mesh repairs: lower rate)
- Haematoma / seroma
- Wound infection — especially with mesh
- Chronic groin pain — ilioinguinal/iliohypogastric/genitofemoral nerve injury
Emergency Management (ED)
Assessment Priorities
- Is the mass truly a hernia?
- Is it reducible, incarcerated, or strangulated?
- Is there bowel obstruction?
Manual Reduction (Taxis)
- Appropriate for incarcerated but non-strangulated hernias
- Position patient supine with hips slightly flexed (Trendelenburg)
- Apply gentle, sustained pressure directed toward the defect — do NOT use excessive force
- More reliable for groin and umbilical hernias than large incisional defects
- Contraindications: fever, skin erythema, severe tenderness, systemic signs of strangulation — these require urgent surgical referral, not reduction attempts
Strangulated Hernia (Surgical Emergency)
- IV access, fluid resuscitation, NBM
- IV antibiotics (cover gram-negative and anaerobes)
- Urgent surgical consultation → laparotomy or laparoscopy; bowel resection if necrotic; hernia repair
Surgical Management
Principles
- Elective repair is preferred (lower morbidity, better outcomes than emergency repair)
- Emergency repair carries significantly higher rates of short-term complications and recurrence
Techniques
Open Tissue Repair (Non-mesh)
- Shouldice repair: multi-layer imbrication of the posterior inguinal wall; recurrence ~1–2% in expert hands
- Bassini repair: classical; less used now
- Preferred in contaminated fields (strangulation, bowel resection) where mesh infection risk is high
Open Mesh Repair
- Lichtenstein tension-free repair: mesh sutured to inguinal ligament and conjoint tendon; standard for elective inguinal hernia
- Plug-and-patch and other variants exist
- Mesh significantly reduces recurrence rates compared to tissue repairs
Laparoscopic Repair
- TAPP (Trans-Abdominal Pre-Peritoneal): mesh placed in pre-peritoneal space via intra-abdominal approach; excellent visualization of triangle of doom (external iliac vessels) and triangle of pain (femoral/lateral cutaneous nerve)
- TEP (Totally Extra-Peritoneal): pre-peritoneal dissection without entering peritoneal cavity; avoids intra-abdominal complications
- Benefits: less post-operative pain, faster return to activity, lower chronic pain rates, better for bilateral or recurrent hernias
Mesh Use in Emergency
- In emergency hernia repair with contamination or bowel resection, tissue repair is preferred (mesh infection risk); mesh deferred to later stage if recurrence occurs
- Without contamination, mesh can be used with acceptable outcomes
Special Considerations
- Hiatal hernia: managed with proton pump inhibitors (medical); surgery (Nissen fundoplication ± mesh hiatal cruroplasty) for symptomatic paraesophageal or failed medical therapy
- Incisional hernia: component separation techniques for large defects; biologic meshes in contaminated fields
- Parastomal hernia: difficult to manage; mesh repair via laparoscopic Sugarbaker technique or open repair
Summary Table
| Hernia | Location | Sex preference | Key feature | Strangulation risk |
|---|---|---|---|---|
| Indirect inguinal | Above inguinal lig., through deep ring | M >> F | Congenital; enters scrotum | Moderate |
| Direct inguinal | Above inguinal lig., Hesselbach's triangle | M >> F | Acquired; older men | Low |
| Femoral | Below inguinal lig., femoral canal | F > M | Narrow neck; medial thigh mass | Very high (45%) |
| Umbilical | At umbilicus | F > M (adults) | Self-resolves in neonates | High (60% at operation) |
| Incisional | At surgical scar | Equal | Post-surgical; 20% of laparotomies | Lower with large defect |
| Spigelian | Lateral rectus border | Equal | Often occult; needs CT | Moderate |
| Epigastric | Linea alba, above umbilicus | M > F | Small, fat-containing | Low |
| Hiatal | Esophageal hiatus | F > M (older) | Associated with GERD | Low (volvulus risk) |
| Richter | Any narrow orifice | Variable | Partial wall entrapment; no full obstruction | High |
Sources:
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, Chapter 44
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chapters 46 & 123
- Mulholland and Greenfield's Surgery: Scientific Principles and Practice, 7e, Chapter 49
- Bailey and Love's Short Practice of Surgery, 28th Edition
This is a shared conversation. Sign in to Orris to start your own chat.