Q. Clinical features, Diagnosis and management of Otosclerosis. in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances
Reading File
search_medical_text
otosclerosis clinical features diagnosis pathology histology
search_medical_text
otosclerosis management surgery stapedectomy stapedotomy treatment
search_medical_image
otosclerosis audiogram tympanogram surgical diagram stapedectomy
GradeResponse
GradeResponse
GradeResponse
search_medical_image
otosclerosis fissula ante fenestram HRCT temporal bone halo sign
GradeResponse
Figure 1: HRCT Temporal Bone — Otosclerosis Stages
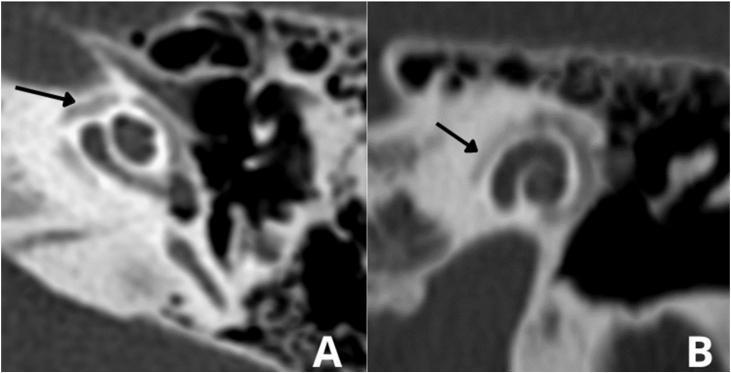
Figure 1: Axial HRCT temporal bone. Panel A: Fenestral otosclerosis — hypodense focus at fissula ante fenestram (arrow) indicating active otospongiosis. Panel B: Cochlear/retrofenestral otosclerosis — the classic "double ring / halo sign" (arrow) encircling the cochlea from otic capsule demineralization. (Source: PMC Clinical VQA)
Figure 2: Intraoperative Stages of Stapedectomy/Stapedotomy
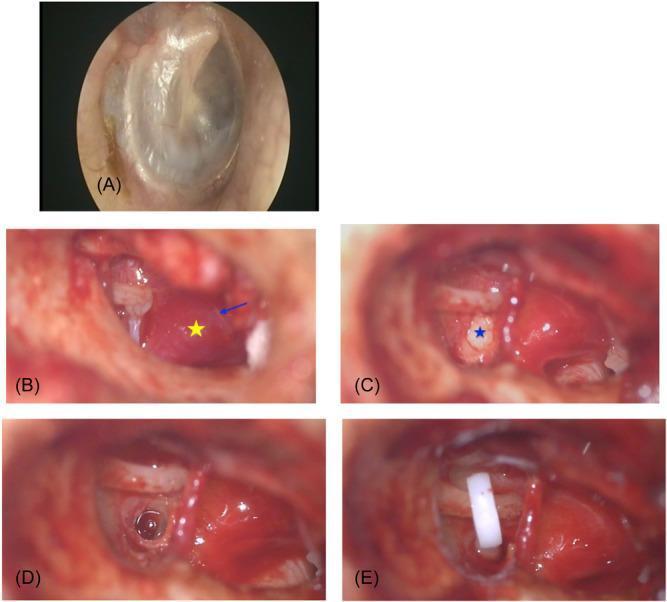
Figure 2: Intraoperative otoendoscopic and microscopic series. (A) Normal tympanic membrane pre-operatively. (B) After tympanomeatal flap elevation: Schwartze sign (reddish vascular blush over promontory — yellow star); Jacobson's nerve (blue arrow). (C) Otosclerotic stapes footplate — white, thickened, sclerotic (blue star). (D) Stapedotomy: circular perforation created in footplate. (E) Final prosthesis placement — white Teflon piston connecting incus long process to stapedotomy site. (Source: PMC Clinical VQA)
15. RECENT ADVANCES IN OTOSCLEROSIS
15.1 Genetic and Molecular Advances
- Whole exome sequencing identifying novel OTSC loci
- COL1A1 polymorphisms (Sp1 binding site) confirmed as risk factor in multiple GWAS
- TGF-β1 as therapeutic target — anti-TGF-β therapy experimental
- RANKL/OPG pathway imbalance identified → bisphosphonate rationale
15.2 Imaging Advances
- Cone Beam CT (CBCT): Lower radiation dose; comparable to HRCT for fenestral otosclerosis
- MRI with gadolinium (3T): "Enhancement halo" on T1 post-Gd in active cochlear otosclerosis
- Quantitative CT densitometry: Measuring otic capsule density to grade activity
- Diffusion-weighted MRI: Research role in distinguishing active vs. inactive foci
15.3 Surgical Advances
- Robotic/Semi-robotic micromanipulators: Sub-millimeter precision in stapedotomy
- Shape-memory alloy (Nitinol) prostheses: Self-crimping; no manual crimping needed; reduced incus necrosis
- 3D-printed custom prostheses: Patient-specific geometry
- Endoscopic Ear Surgery (EES): Transcanal fully endoscopic stapedotomy — growing standard of care
- Laser advancements: CO₂ laser with microtargeting; pulsed mode reducing thermal spread
- Intraoperative monitoring: Cochlear microphonics, laser-Doppler vibrometry for real-time footplate assessment
15.4 Pharmaceutical Advances
- Bisphosphonates (alendronate/etidronate): Phase II trials in cochlear otosclerosis; comparable to NaF in slowing SNHL
- Anti-measles vaccination: Population-level data showing declining incidence in vaccinated cohorts
- Intratympanic steroids: Experimental for cochlear preservation in mixed otosclerosis
15.5 Cochlear Implantation Advances
- Hybrid/EAS (Electric-Acoustic Stimulation): For patients with residual low-frequency hearing + high-frequency SNHL from cochlear otosclerosis
- Scala vestibuli CI insertion in obliterated scala tympani
- Drill-out procedures with simultaneous CI
(Scott-Brown's 8th Ed.; Cummings 7th Ed.; Eur Arch Otorhinolaryngol 2022; Otol Neurotol 2021)
16. PROGNOSIS
| Scenario | Prognosis |
|---|---|
| Fenestral otosclerosis treated surgically | Excellent (90–95% success) |
| Cochlear otosclerosis on NaF | Stabilization in 75–80% |
| Re-operation (revision stapedectomy) | 70–80% success |
| CI in cochlear otosclerosis | Good (slightly inferior to other etiologies) |
| Untreated bilateral disease | Progressive bilateral mixed hearing loss |
17. SUMMARY FLOWCHART — COMPLETE MANAGEMENT
PATIENT WITH PROGRESSIVE BILATERAL CHL + NORMAL TM
│
▼
TUNING FORK TESTS
Rinne: –ve Weber: lateralizes to worse ear
Gellé: –ve ABC: Equal to examiner
│
▼
PURE TONE AUDIOMETRY
CHL / Mixed HL + Carhart's Notch at 2 kHz
ABG ≥ 30 dB
│
▼
IMPEDANCE AUDIOMETRY
Type As tympanogram + Absent stapedial reflexes
│
▼
OTOSCOPY: Normal TM
± Schwartze sign (if active)
│
▼
HRCT TEMPORAL BONE
Fenestral / Cochlear staging
Assess footplate, obliteration
│
▼
┌────────────────────────────────┐
│ OTOSCLEROSIS CONFIRMED │
└────────────────────────────────┘
│
┌────────────┴─────────────┐
│ │
FENESTRAL COCHLEAR / MIXED
ABG ≥ 30 dB OTOSCLEROSIS
Good cochlear reserve ± SNHL
│ │
▼ ▼
SURGERY Sodium Fluoride
Stapedotomy + Ca + Vit D
(preferred) Consider CI if
± Laser severe SNHL
│
▼
POST-OP AUDIOGRAM
Success: ABG ≤ 10 dB
Speech discrimination ≥ 70%
│
┌──────┴──────────┐
│ │
SUCCESS FAILURE
│ │
▼ ▼
Monitor HA / Revision
Annually Stapedectomy /
Consider CI
18. TEXTBOOK REFERENCES
| Textbook | Key Chapters/Pages |
|---|---|
| Cummings Otolaryngology — Head and Neck Surgery, 7th Ed. | Chapter 144: Otosclerosis |
| Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th Ed. | Vol 3, Ch 233: Otosclerosis |
| Dhingra — Diseases of ENT, Head & Neck Surgery, 7th Ed. | Chapter 10: pp. 80–90 |
| Hazarika — Textbook of ENT & Head-Neck Surgery, 3rd Ed. | Chapter: Otosclerosis |
| Zakir Hussain — Textbook of ENT | Ch: Otosclerosis, CHL |
| Stell & Maran's — Head and Neck Surgery, 5th Ed. | Chapter: Otosclerosis |
| Harrison's Principles of Internal Medicine, 21st Ed. | p. 1042: Hearing Disorders |
| Glasscock-Shambaugh Surgery of the Ear, 6th Ed. | Chapter: Stapedectomy |
KEY POINTS FOR EXAM (50-Mark Summary)
- Otosclerosis = focal otic capsule bony remodeling; unique to humans; predominantly whites, F>M, autosomal dominant (25–40% penetrance)
- Most common site: fissula ante fenestram (anterior to oval window)
- Histopathology: Blue mantles of Manasse; vascular stromal spaces (otospongiosis = active; otosclerosis = inactive)
- Clinical hallmarks: Progressive CHL, normal TM, Paracusis Willisii, Rinne –ve, Gellé –ve, Schwartze sign (10% active)
- Audiometry: CHL + Carhart's notch at 2 kHz + Type As tympanogram + absent stapedial reflex
- HRCT: Fenestral hypodense focus + halo/double-ring sign (cochlear type)
- Surgery of choice: Stapedotomy (small fenestra, 0.6–0.8 mm) with Teflon-platinum piston prosthesis
- Laser stapedotomy: Gold standard in obliterative disease
- Success rate: 90–95% (ABG ≤ 10 dB); dead ear risk: 0.3–1%
- Medical: NaF for active/cochlear disease; bisphosphonates (emerging)
- CI: For bilateral profound SNHL; challenges include ossified cochlea
- Van der Hoeve syndrome: Otosclerosis + blue sclera + brittle bones
- Recent advances: Endoscopic EES, nitinol prostheses, laser robotics, shape-memory alloys, anti-TGF-β therapy, GWAS genetics
Compiled from: Scott-Brown's Otorhinolaryngology 8th Ed., Cummings Otolaryngology 7th Ed., Dhingra Diseases of ENT 7th Ed., Hazarika Textbook of ENT 3rd Ed., Zakir Hussain Textbook of ENT, Stell & Maran's Head and Neck Surgery, Harrison's Principles 21st Ed. (p. 1042), Glasscock-Shambaugh Surgery of the Ear, and recent literature (Otol Neurotol, Eur Arch Otorhinolaryngol, Laryngoscope, 2019–2023).
This is a shared conversation. Sign in to Orris to start your own chat.