Write diagnostic methods for amyloidosis in clinical storyy from
Reading File
Finding Sources
Finding Sources
Searching PubMed
amyloidosis diagnosis biopsy imaging biomarkers
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed. Let me compose the comprehensive clinical story on diagnostic methods for amyloidosis.
Diagnostic Methods for Amyloidosis: A Clinical Story
The Clinical Presentation - Raising Suspicion
A 68-year-old man, Mr. Harrison, presents to the cardiology clinic with a 6-month history of progressive exertional dyspnea, bilateral ankle edema, and unintentional weight loss of 8 kg. His GP had noted proteinuria on routine urinalysis. On examination his blood pressure is surprisingly low at 95/60 mmHg despite biventricular heart failure signs - elevated JVP, hepatomegaly, and pitting edema to the knees. His ECG shows a low-voltage pattern discordant with the echo finding of markedly increased left ventricular wall thickness. He has a history of bilateral carpal tunnel syndrome, treated surgically 3 years prior.
This constellation - HFpEF with low blood pressure, increased wall thickness without matching ECG voltage, proteinuria, carpal tunnel syndrome, and peripheral neuropathy - immediately raises the flag for systemic amyloidosis.
"Amyloidosis should be considered in any patient with suggestive presentations, including heart failure with preserved ejection fraction, albuminuria, or peripheral neuropathy, particularly if a monoclonal gammopathy is present."
- Comprehensive Clinical Nephrology, 7th Edition
Step 1: Blood and Urine Screening
Before reaching for a biopsy needle, the team orders targeted screening tests.
Haematology / Plasma Cell Dyscrasia Screen
- Serum free light chain (FLC) assay - abnormal kappa/lambda ratio
- Serum protein electrophoresis (SPEP) with immunofixation - detects M-protein
- Urine immunofixation - Bence Jones protein
Mr. Harrison's serum FLC shows a markedly elevated lambda light chain with a reversed ratio, and immunofixation of serum and urine confirms a lambda monoclonal protein. This raises strong suspicion for AL (light chain) amyloidosis.
Cardiac Biomarkers
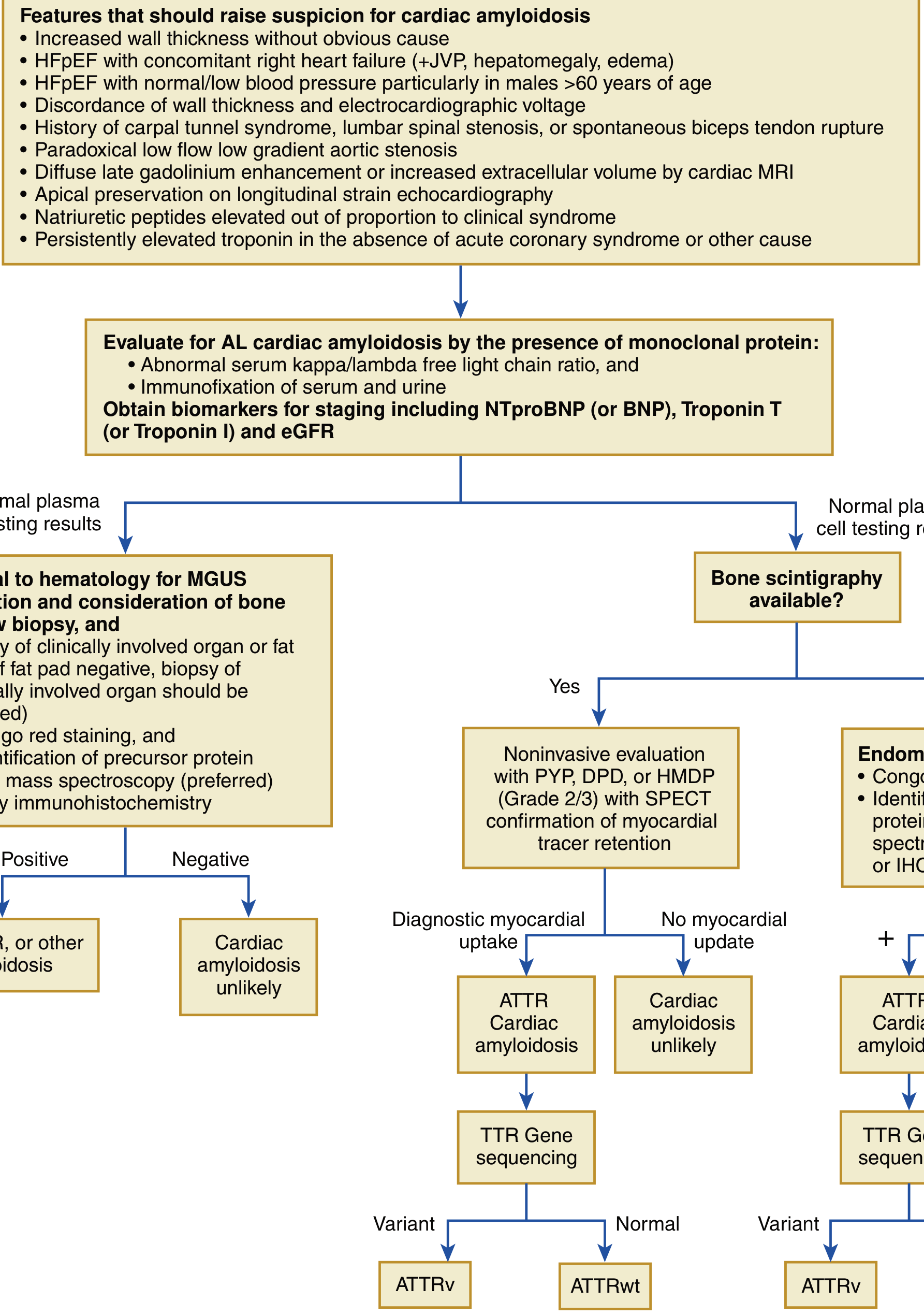
Per the Braunwald/Fuster diagnostic algorithm, all suspected cardiac amyloidosis patients should have:
- NT-proBNP / BNP - elevated out of proportion to the apparent clinical syndrome
- Troponin T or Troponin I - persistently elevated in the absence of acute coronary syndrome
- eGFR (for staging)
These biomarkers serve double duty: they confirm cardiac involvement and stage prognosis. Troponin is a powerful independent predictor of survival in amyloidosis. - Goldman-Cecil Medicine
Step 2: Cardiac Imaging
Echocardiography
The echo report reads: biventricular hypertrophy with a "sparkling" granular appearance of the myocardium, diastolic dysfunction (Grade III), biatrial enlargement, and a small pericardial effusion. Longitudinal strain imaging shows the classic "apical sparing" pattern - reduced strain in the basal segments with relative preservation at the apex - which is highly characteristic of cardiac amyloidosis.
Key red-flag echo features:
- Increased wall thickness without obvious cause
- HFpEF + right heart failure
- Discordance between wall thickness and ECG voltage
- Apical sparing on longitudinal strain mapping
- Small pericardial effusion
Cardiac MRI (CMR)
CMR with gadolinium contrast reveals diffuse late gadolinium enhancement (LGE) in a characteristic subendocardial circumferential pattern, along with increased extracellular volume (ECV) - both hallmarks of amyloid infiltration. CMR is also useful for quantifying the extent of myocardial involvement and tracking response to therapy.
Bone Scintigraphy (99mTc-PYP / DPD Scan)
Given the possible ATTR component, the team orders a technetium-99m pyrophosphate (PYP) scan (US) or DPD/HMDP scan (Europe). This radionuclide test has:
- Sensitivity >99% and specificity ~86% for cardiac ATTR amyloidosis
- Grade 2 or 3 myocardial uptake (equal to or greater than bone uptake) with SPECT confirmation = diagnostic of ATTR cardiomyopathy
However, since Mr. Harrison has a monoclonal protein, a positive scan alone is insufficient - it cannot distinguish between ATTR and AL amyloidosis on scintigraphy alone. Tissue diagnosis is still required.
"ATTRwt is the only type of amyloid that can be made without a tissue diagnosis. When a monoclonal protein is present, however, confirmation of the type of amyloid requires analysis of the Congo red-positive tissues by mass spectrometry or immunoelectron microscopy."
- Goldman-Cecil Medicine
The diagnostic algorithm from Braunwald's Heart Disease:
Step 3: Tissue Biopsy - The Gold Standard
"Histology is the gold standard for the diagnosis of amyloidosis, with the demonstration of the presence of amyloid deposits by apple green birefringence when the tissue biopsy is stained with the aniline dye Congo red and viewed under cross-polarized light."
- Firestein & Kelley's Textbook of Rheumatology
3a. Non-Invasive Screening Biopsies (First Line)
Whenever possible, less invasive sites are sampled first:
| Site | Sensitivity | Notes |
|---|---|---|
| Abdominal fat pad aspirate (AFPA) | ~75% | Simple, office procedure, FNA technique |
| Minor salivary gland biopsy | ~75% | Outpatient, from lower lip |
| Rectal biopsy | ~70% | Submucosa must be sampled |
| Bone marrow biopsy | ~50-60% | Often performed concurrently for plasma cell assessment in AL |
The fat pad aspirate is simple and underutilized. A negative result does not exclude amyloidosis - amyloid deposits may be patchy and Congo red sensitivity depends on adequate tissue, correct processing, and experienced observers. - Comprehensive Clinical Nephrology, 7th Ed.
In Mr. Harrison's case, the abdominal fat pad aspirate is performed - the smear is stained with Congo red.
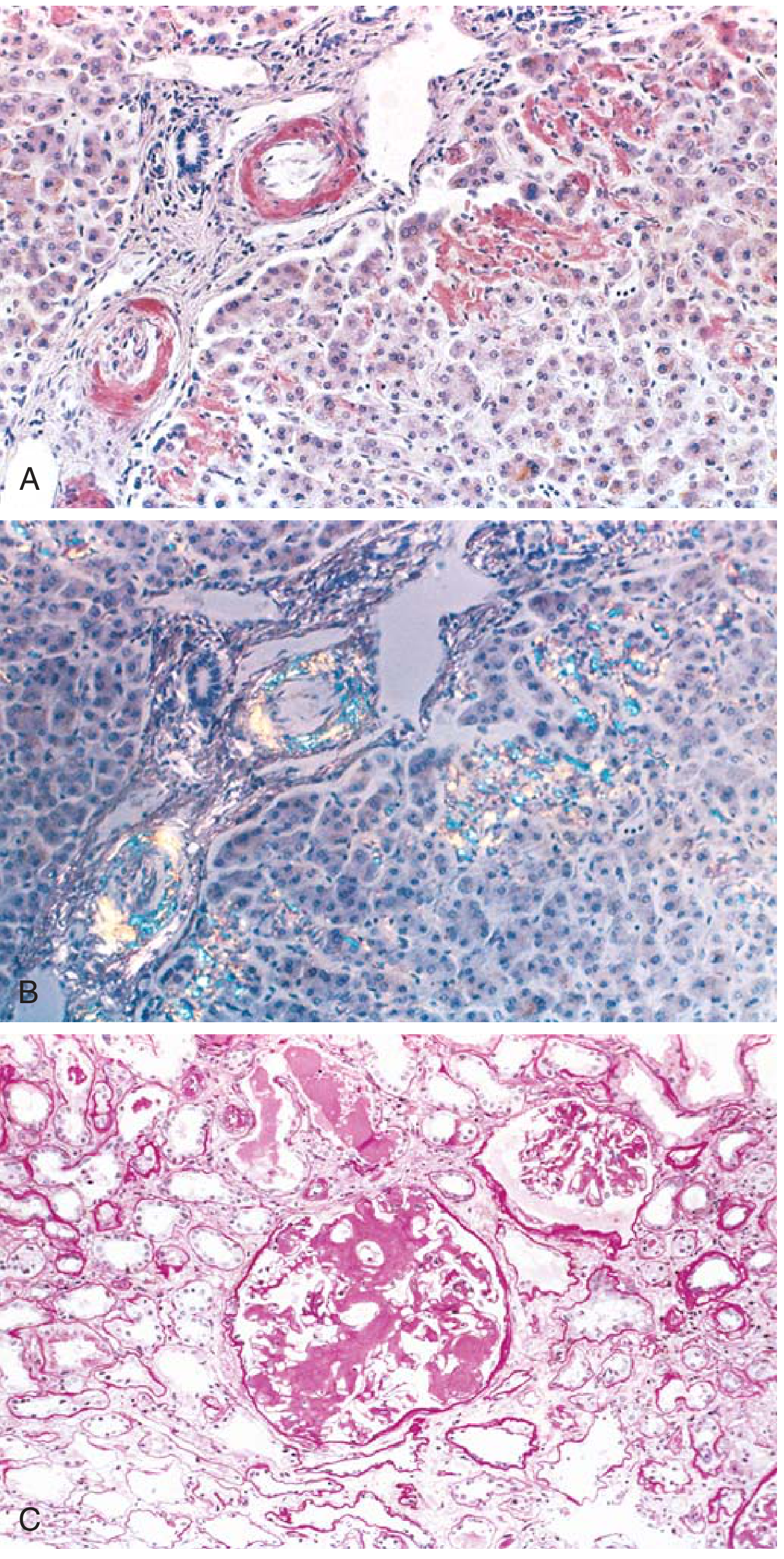
3b. Tissue Staining - Reading the Congo Red
Under ordinary light microscopy (H&E stain), amyloid appears as an amorphous, eosinophilic, hyaline, extracellular substance. This can be confused with collagen or fibrin.
Congo red staining is the definitive histochemical test:
- Routine light microscopy: deposits appear pink-orange/red
- Polarized light microscopy: the pathognomonic apple-green birefringence - diagnostic for all types of amyloid
This staining reaction is conferred by the crossed beta-pleated sheet configuration of amyloid fibrils, which is shared by all types regardless of precursor protein. - Robbins & Kumar Basic Pathology
Other staining properties of amyloid:
- Weakly PAS-positive, diastase-resistant
- Crystal violet: purple metachromatically
- Thioflavin T/S: fluorescent yellow-green under UV
Pitfall: Congo red staining can be falsely negative if tissue sections are less than 5 µm thick. A negative result on a thin section does not exclude amyloidosis.
3c. Organ-Specific (Invasive) Biopsy
If screening biopsies are negative or inconclusive, biopsy of the clinically affected organ is performed. In Mr. Harrison's case, given heavy proteinuria (7 g/day), a kidney biopsy is obtained.
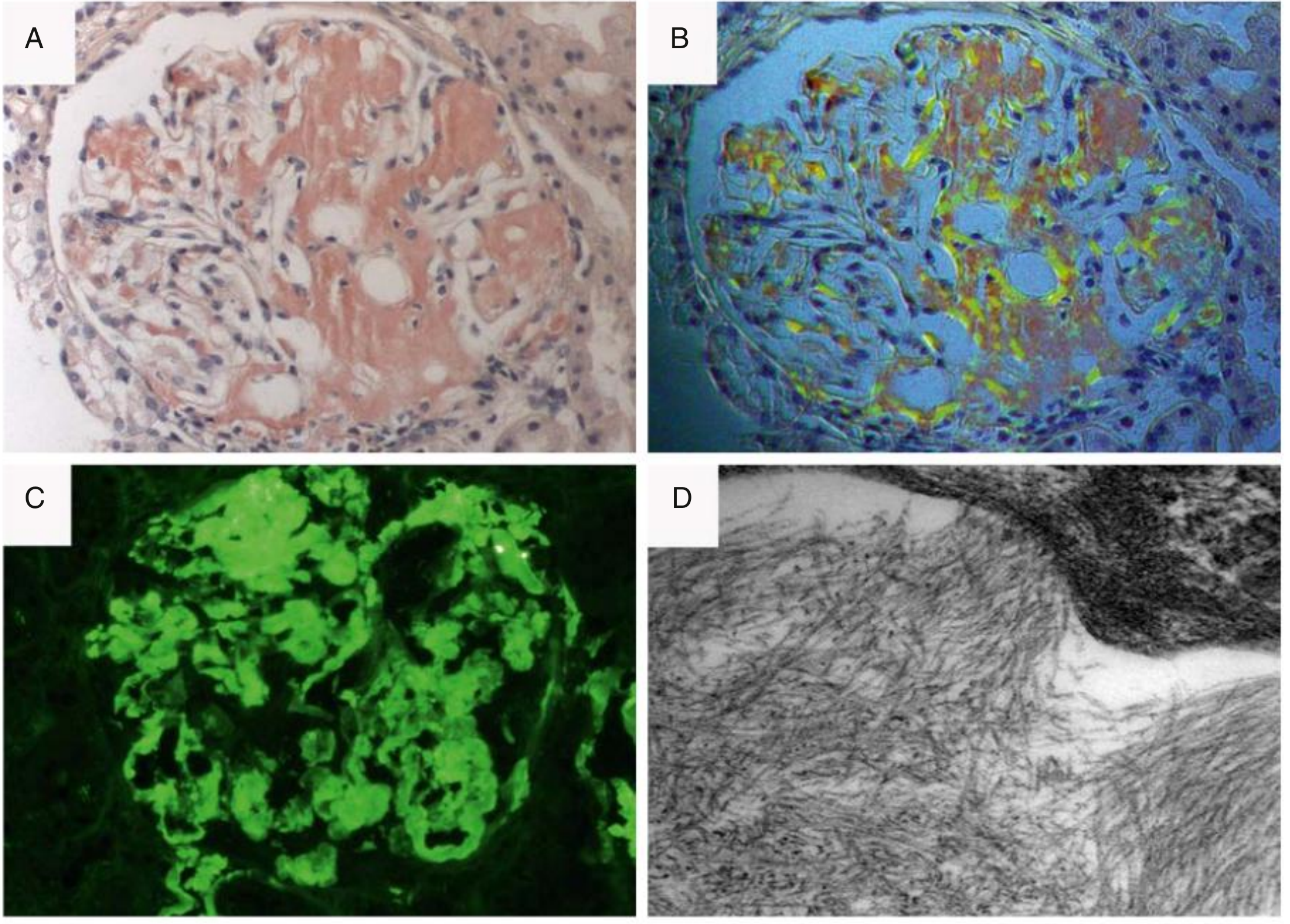
The renal biopsy reveals:
- Light microscopy: extracellular eosinophilic deposits in the mesangium and along glomerular basement membranes - Congo red positive
- Polarized light: apple-green birefringence (see image below)
- Immunofluorescence: positive lambda light chain staining in glomeruli
- Electron microscopy: randomly arranged, unbranched fibrils 7-10 nm in diameter - the ultrastructural hallmark
Step 4: Amyloid Typing - Knowing the Enemy
Confirming amyloid is present is only half the battle. Typing is mandatory because treatment is radically different for AL vs. ATTR vs. AA amyloidosis.
Immunohistochemistry (IHC)
IHC on paraffin-embedded tissue using antibody panels directed against:
- Kappa and lambda immunoglobulin light chains (for AL)
- Immunoglobulin heavy chains
- Serum amyloid A (SAA) (for AA)
- Transthyretin (TTR) (for ATTR)
Immunofluorescence (IF) on Frozen Sections
IF is superior to IHC for amyloid typing and gives a higher rate of successful identification. In AL amyloidosis, it identifies Ig light chain deposits in >80% of cases on kidney biopsy.
Tandem Mass Spectrometry (Gold Standard for Typing)
When IHC and IF are inconclusive (due to local proteolysis, inaccessible epitopes, or lack of commercial antibodies), laser capture microdissection combined with tandem mass spectrometry provides:
- Correct typing in nearly 100% of cases
- Identification of rare and unexpected amyloid precursors
- Available at specialized amyloid centers
"Due to their high sensitivity and specificity, they allow correct typing in nearly 100% of cases. Although available only in a few specialized centers, they should be systematically considered when routine antibody-based techniques are inconclusive."
- Comprehensive Clinical Nephrology, 7th Ed.
Genetic Testing / TTR Gene Sequencing
When ATTR amyloidosis is confirmed (by IHC or scintigraphy), TTR gene sequencing distinguishes:
- ATTRv (variant/hereditary): pathogenic TTR mutation (e.g., V30M causing polyneuropathy, V122I causing cardiomyopathy in ~4% of Black Americans)
- ATTRwt (wild-type): no mutation; "senile" amyloidosis, typically age >70 years, predominantly cardiac
Genetic counseling and presymptomatic genetic testing of first-degree relatives is recommended when a pathogenic TTR variant is identified.
Diagnostic Summary Table
| Method | What It Detects | Key Finding |
|---|---|---|
| Serum FLC + SPEP + immunofixation | Monoclonal protein (AL) | Abnormal FLC ratio, M-spike |
| NT-proBNP / Troponin | Cardiac involvement staging | Elevated out of proportion |
| Echocardiography | Myocardial infiltration | Biventricular hypertrophy, apical sparing, sparkling |
| Cardiac MRI | Myocardial infiltration + ECV | Diffuse LGE, increased ECV |
| 99mTc-PYP / DPD bone scan | ATTR cardiac amyloidosis | Grade 2/3 myocardial uptake |
| Congo red stain (LM) | Amyloid presence | Pink-red deposits |
| Congo red + polarized light | Amyloid presence | Apple-green birefringence |
| Electron microscopy | Amyloid fibrils | 7-10 nm randomly arranged fibrils |
| Immunofluorescence | Amyloid typing | Lambda/kappa restriction, SAA, TTR |
| IHC | Amyloid typing | Antibody-specific staining |
| Tandem mass spectrometry | Definitive typing | ~100% accuracy |
| TTR gene sequencing | ATTRv vs. ATTRwt | Specific mutation identified |
Resolution of Mr. Harrison's Story
Mr. Harrison's kidney biopsy confirms AL amyloidosis (lambda type) by immunofluorescence. Bone marrow biopsy shows 15% clonal lambda-restricted plasma cells, confirming an underlying plasma cell dyscrasia. The Tc-PYP scan shows no significant myocardial uptake (arguing against ATTR as the primary driver). He is referred to haematology for staging and treatment with a daratumumab-based regimen (Dara-CyBorD).
Key Teaching Points
- Congo red + polarized light = gold standard histological test. Apple-green birefringence is pathognomonic.
- Tissue sections must be ≥5 µm - thinner sections cause false-negative Congo red.
- All amyloid types share the same birefringence - typing requires IHC/IF or mass spectrometry.
- Start with non-invasive biopsies (fat pad, minor salivary gland, rectum) before organ biopsy.
- Tc-PYP scan is >99% sensitive for ATTR cardiomyopathy, but a positive result in a patient with a monoclonal protein still requires tissue confirmation.
- ATTRwt is the only amyloid subtype diagnosable without biopsy (positive scintigraphy + absence of monoclonal protein).
- Tandem mass spectrometry is the most accurate typing method and is the fallback when antibody-based techniques fail.
- Electron microscopy shows 7-10 nm randomly arranged, non-branching fibrils - distinct from other fibrillar deposits.
Sources:
- Robbins & Kumar Basic Pathology (Robbins Pathology)
- Comprehensive Clinical Nephrology, 7th Edition
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set
- Goldman-Cecil Medicine International Edition
- Fuster and Hurst's The Heart, 15th Edition
- Braunwald's Heart Disease, 2-Volume Set
This is a shared conversation. Sign in to Orris to start your own chat.