Management of IBS
Reading File
Finding Sources
Searching PubMed
"irritable bowel syndrome"[MeSH Terms] AND "management"[Title/Abstract]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I have very rich content. I now have everything needed to write a comprehensive answer. Let me also fetch the diagnostic algorithm image to include it.
Management of Irritable Bowel Syndrome (IBS)
IBS is a functional bowel disorder characterized by chronic or recurrent abdominal pain associated with alterations in stool form and/or frequency. It is diagnosed using the Rome IV criteria and managed in a stepwise, subtype-guided fashion. Below is a structured overview.
1. Diagnosis First: Rome IV Criteria
Before treatment, confirm the diagnosis positively - IBS should not be a diagnosis of exclusion in straightforward cases.
Rome IV criteria (symptoms for at least 6 months, active for last 3 months):
- Recurrent abdominal pain at least 1 day/week, associated with 2 or more of:
- Related to defecation
- Change in stool frequency
- Change in stool form/appearance
Alarm features requiring investigation:
- New onset at age ≥50 years
- Unintentional weight loss
- Rectal bleeding (hematochezia/melena not from hemorrhoids)
- Nocturnal diarrhea
- Anemia
- Palpable abdominal mass or lymphadenopathy
- Family history of colorectal cancer, IBD, or celiac disease
Recommended tests (limited):
| Test | Population |
|---|---|
| Celiac serologies (IgA anti-TTG) | IBS-D |
| Fecal calprotectin/lactoferrin | IBS-D |
| CRP | IBS-D |
| Bile acid diarrhea testing | IBS-D if suspected |
| Giardia stool antigen | IBS-D in endemic areas |
| Colonoscopy with random biopsies | Age >45-50 or alarm features |
Not routinely recommended: routine colonoscopy in patients <45 without alarm features, food allergy testing, lactulose/glucose breath tests.
2. IBS Subtypes
| Subtype | Abbreviation | Frequency |
|---|---|---|
| Predominant diarrhea | IBS-D | 35-40% |
| Mixed bowel habits | IBS-M | 35-40% |
| Predominant constipation | IBS-C | ~25% |
| Unclassified | IBS-U | <5% |
3. Overall Management Approach (Severity-Tiered)
Mild symptoms (little impact on quality of life): positive diagnosis, patient education, reassurance, dietary advice, OTC medications.
Moderate symptoms (affect daily activities): above + pharmacotherapy targeted to the dominant symptom.
Severe symptoms (major quality-of-life impact, psychological comorbidity, treatment-refractory): integrated pharmacologic + behavioral/psychological treatment.
4. Non-Pharmacological Treatments (All Subtypes)
Diet - Low-FODMAP
The low-FODMAP diet (reducing Fermentable Oligosaccharides, Disaccharides, Monosaccharides, And Polyols) is a proven first-line intervention. It reduces global IBS symptoms, particularly bloating, abdominal pain, and abnormal bowel habits, especially in IBS-D. This diet should be supervised by a trained dietitian who guides re-introduction of foods. A 1-2 week food and symptom diary helps identify individual triggers.
A recent 2025 network meta-analysis (Lancet Gastroenterol Hepatol, PMID 40258374) confirms dietary interventions - particularly low-FODMAP - have the strongest evidence among dietary approaches.
Gluten-free diet: less clear benefit; may be tried in patients whose symptoms consistently worsen with gluten-containing foods.
Soluble Fiber
- Psyllium (soluble fiber): 25-35 g/day; most beneficial in IBS-C; also helpful in other subtypes.
- Start at low doses and increase gradually to avoid gas and discomfort.
- Insoluble fiber (bran) is NOT recommended - can worsen symptoms.
Exercise
Regular physical activity improves overall IBS symptoms and is recommended as part of lifestyle management.
Stress Reduction
Psychological stress is a major trigger. Identifying and reducing stressors is part of first-line care.
5. Psychological / Brain-Gut Behavioral Therapies
These are the most evidence-based treatments for severe or refractory IBS. A 2025 network meta-analysis in Lancet Gastroenterol Hepatol (PMID 41077057) confirms their efficacy.
| Therapy | Notes |
|---|---|
| Cognitive Behavioral Therapy (CBT) | Strongest evidence; first-line for severe/refractory IBS |
| Gut-directed hypnotherapy | High efficacy, especially for global symptoms |
| Mindfulness-based stress reduction | Beneficial for abdominal pain |
| Psychodynamic therapy | Evidence for global symptoms |
| Relaxation training | Adjunctive benefit |
A 2024 network meta-analysis (Gastroenterology, PMID 38777133) specifically shows brain-gut behavioral treatments are superior to control for abdominal pain in IBS.
6. Pharmacological Treatment
IBS-C (Constipation-Predominant) Agents
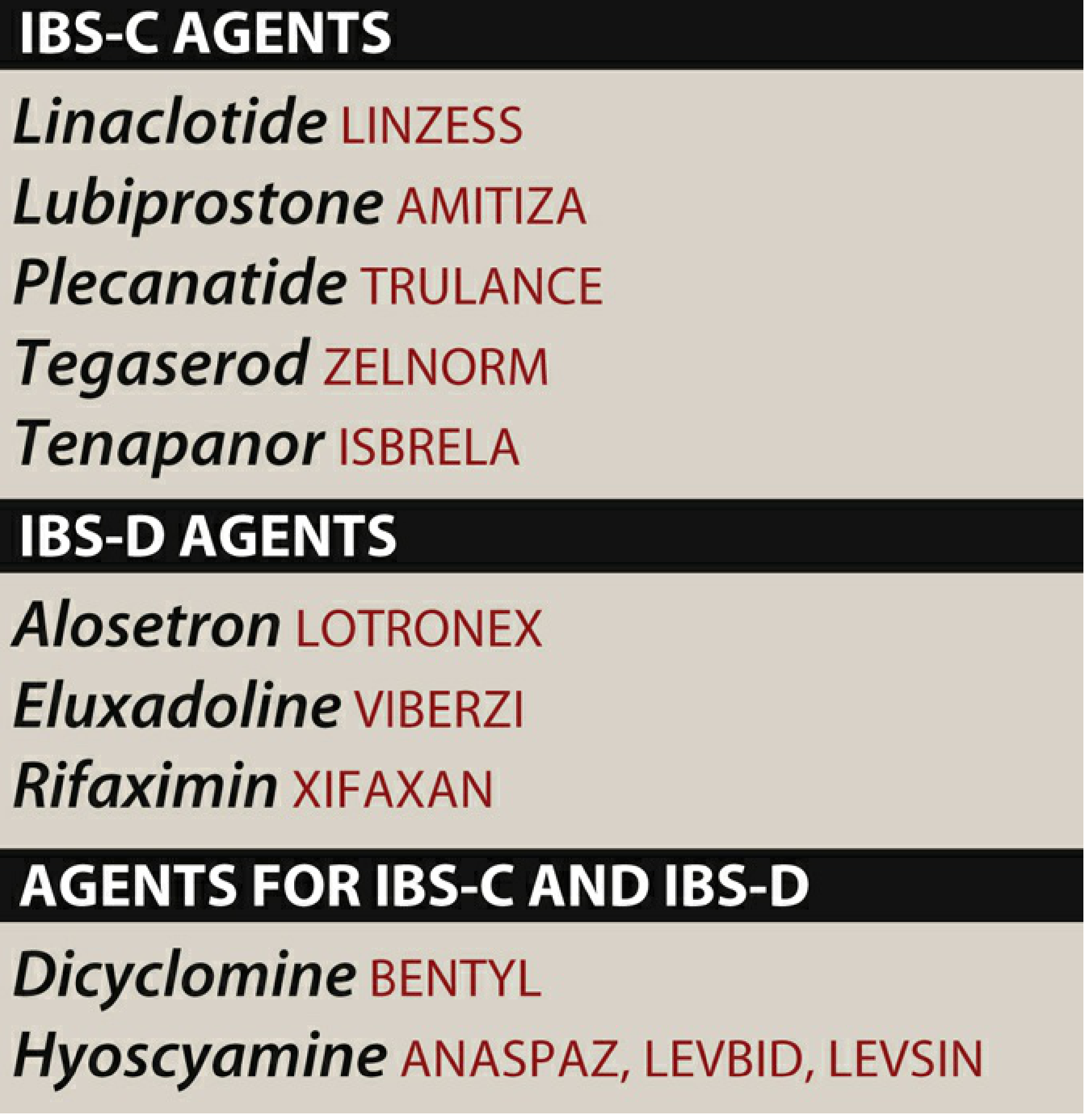
| Drug | Mechanism | Key Notes |
|---|---|---|
| Linaclotide (Linzess) | Guanylate cyclase-C agonist | IBS-C; also used in chronic idiopathic constipation; main SE: diarrhea |
| Plecanatide (Trulance) | Guanylate cyclase-C agonist | IBS-C; similar to linaclotide; SE: diarrhea |
| Lubiprostone (Amitiza) | Chloride channel (ClC-2) activator | Women with IBS-C; increases intestinal fluid secretion; SE: nausea, diarrhea |
| Tegaserod (Zelnorm) | 5-HT4 partial agonist | Women with IBS-C and <65 years old; contraindicated in history of MI, stroke, or angina |
| Tenapanor (Isbrela) | NHE3 (sodium/hydrogen exchanger 3) inhibitor | IBS-C; reduces sodium absorption, increases water in stool; SE: diarrhea |
| Osmotic laxatives (PEG/macrogol) | Osmotic effect | Can improve stool consistency but not validated to reduce abdominal pain in IBS-C specifically |
IBS-D (Diarrhea-Predominant) Agents
| Drug | Mechanism | Key Notes |
|---|---|---|
| Rifaximin (Xifaxan) | Non-absorbable antibiotic (structural analog of rifampin) | Short-term use; reduces bacterial load; may be repeated; SE: nausea, fatigue, headache, rare C. difficile |
| Alosetron (Lotronex) | 5-HT3 antagonist | Women with severe IBS-D only (restricted prescribing program); SE: constipation, ischemic colitis (rare) |
| Eluxadoline (Viberzi) | Mixed mu/kappa-opioid agonist + delta-opioid antagonist | IBS-D; reduces diarrhea and pain; contraindicated in pancreatitis, biliary duct obstruction, alcoholism; SE: constipation, abdominal pain, rare pancreatitis |
| Loperamide | Opioid receptor agonist (peripheral) | OTC; slows motility; reduces diarrhea but NOT validated for abdominal pain in IBS |
| Cholestyramine | Bile acid sequestrant | Useful in bile acid malabsorption-related IBS-D |
Antispasmodics (IBS-C and IBS-D)
| Drug | Mechanism | Notes |
|---|---|---|
| Dicyclomine (Bentyl) | Antimuscarinic | Reduces GI spasms and motility; SE: anticholinergic effects (dry mouth, drowsiness) |
| Hyoscyamine (Levsin) | Antimuscarinic | Same class; overdose can cause hallucinations, arrhythmias |
| Peppermint oil | Smooth muscle calcium channel relaxation | Natural antispasmodic; evidence for abdominal pain reduction |
Antidepressants
Used for pain modulation via central and peripheral mechanisms, independent of their antidepressant effect:
| Drug | Use |
|---|---|
| Tricyclic antidepressants (TCAs) - e.g., amitriptyline, nortriptyline | IBS-D (anticholinergic effects slow GI transit); also reduce visceral hypersensitivity |
| SSRIs/SNRIs | IBS-C (can accelerate transit); also helpful for psychological comorbidities |
| Low-dose antidepressants | Used even in absence of depression for visceral pain modulation |
7. Treatment by Subtype - Summary Algorithm
ALL IBS:
→ Education + reassurance
→ Dietary modification (low-FODMAP, trigger avoidance)
→ Soluble fiber (psyllium)
→ Regular exercise + stress management
→ Antispasmodics (for pain/cramps)
IBS-C (add):
→ Osmotic laxatives (PEG)
→ Linaclotide / Plecanatide
→ Lubiprostone (women)
→ Tenapanor
→ Tegaserod (women <65, no CVD)
→ TCAs (SSRIs if constipation dominant)
IBS-D (add):
→ Loperamide (acute diarrhea control)
→ Rifaximin (short course, repeatable)
→ Eluxadoline (avoid in pancreatitis/alcoholism)
→ Alosetron (severe IBS-D in women only, restricted program)
→ Bile acid sequestrants if bile acid malabsorption suspected
→ TCAs (low dose)
Refractory/Severe (any subtype, add):
→ CBT
→ Gut-directed hypnotherapy
→ Psychodynamic therapy / mindfulness
→ Specialist referral
8. Special Populations
- Pregnancy: Most pharmacological agents above are avoided; dietary and behavioral approaches are first-line.
- Post-infectious IBS: Consider rifaximin; address gut dysbiosis. Small intestinal bacterial overgrowth (SIBO) can co-occur - treat if present.
- IBS with bloating/distention: Low-FODMAP diet most effective; rifaximin may help; neuromodulators can reduce visceral sensitivity.
Key Points to Remember
- IBS is a positive diagnosis using Rome IV criteria, not a diagnosis of exclusion.
- Low-FODMAP diet is the most evidence-based dietary intervention - always involve a dietitian.
- Soluble fiber yes, insoluble fiber no.
- Psychological therapies (especially CBT and gut-directed hypnotherapy) have strong evidence for refractory or severe IBS.
- Drug choice is subtype-dependent - IBS-C agents can precipitate severe diarrhea in IBS-D and vice versa.
- Alosetron (IBS-D) and tegaserod (IBS-C) have restricted use due to safety concerns (ischemic colitis and cardiovascular risk, respectively).
- Antidepressants work for visceral pain modulation even without comorbid depression.
- Treatment is rarely a single intervention - most patients benefit from a combination approach.
Sources: Goldman-Cecil Medicine (International Edition) - Ch. 123; Lippincott Illustrated Reviews: Pharmacology - Ch. 42; Sleisenger & Fordtran's Gastrointestinal and Liver Disease - Ch. 122. Recent evidence: PMID 40258374 (dietary interventions, Lancet GH 2025), PMID 41077057 (behavioral therapies, Lancet GH 2025), PMID 38777133 (brain-gut treatments, Gastroenterology 2024).
This is a shared conversation. Sign in to Orris to start your own chat.