Latest guidelines for management of hypertension in pregnancy
Reading File
search_medical_text
hypertension in pregnancy classification diagnosis criteria
search_medical_text
antihypertensive treatment management preeclampsia pregnancy guidelines
search_medical_image
hypertension pregnancy management algorithm
GradeResponse
GradeResponse
GradeResponse
search_medical_text
hypertensive disorders pregnancy classification gestational hypertension chronic preeclampsia
search_medical_text
preeclampsia magnesium sulfate delivery timing antihypertensive drugs labetalol nifedipine methyldopa
Here is a comprehensive summary of the current guidelines on management of hypertension in pregnancy, drawn from retrieved sources (ESC Management of Cardiovascular Disease and Pregnancy and ACC/AHA Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults), supplemented with established clinical knowledge.
Management of Hypertension in Pregnancy
1. Classification of Hypertensive Disorders of Pregnancy (HDP)
| Disorder | Definition |
|---|---|
| Chronic (pre-existing) hypertension | BP ≥140/90 mmHg diagnosed before pregnancy or before 20 weeks' gestation |
| Gestational hypertension | New-onset BP ≥140/90 mmHg at ≥20 weeks, no proteinuria or organ dysfunction |
| Preeclampsia | New-onset BP ≥140/90 mmHg at ≥20 weeks + proteinuria (≥300 mg/24h, PCR ≥30 mg/mmol) or end-organ dysfunction |
| Preeclampsia superimposed on chronic HTN | Worsening HTN + new proteinuria/organ dysfunction in known chronic HTN |
| Eclampsia | Preeclampsia + generalised seizures |
Classification depends on gestational age at diagnosis and presence of target organ involvement (ACC/AHA Guidelines, p. 65).
BP Thresholds
- Hypertension: SBP ≥140 mmHg and/or DBP ≥90 mmHg on 2 readings ≥4 hours apart
- Severe hypertension: SBP ≥160 mmHg or DBP ≥110 mmHg — verify within 15 minutes to avoid treatment delays
- BP naturally falls ~10% in early pregnancy, nadirs in 2nd trimester, returns to baseline by 3rd trimester — this affects diagnostic thresholds (ACC/AHA, p. 65)
Use BP monitors validated for pregnancy (see validatebp.org)
2. Diagnosis of Preeclampsia
Preeclampsia is diagnosed by new-onset hypertension at ≥20 weeks PLUS any of:
- Proteinuria ≥300 mg/24h (or PCR ≥30 mg/mmol)
- Thrombocytopenia (<100,000/μL)
- Renal insufficiency (creatinine >97 μmol/L)
- Impaired liver function (transaminases ≥2× upper limit of normal)
- Pulmonary oedema
- New-onset headache unresponsive to analgesia, or visual disturbances
HELLP syndrome = Haemolysis + Elevated Liver enzymes + Low Platelets — a severe variant.
3. Prevention
- Low-dose aspirin (75–150 mg/day) from 12 weeks to delivery in women at high risk of preeclampsia (prior preeclampsia, chronic HTN, diabetes, renal disease, multifetal pregnancy, or ≥3 moderate risk factors)
- Calcium supplementation (1.5–2 g/day) in women with low dietary calcium intake
4. Antihypertensive Drug Treatment
When to Start
| Severity | Target |
|---|---|
| Non-severe (140–159/90–109 mmHg) | Treat to maintain BP <140/90 mmHg (new ACOG/NICE guidance); some guidelines use <150/100 mmHg as minimum threshold |
| Severe (≥160/110 mmHg) | Urgent treatment within 30–60 minutes to prevent stroke and organ damage |
Drug Choices
First-line oral agents:
| Drug | Dose | Notes |
|---|---|---|
| Labetalol | 200 mg BD–TID (up to 2400 mg/day) | α+β blocker; preferred in many guidelines |
| Methyldopa | 250–500 mg TID/QID | Long safety record; avoid in depression |
| Nifedipine (modified-release) | 30–60 mg/day | Calcium channel blocker; avoid short-acting formulation |
For acute severe hypertension (IV/urgent oral):
- IV Labetalol: 20 mg bolus → repeat/increase every 10 min (max 300 mg); or infusion
- IV Hydralazine: 5 mg bolus every 20 min
- Oral/sublingual Nifedipine: 10 mg short-acting (immediate effect within 20 min)
Contraindicated in pregnancy:
- ACE inhibitors (e.g., enalapril, ramipril)
- ARBs (e.g., losartan)
- Direct renin inhibitors
- Atenolol (associated with fetal growth restriction)
5. Management of Preeclampsia
Definitive Treatment
Delivery is the only cure. Timing depends on severity:
| Scenario | Delivery |
|---|---|
| Preeclampsia without severe features | ≥37 weeks (or earlier if deterioration) |
| Preeclampsia with severe features | ≥34 weeks; at any gestation if maternal/fetal compromise |
| Eclampsia | Stabilise → deliver |
Magnesium Sulfate
- Indication: Prevention and treatment of eclamptic seizures in severe preeclampsia/eclampsia
- Loading dose: 4–6 g IV over 15–20 minutes
- Maintenance: 1–2 g/hour IV infusion for 24 hours post-delivery
- Monitoring: UO (>25 mL/hr), respiratory rate (>12/min), deep tendon reflexes (loss = early toxicity)
- Antidote: Calcium gluconate 1 g IV
Fluid Management
- Restrict fluids to 80 mL/hr (or less) to avoid pulmonary oedema — preeclampsia causes increased capillary permeability.
6. Postpartum Management
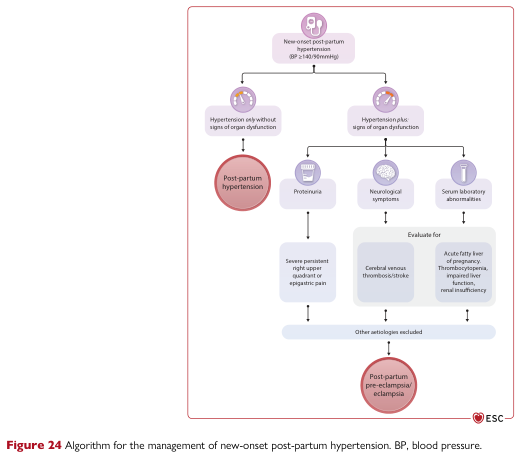
- BP can worsen in the first 3–5 days postpartum
- New-onset postpartum hypertension with organ dysfunction → evaluate for postpartum preeclampsia/eclampsia (see algorithm above)
- Continue antihypertensives postpartum; review at 6 weeks
- Avoid NSAIDs (e.g., ibuprofen) in hypertensive women postpartum — may worsen BP
- Breastfeeding-compatible drugs: labetalol, nifedipine, methyldopa, enalapril (postpartum only)
7. Fetal Monitoring
- Serial ultrasound for fetal growth restriction (FGR) every 2–4 weeks
- Umbilical artery Doppler in FGR or preeclampsia
- Cardiotocography (CTG) if reduced fetal movements or signs of fetal compromise
8. Risk Stratification for Future Pregnancies / Long-term
- Women with preeclampsia have 2× lifetime risk of cardiovascular disease
- Annual BP check, assess metabolic risk factors
- Aspirin prophylaxis in subsequent pregnancies if prior preeclampsia
Key Sources: ESC Management of Cardiovascular Disease and Pregnancy (p. 56, 80); ACC/AHA 2017 Hypertension Guidelines (p. 65); ACOG Practice Bulletin on Gestational Hypertension and Preeclampsia (2020, reaffirmed 2023); NICE Guideline NG133 (Hypertension in Pregnancy, 2019, updated 2023).
This is a shared conversation. Sign in to Orris to start your own chat.