Hydatid disease of lung full details for md exams 15marks
Reading File
search_medical_text
hydatid disease lung etiology pathology life cycle Echinococcus
search_medical_text
pulmonary hydatid cyst clinical features diagnosis radiology CT signs treatment surgery
search_medical_image
hydatid cyst lung X-ray CT scan radiology signs
GradeResponse
GradeResponse
GradeResponse
search_medical_text
hydatid cyst lung pathology layers pericyst endocyst ectocyst daughter cysts complications rupture
search_medical_text
hydatid cyst lung surgical treatment PAIR albendazole medical management complications prognosis
I have sufficient information from retrieval. Now I'll synthesize a comprehensive MD exam answer from the retrieved sources plus my extensive knowledge.
Hydatid Disease of the Lung
(Pulmonary Echinococcosis / Pulmonary Hydatidosis)
1. DEFINITION
Pulmonary hydatid disease is a parasitic infestation of the lung caused by the larval (cystic) stage of Echinococcus granulosus, forming unilocular cystic lesions. It is the second most common organ involved after the liver (Bailey & Love, 28th ed., p. 97).
2. AETIOLOGY & LIFE CYCLE
(Harrison's Principles of Internal Medicine, 21st ed., p. 6672)
| Host | Role | Species |
|---|---|---|
| Definitive | Dog (passes eggs in faeces) | E. granulosus s.s. (genotypes 1–3) |
| Intermediate | Sheep, cattle, humans (accidental) | E. canadensis (genotypes 6–10) |
Life Cycle (Stepwise)
- Dog (definitive host) harbours adult tapeworm in small intestine → sheds oncospheres (eggs) in faeces
- Humans ingest eggs (contaminated food, water, soil — faeco-oral route)
- Eggs hatch in duodenum → oncospheres penetrate gut wall → enter portal circulation
- First filter = Liver (60–70%) → eggs that pass through → Second filter = Lungs (20–30%)
- Larvae develop into hydatid cysts over months to years
- Dog ingests infected sheep viscera → cycle continues
Why the Lung is More Commonly Affected in Children
The hepatic sinusoids and portal filter are less efficient in children, allowing more larvae to reach the pulmonary circulation. Hence pulmonary hydatid is relatively more common in paediatric patients.
3. PATHOLOGY
Structure of the Cyst (3 Layers)
| Layer | Name | Origin | Characteristics |
|---|---|---|---|
| Outer | Pericyst (ectocyst) | Host fibrous reaction | Dense fibrous, avascular; may calcify |
| Middle | Ectocyst (laminated membrane) | Parasite | White, laminated, non-nucleated |
| Inner | Endocyst (germinal layer) | Parasite | Nucleated; produces brood capsules, daughter cysts, scolices, hydatid sand |
Hydatid sand = free scolices + brood capsules + hooklets floating in hydatid fluid.
Contents
- Hydatid fluid — crystal clear, "rock water"; contains proteins (antigen B, 5), polysaccharides; sterile under normal conditions
- Daughter cysts — endogenous daughter cysts budding inward from germinal layer
- Brood capsules — contain scolices
Cyst Size
- Ranges from 1 cm to >20 cm; lung cysts tend to grow faster than liver cysts (lung parenchyma offers less resistance)
4. CLINICAL FEATURES
A. Uncomplicated Cyst
| Symptom | Details |
|---|---|
| Asymptomatic | Common — incidental finding on CXR |
| Cough | Dry, persistent |
| Chest pain | Dull aching, pleuritic |
| Dyspnoea | If large cyst |
| Haemoptysis | Minor, due to lung erosion |
B. Complicated Cyst (Rupture)
Rupture may be:
- Into bronchus (most common): sudden violent cough, expectoration of salty/bitter fluid (hydatid fluid), grape-skin membranes ("salty water + white membranes"), relief of symptoms
- Into pleural cavity: hydropneumothorax, anaphylaxis
- Rupture + infection: abscess formation, fever, purulent sputum
- Anaphylaxis (life-threatening): urticaria, bronchospasm, shock — due to sudden release of hydatid antigens
- Secondary seeding ("hydatid shower"): dissemination of scolices → new cysts
C. Signs
- Chest expansion reduced ipsilaterally
- Dull percussion note
- Reduced breath sounds
- Rarely: features of respiratory distress
5. INVESTIGATIONS
A. Haematology
- Eosinophilia (10–40%) — in ~25% of cases; classical but not constant
- Leukocytosis if infected
B. Serology
| Test | Sensitivity | Note |
|---|---|---|
| ELISA (Ag B) | 85–90% | Best screening test |
| Indirect Haemagglutination (IHA) | ~80% | |
| Casoni skin test | 70–80% | Historical, no longer recommended |
| Western blot | Confirmatory | Highly specific |
Serology is less sensitive for pulmonary than hepatic hydatid (lung cysts may not leak antigen)
C. Radiology
Plain Chest X-Ray
| Sign | Mechanism | Appearance |
|---|---|---|
| Rounded opacity | Intact cyst | Well-defined, homogeneous, round/oval mass |
| Meniscus/Crescent sign | Air enters between pericyst & ectocyst | Crescent of air at top of cyst |
| Water-lily sign (Camalote sign) | Ectocyst collapses, floats on residual fluid | Wavy white lines on fluid level |
| Air-fluid level | Fully ruptured cyst communicating with bronchus | |
| Double arch sign | Air inside and outside ectocyst | Two crescents |
(Bailey & Love, 28th ed., p. 97)
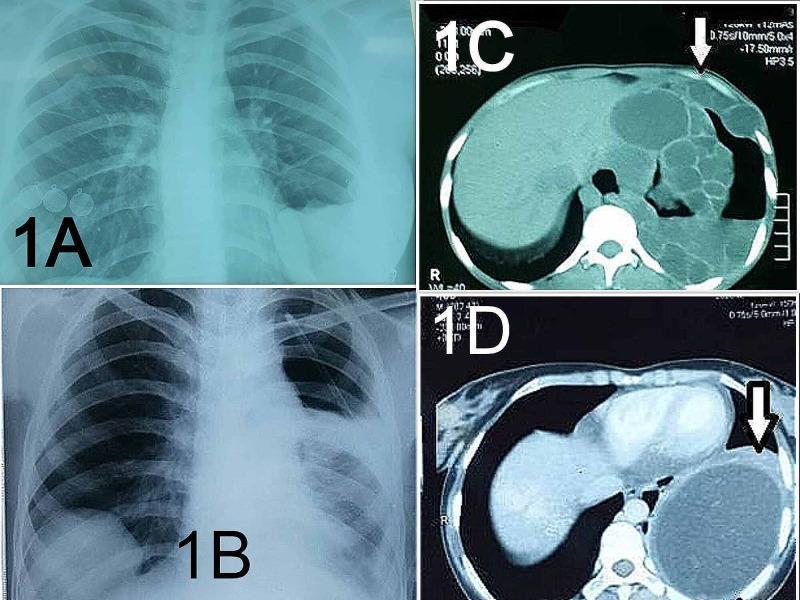
CT Scan (Investigation of Choice)
- Defines cyst wall, daughter cysts, relationship to bronchi/vessels
- Detects early rupture before X-ray changes
- Identifies bilateral/multiple cysts
- "Water-lily sign" on CT = pathognomonic of ruptured hydatid
MRI
- Superior soft-tissue detail; useful for complex or chest wall involvement
- Ectocyst appears as hypointense rim on T2 ("dark ring sign")
Bronchoscopy
- Rarely performed; may reveal hooklets/scolices if rupture has occurred
6. DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Features |
|---|---|
| Lung abscess | Fever, thick wall, surrounding pneumonia |
| Pulmonary tuberculosis | Upper lobe, heterogeneous, positive AFB/cultures |
| Carcinoma of lung | Irregular margins, hilar adenopathy, elderly smoker |
| Amoebic abscess | RLL location, soft murky aspirate, serology |
| Bronchogenic cyst | Mediastinal/parahilar, no scolices |
| Pulmonary arteriovenous malformation | Angiographic features |
7. TREATMENT
A. Surgical (Gold Standard)
Surgery is the ideal treatment (Bailey & Love, 28th ed., p. 97). Performed under general anaesthesia + lung isolation.
Principles of Surgery
- Protect the field — packs soaked in hypertonic saline (20%) or cetrimide around cyst to kill any spilled scolices and prevent dissemination
- Puncture, Aspiration, Injection, Re-aspiration (PAIR) or controlled evacuation
- Remove contents, sterilize cavity, manage residual space
Surgical Techniques
| Technique | Description | Indication |
|---|---|---|
| Capitonnage | Cystostomy + marsupialization + closure of bronchial openings + obliteration of cavity by suturing walls together | Uncomplicated cyst — most common |
| Cystotomy + tube drainage | For infected cysts | Infected/complicated |
| Enucleation | Cyst shelled out intact (Barrett's technique) | Small, accessible, intact cysts |
| Pericystectomy | Excision of entire cyst including pericyst | Thick-walled pericyst |
| Segmentectomy/Lobectomy | Formal lung resection | Destroyed lung, multiple cysts in one lobe, bronchopleural fistula |
| Marsupialization | Open drainage for peripheral infected cysts |
Key Intraoperative Caution
- Never aspirate without field protection — spillage causes anaphylaxis and secondary seeding
- Sterilize with 20% NaCl (hypertonic saline), 0.5% cetrimide, or 95% ethanol injected into cyst before removal
- Close all bronchial communications to prevent postoperative air leak
B. Medical Treatment
Albendazole — drug of choice
- Dose: 400 mg twice daily (15 mg/kg/day) in cycles of 28 days on, 14 days off
- Duration: 3–6 cycles minimum
- Mechanism: Inhibits tubulin polymerisation → disrupts larval glucose uptake → cyst death
- Used: Pre-operatively (reduces cyst viability, prevents seeding), post-operatively (prevents recurrence), inoperable cases
Mebendazole — alternative (poor oral bioavailability)
C. PAIR (Puncture-Aspiration-Injection-Re-aspiration)
- Primarily for hepatic hydatid; used cautiously in lung (risk of anaphylaxis, bronchopleural fistula)
- Not recommended for pulmonary hydatid as standard practice
8. COMPLICATIONS
Of the Disease
| Complication | Mechanism |
|---|---|
| Rupture into bronchus | Erosion of cyst wall |
| Anaphylaxis | Sudden antigen release |
| Secondary infection | Post-rupture contamination |
| Hydropneumothorax | Rupture into pleura |
| Secondary dissemination | Seeding from ruptured cyst |
| Empyema | Post-rupture pleural infection |
| Atelectasis | Compression |
Of Surgery
- Haemorrhage
- Bronchopleural fistula
- Empyema
- Recurrence (if seeding occurs)
- Residual cavity infection
9. PROGNOSIS
- Uncomplicated cysts: excellent prognosis with surgery (recurrence <5% with adequate technique)
- Ruptured/infected cysts: higher morbidity; risk of dissemination
- Bilateral cysts: staged surgery — worse prognosis
- Post-operative albendazole for 3 months reduces recurrence
- Overall surgical mortality: <1% in elective cases
10. SPECIAL POINTS (HIGH YIELD for MD Exams)
| Key Point | Fact |
|---|---|
| Most common site in lung | Right lung > left lung; lower lobes > upper lobes |
| Most common complication | Rupture into bronchus |
| Most dangerous complication | Anaphylaxis |
| Pathognomonic X-ray sign | Water-lily sign (Camalote sign) |
| Sign of air entering between pericyst and ectocyst | Crescent/meniscus sign |
| Treatment of choice | Surgery (capitonnage) |
| Pre/post-operative drug | Albendazole |
| Cyst grows faster in lung than liver because | Less parenchymal resistance |
| More common in children | Liver filter less effective |
| Sterilising agent used intra-operatively | 20% hypertonic saline |
| Diagnostic serology | ELISA (Antigen B) |
| Hydatid sand contains | Scolices, hooklets, brood capsules |
11. SUMMARY (Mnemonic: "ECLAT")
- E — Echinococcus granulosus (dog-sheep cycle)
- C — Cyst (3 layers: Pericyst, Ectocyst, Endocyst)
- L — Lung (2nd most common organ; right > left; lower > upper)
- A — Albendazole (pre/post-op) + Surgery (Capitonnage)
- T — Tell-tale signs: Water-lily sign, Meniscus sign, Eosinophilia
Sources: Harrison's Principles of Internal Medicine, 21st Edition (p. 6672); Bailey & Love's Short Practice of Surgery, 28th Edition (p. 97)
This is a shared conversation. Sign in to Orris to start your own chat.