Causes of blindness and symptoms of eye disorders
Reading File
Finding Sources
Finding Sources
Searching the Web
leading causes of blindness worldwide 2024 WHO
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
I now have rich material from multiple authoritative sources. Here is a thorough, well-organized answer.
Causes of Blindness and Symptoms of Eye Disorders
Global Overview
As of 2020, approximately 33.6 million people live with blindness worldwide, and over 206 million have moderate-to-severe vision impairment. Cataract and uncorrected refractive error together account for the majority of global blindness. The leading causes differ by country and age group.
Leading Causes of Blindness
1. Cataract
Cataract (clouding of the lens) is responsible for 51% of world blindness according to the WHO and is the single most common cause globally.
Symptoms:
- Gradual, painless blurring of vision - often worse at night
- Increased glare and halos around lights
- Faded or yellowed colors
- Frequent changes in eyeglass prescription
- Double vision in one eye
The lens opacity blocks or scatters incoming light. Cataract surgery (lens replacement) is the definitive treatment and is covered by Medicare in the US.
- Goldman-Cecil Medicine, block 57
2. Glaucoma
Glaucoma is a group of diseases causing optic neuropathy, usually (but not always) associated with elevated intraocular pressure (IOP). It accounts for at least 10% of blindness in the US and is 4x more common in African Americans, who are 8x more likely to go blind from it. The most common form in the US is primary open-angle glaucoma (POAG).
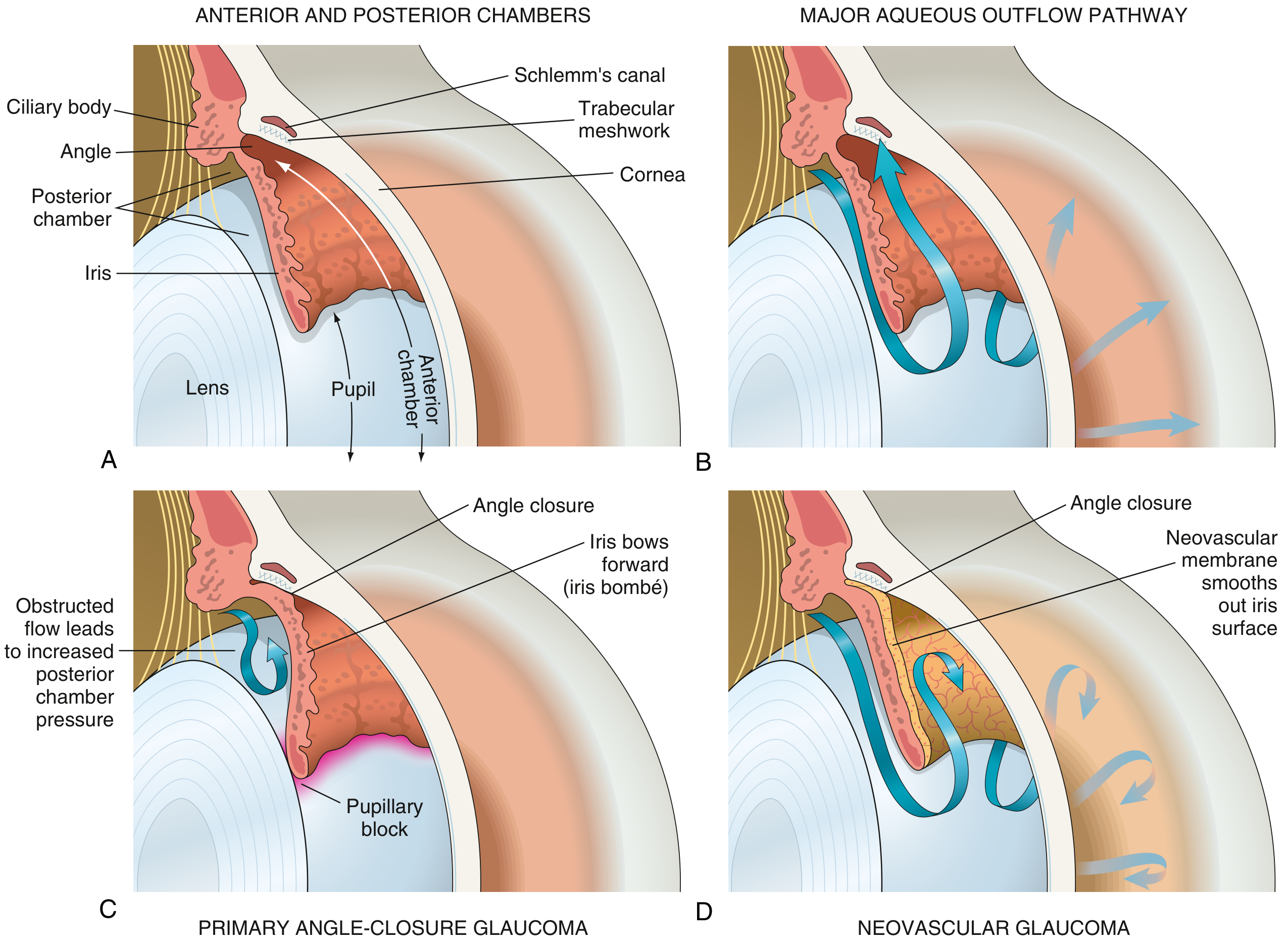
Pathophysiology: Aqueous humor, produced in the ciliary body, normally drains through the trabecular meshwork into Schlemm's canal. When this outflow is obstructed, IOP rises and damages the optic nerve.
Types and symptoms:
| Type | Symptoms |
|---|---|
| Open-angle glaucoma | Often silent early; gradual peripheral (tunnel) vision loss; discovered incidentally on tonometry |
| Angle-closure glaucoma (acute) | Sudden severe eye pain, headache, nausea/vomiting, halos around lights, blurred vision, red eye |
| Neovascular glaucoma | Secondary to diabetes/vascular disease; severe vision loss |
| Steroid-induced glaucoma | Follows prolonged corticosteroid eye drops or systemic steroids |
| Congenital glaucoma | Enlarged eyes (buphthalmos), tearing, light sensitivity |
The damage to vision caused by glaucoma is irreversible - early detection is key. Treatment includes topical medications (beta-blockers, prostaglandin analogs), laser surgery, and trabeculectomy.
- Robbins & Kumar Basic Pathology, p. 868-869
- Textbook of Family Medicine 9e, p. 371-373
3. Age-Related Macular Degeneration (AMD)
AMD is the leading cause of blindness in adults aged 65+ and primarily damages the macula (the central, high-acuity part of the retina).
Types:
- Dry AMD: Gradual accumulation of drusen (membranous debris) and geographic atrophy of the retinal pigment epithelium
- Wet AMD: Choroidal neovascularization - fragile new vessels leak and bleed, causing rapid central vision loss
Symptoms:
- Blurry or distorted central vision (straight lines appear wavy - "metamorphopsia")
- Dark or empty spot in the center of vision (scotoma)
- Colors appearing less vivid
- Difficulty reading or recognizing faces
- Peripheral vision is preserved - people can still navigate around but cannot see detail
Treatment options include antioxidant vitamins (AREDS formula: vitamins C, E, beta-carotene, zinc), anti-VEGF intravitreal injections (for wet AMD), and laser photocoagulation.
- Textbook of Family Medicine 9e, pp. 371-372
4. Diabetic Retinopathy (DR)
DR is the most common cause of blindness in Americans aged 20 to 74 years. People with diabetes are at 25 times greater risk of becoming blind compared to non-diabetics.
Mechanism: Chronic hyperglycemia damages retinal blood vessels, leading to progressive leakage, hemorrhage, neovascularization, and eventual traction retinal detachment.
Symptoms (often absent until advanced):
- Blurred or fluctuating vision
- Dark spots or floaters
- Impaired color vision
- Sudden vision loss (from vitreous hemorrhage)
- Vision loss in both eyes if advanced
Key point: Macular edema (fluid accumulation at the macula) accounts for most cases of decreased vision in DR, while proliferative DR can cause catastrophic hemorrhage.
- Goldman-Cecil Medicine, block 57
- Textbook of Family Medicine 9e, p. 372
5. Refractive Errors
Uncorrected refractive errors (myopia, hyperopia, astigmatism, presbyopia) are the most frequent eye problems in the US and are the second leading cause of global blindness. They are correctable with glasses, contact lenses, or surgery (LASIK, PRK).
Symptoms:
- Blurred vision at distance (myopia) or near (hyperopia, presbyopia)
- Eyestrain and headaches
- Squinting
6. Retinal Vascular Occlusions
Central Retinal Artery Occlusion (CRAO):
- Sudden, painless, complete unilateral vision loss
- Signs: cherry-red spot at the macula, pale/edematous retina, narrowed arteries
- Considered a "stroke of the eye" - ocular emergency
Central Retinal Vein Occlusion:
- Sudden painless visual loss, often with "blood and thunder" fundus appearance
- Associated with hypertension and hyperviscosity
7. Retinal Detachment
Symptoms (urgent - requires immediate referral):
- Sudden increase in floaters
- Flashing lights (photopsia)
- A "veil" or "curtain" appearing across the visual field
- Preceded by posterior vitreous detachment in many cases
Floaters alone are usually benign (from vitreous gel degeneration with aging), but their sudden increase alongside flashes is a red flag for retinal tear or detachment.
- Textbook of Family Medicine 9e, p. 371
8. Optic Neuritis and Optic Neuropathy
- Optic neuritis: Inflammation of the optic nerve; painful eye movement, central visual loss; ~75% of women and 34% of men develop multiple sclerosis within 15 years
- Ischemic optic neuropathy: Sudden painless monocular vision loss; associated with temporal arteritis (GCA) - a medical emergency requiring immediate steroids
9. Infectious Causes
- Trachoma (Chlamydia trachomatis): Leading infectious cause of blindness globally; causes scarring conjunctivitis and corneal opacity
- Onchocerciasis ("river blindness"): Onchocerca volvulus microfilariae invade cornea causing "snowflake" keratitis
- Herpes simplex keratitis: Recurrent infection causes corneal scarring and chronic keratitis
- Cytomegalovirus (CMV) retinitis: Occurs in immunocompromised patients (HIV/AIDS); causes progressive necrotizing retinitis
10. Other Important Causes
| Cause | Key Features |
|---|---|
| Corneal disease/scarring | Trauma, infection, chemical burns; corneal transplant may restore vision |
| Temporal arteritis (GCA) | Older adults >50; headache, jaw claudication, elevated ESR/CRP; sudden vision loss |
| Cortical blindness | Bilateral occipital lobe infarcts; can cause complete loss of conscious vision |
| Amaurosis fugax | Transient monocular blindness from carotid emboli; TIA equivalent - 50% risk of stroke within 1 month |
| Amblyopia | "Lazy eye" - reduced vision from abnormal visual development in childhood |
| Vitamin A deficiency | Causes night blindness and xerophthalmia; major cause in developing countries |
| Hereditary retinal dystrophies | Retinitis pigmentosa: progressive peripheral then central loss; night blindness early |
| Hypertensive retinopathy | Chronic hypertension causes arteriolar changes; severe cases cause vision loss |
Rapid Approach to Sudden Vision Loss
From the Textbook of Family Medicine, four common causes of acute/sudden vision loss follow a useful clinical pattern:
| Presentation | Most Likely Cause |
|---|---|
| Painful, with halos, nausea | Acute angle-closure glaucoma |
| Painless, sudden, monocular (cherry-red spot) | Central retinal artery occlusion |
| Painless, flashes and curtain | Retinal detachment |
| Painless, older adult with headache/jaw pain | Temporal arteritis / ischemic optic neuropathy |
Key Points
- Globally: Cataract (#1), uncorrected refractive error (#2), glaucoma (#3)
- In the US (age-related): AMD, cataract, diabetic retinopathy, glaucoma
- Working-age adults (20-64): Diabetic retinopathy is the leading cause
- Elderly (65+): AMD is the leading cause
- Most causes are preventable or treatable if detected early - routine eye screening is essential, especially in diabetics, hypertensives, and those with a family history of glaucoma
Sources: Textbook of Family Medicine 9e | Robbins & Kumar Basic Pathology | Goldman-Cecil Medicine | CDC Vision Health | WHO / Prevent Blindness
Create a clinical decision summary PDF for diagnosing sudden vision loss
Reading File
Reading File
Running Command
Running Command
Writing File
Running Command
Editing File
Running Command
Running Command
The PDF has been generated successfully. Here's your download link:
Sudden Vision Loss Clinical Decision Summary
PDF Document · PDF
Here's what's included across the 4 pages:
Page 1 - Assessment & Differential Diagnosis
- Red-flag emergency banner
- Initial rapid assessment checklist (history + examination, including RAPD test)
- Full differential diagnosis table (13 conditions) organized by pain/laterality with urgency coding (EMERGENCY / URGENT)
Page 2 - Diagnostic Pathway & Investigations
- Step-by-step decision flowchart: transient vs. persistent → monocular vs. binocular → painful vs. painless - each branch with specific diagnoses and first actions
- Investigations table (14 tests): tonometry, fundoscopy, ESR/CRP, MRI, carotid Doppler, OCT, fluorescein angiography, etc. with key expected findings
Page 3 - Management & Fundoscopy
- Condition-specific emergency management for 6 major causes (acute glaucoma, CRAO, GCA/ION, retinal detachment, optic neuritis, wet AMD) with specific drug doses and timelines
- Visual field defect localization table (8 patterns matched to anatomical lesion)
- Key fundoscopic signs table (10 signs with appearances and diagnoses)
Page 4 - Special Populations & Disposition
- Drug-induced visual loss (9 drugs: ethambutol, HCQ, amiodarone, topiramate, etc.)
- Special population considerations: paediatric, pregnancy, elderly, diabetics, HIV/immunocompromised
- Three-column disposition guide: admit now / same-day referral / routine follow-up
- Disclaimer
This is a shared conversation. Sign in to Orris to start your own chat.