Ascitis from sleisenger and fordtran’s gastroenterology book
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive content from the chapter. Let me compile the full answer.
Ascites — Sleisenger and Fordtran's Gastrointestinal and Liver Disease (Chapter 93)
Definition and Epidemiology
Ascites is the abnormal accumulation of fluid in the peritoneal cavity. In Western countries, cirrhosis accounts for over 80% of cases. Remaining causes include heart failure, malignancies, tuberculosis, and pancreatic disease.
Ascites is the most frequent complication of cirrhosis, developing in approximately 60% of patients within 10 years of a diagnosis of compensated cirrhosis. It is associated with:
- Impaired health-related quality of life
- Increased risk of SBP, hyponatremia, and AKI
- Poor survival: 5-year survival ~30% with ascites vs. ~80% in compensated cirrhosis
Pathogenesis of Ascites in Cirrhosis
The key mechanism is renal sodium retention, driven by activation of the:
- RAAS (renin-angiotensin-aldosterone system)
- SNS (sympathetic nervous system)
This causes extracellular fluid volume expansion, leading to ascites and edema.
1. Sodium Retention and ECF Volume Expansion
- Earliest and most frequent renal abnormality in cirrhosis
- Sodium is retained isosmotically with water
- Ascites develops when urinary sodium excretion < dietary sodium intake
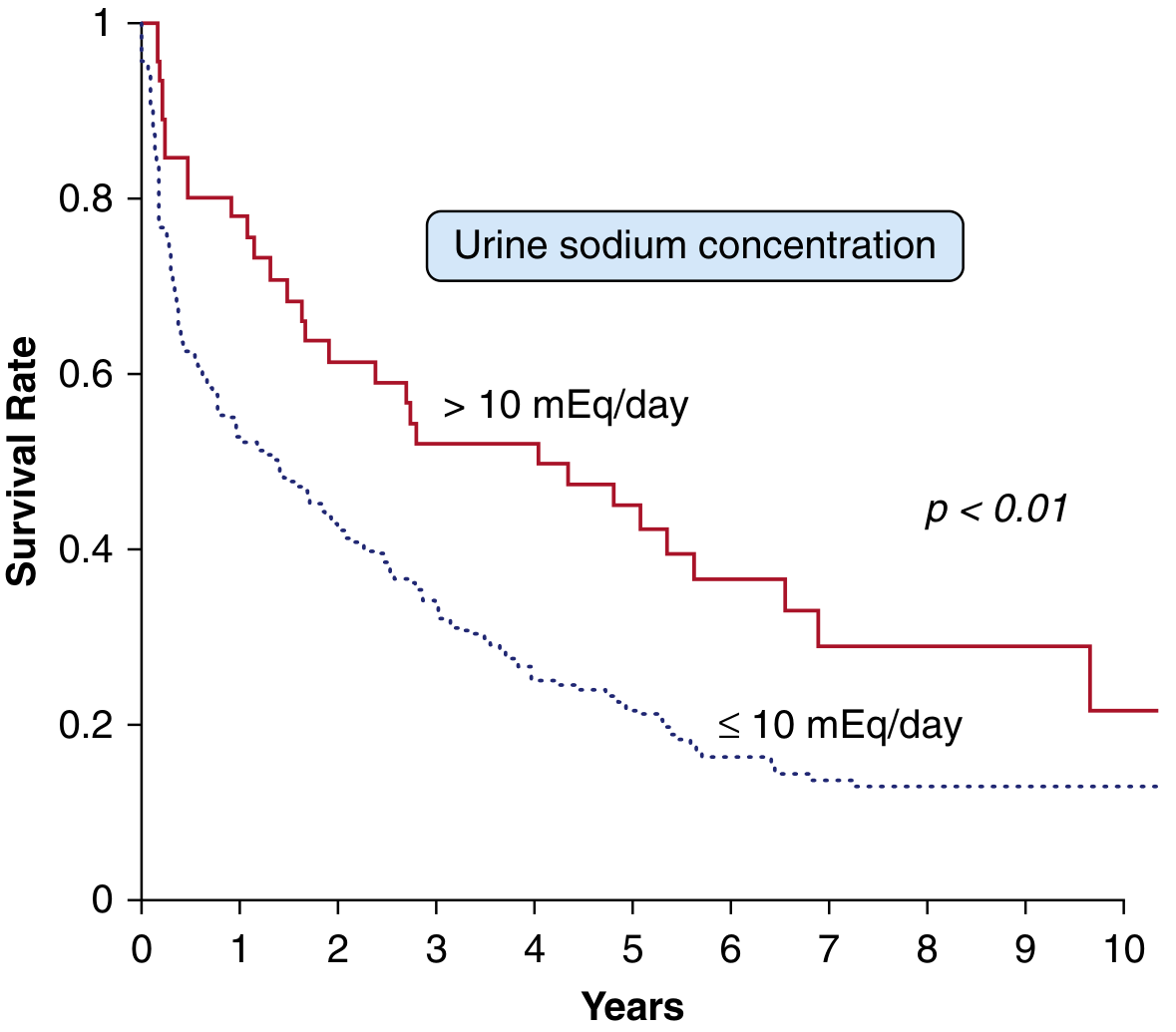
- Degree of sodium retention varies widely: patients with urine Na <10 mEq/day have marked retention and worse prognosis
- Goal of pharmacologic therapy: achieve negative sodium balance
2. Portal Hypertension
- Portal hypertension triggers splanchnic vasodilation
- Leads to underfilling of the systemic circulation
- Activates neurohumoral systems (RAAS, SNS, ADH), causing renal sodium and water retention
3. Systemic Circulatory Dysfunction
- Splanchnic arterial vasodilation causes "underfilling" of the effective arterial blood volume
- Results in:
- Impaired ability to excrete sodium
- Impaired ability to excrete solute-free water (causing dilutional hyponatremia)
- Reduced GFR via renal vasoconstriction (leading to hepatorenal syndrome in advanced disease)
- Chronological progression: sodium retention (earliest) → dilutional hyponatremia → HRS (most advanced)
4. Systemic Inflammation
- Chronic systemic inflammatory state further impairs circulatory function
- Contributes to kidney dysfunction and multiorgan failure in advanced cirrhosis
Diagnosis
Clinical Assessment
All patients with a first episode of ascites should have:
- Medical history and physical examination
- Standard blood tests
- Abdominal ultrasound
Laboratory Tests
- Urine sodium excretion: Predicts diuretic response. Patients with urine Na ≥10 mEq/day respond better to lower diuretic doses. Urine Na <10 mEq/day = median survival only 1.5 years vs. 4.5 years with ≥10 mEq/day.
Fig. 93.3 - Survival by Urine Sodium:
Abdominal Ultrasound
- First-line imaging for all patients with first-episode ascites
- Evaluates liver parenchyma, portal vein and suprahepatic vein patency, and rules out liver tumor
- Also indicated for known ascites with unexplained loss of treatment response
Ascitic Fluid Analysis
Diagnostic paracentesis (1.5-inch, 22-gauge needle; longer in obese) should be performed in:
- All patients with first episode of grade 2 or 3 ascites
- All patients with ascites admitted to hospital for any intercurrent complication
Mandatory tests on ascitic fluid:
| Test | Clinical significance |
|---|---|
| Neutrophil (PMN) count | PMN >250/mm³ = diagnostic of SBP |
| Total protein | <1.5 g/dL = increased SBP risk |
| Albumin | For SAAG calculation |
| Culture | Inoculate ≥10 mL into blood culture bottles immediately |
Serum-Ascites Albumin Gradient (SAAG):
- SAAG = serum albumin - ascitic fluid albumin (subtraction, NOT a ratio)
- SAAG ≥1.1 g/dL = portal hypertension (accuracy ~97%) — includes cirrhosis, cardiac ascites
- SAAG <1.1 g/dL = non-portal hypertension cause (peritoneal carcinomatosis, TB peritonitis, pancreatic ascites)
Additional tests based on suspicion:
- Suspected secondary bacterial peritonitis: ascitic glucose (near 0 mg/dL in secondary peritonitis), LDH (several-fold above serum), Gram stain (polymicrobial)
- Suspected malignancy: cytology (positive for peritoneal tumor, negative if tumor confined to liver)
- Suspected TB: mycobacterial culture
- Suspected pancreatic ascites: amylase/lipase
Grading of Ascites
| Grade | Description |
|---|---|
| Grade 1 | Mild, detected only on US |
| Grade 2 | Moderate, detectable by clinical examination |
| Grade 3 | Large/tense ascites with abdominal distension |
Differential Diagnosis
Up to 20% of ascites cases are non-cirrhotic. Key differentials:
| Cause | SAAG | Ascitic protein | Distinguishing features |
|---|---|---|---|
| Cirrhosis | ≥1.1 g/dL | Low (<2.5 g/dL) | Low Hct, low platelets, signs of chronic liver disease |
| Heart failure | ≥1.1 g/dL | High (≥2.5 g/dL) | Dyspnea persists after LVP, cardiomegaly on CXR |
| Peritoneal malignancy | <1.1 g/dL | High | Positive cytology |
| TB peritonitis | <1.1 g/dL | High | ADA elevated, mycobacterial culture |
| Pancreatic ascites | <1.1 g/dL | High | Very high amylase in fluid |
| Budd-Chiari | ≥1.1 g/dL | Variable | Hepatic vein occlusion on imaging |
Complications of Ascites
- Spontaneous Bacterial Peritonitis (SBP) - most important (see below)
- Refractory ascites - 10% of patients develop this; median survival ~6 months
- Hepatorenal Syndrome (HRS)
- Hepatic hydrothorax - accumulation of fluid in pleural space via diaphragmatic defects; median survival ~1 year; MELD underestimates prognosis
- Abdominal wall hernias (umbilical/inguinal) - occur in up to 20% of refractory ascites patients; risks: incarceration, perforation
Management of Ascites in Cirrhosis
Goal: Achieve negative sodium balance (reduce Na intake + increase urinary Na excretion).
Grade 1 Ascites
- No treatment recommended (insufficient data on natural history)
Grade 2 (Moderate) Ascites
- Managed in outpatient setting
- Most have urine Na >20 mEq/L at baseline
- Dietary sodium restriction: 80-120 mEq/day (4.6-6.9 g salt/day) - more stringent restriction is poorly tolerated and may worsen malnutrition
- Diuretics (first-line):
- Spironolactone (anti-mineralocorticoid): 100 mg/day, can increase to 400 mg/day
- Furosemide (loop diuretic): often combined, starting at 40 mg/day, up to 160 mg/day
- Combination preferred: maintains normokalemia; spironolactone:furosemide ratio 100:40 maintained throughout
- Response target: weight loss of 0.5 kg/day (no edema) or 1 kg/day (with edema)
- Monitor: serum creatinine, Na, K during therapy
Diuretic side effects and management:
| Side effect | Associated drug | Management |
|---|---|---|
| Hyponatremia | Loop diuretics > anti-mineralocorticoids | Withhold if Na <125 mEq/L |
| Hyperkalemia | Anti-mineralocorticoids | Stop if K >5.5 mEq/L |
| Hypokalemia | Furosemide | Stop if K <3 mEq/L |
| Painful gynecomastia | Spironolactone | Reduce dose or switch to amiloride |
| Muscle cramps | Both | Albumin infusion, baclofen |
| AKI | Both | Withhold diuretics |
| HE | Both | Withhold diuretics |
Grade 3 (Tense) Ascites
- Large-Volume Paracentesis (LVP) is first-line treatment
- Must be accompanied by IV albumin infusion to prevent post-paracentesis circulatory dysfunction (PPCD):
- 6-8 g albumin per liter of ascites removed when >5 L removed
- For <5 L: alternative plasma expanders may be acceptable, but albumin preferred
- After LVP: restart diuretic therapy + sodium restriction to prevent recurrence
Refractory Ascites
Definition: Ascites that cannot be mobilized or prevented from recurring despite:
- Maximum diuretic doses, OR
- Diuretic-related complication preventing effective dosing
Diagnostic Criteria (Box 93.5):
- Diuretic-resistant: No response to spironolactone 400 mg/day + furosemide 160 mg/day with Na restriction
- Diuretic-intractable: Diuretic-induced complications preclude effective dosing
Affects ~10% of patients with cirrhosis and ascites. Median survival ~6 months - all patients should be evaluated for liver transplantation.
Treatment options:
1. LVP + Albumin
- First-line for refractory ascites
- Repeated as needed; patient typically requires paracentesis every 2-4 weeks
2. Diuretics in Refractory Ascites
- Should generally be stopped once refractory ascites develops to prevent adverse events
3. TIPS (Transjugular Intrahepatic Portosystemic Shunt)
- Connects intrahepatic portal branch to hepatic vein outflow → decompresses portal system
- Improves effective blood volume and renal hemodynamics → increases urinary Na excretion
- Evidence: 6 RCTs + 7 meta-analyses show TIPS > LVP for control of recurrent/refractory ascites
- Survival benefit: TIPS improves survival in recurrent ascites but NOT in refractory ascites
- Covered stents preferred (reduce TIPS dysfunction and hepatic encephalopathy)
- HE risk: up to 50% with uncovered stents; reduced with covered stents
TIPS contraindications:
- Serum bilirubin >3 mg/dL
- Platelet count <75,000/mm³ (especially <20,000/mm³)
- Grade >2 or chronic hepatic encephalopathy
- Multiple hepatic cysts
- Unrelieved biliary obstruction
- Active infection
- Progressive renal failure
- Severe systemic or diastolic cardiac dysfunction
- Pulmonary hypertension
4. Hepatic Hydrothorax Management
- Thoracentesis for diagnosis and symptomatic relief
- Same medical treatment as ascites (Na restriction + diuretics)
- Chest tube drainage contraindicated (risk of complications)
- TIPS can be considered in selected cases
- LT is the definitive treatment
Contraindicated Drugs in Cirrhotic Ascites
- NSAIDs: Cause renal vasoconstriction and sodium retention; precipitate AKI and HRS
- ACE inhibitors / ARBs: Cause hypotension and AKI in cirrhosis
- Alpha-1 adrenergic blockers (e.g., prazosin): Worsen circulatory dysfunction
- Aminoglycosides: Nephrotoxic
Spontaneous Bacterial Peritonitis (SBP)
Pathogenesis
SBP develops from bacterial translocation - passage of intestinal bacteria (primarily gram-negative) from the gut lumen to mesenteric lymph nodes and then into the systemic circulation and ascites. Risk is highest when ascitic protein <1.5 g/dL.
Diagnosis
- PMN count >250/mm³ in ascitic fluid = diagnostic of SBP
- Culture should be performed (monomicrobial = SBP; polymicrobial = suspect secondary bacterial peritonitis)
- Most common organisms: Escherichia coli, Klebsiella pneumoniae, Streptococcus pneumoniae
Treatment
- Cefotaxime 2g IV q8h x 5 days (antibiotic of choice)
- IV albumin 1.5 g/kg at diagnosis + 1 g/kg on day 3 → prevents HRS and reduces mortality
Prophylaxis
- Primary prophylaxis: Indicated when ascitic protein <1.5 g/dL AND (serum creatinine ≥1.2 mg/dL OR BUN ≥25 mg/dL OR serum Na ≤130 mEq/L OR Child-Pugh ≥9 + bilirubin ≥3 mg/dL)
- Secondary prophylaxis (after first SBP episode): Norfloxacin 400 mg/day indefinitely (or ciprofloxacin/trimethoprim-sulfamethoxazole)
- Short-term prophylaxis (GI hemorrhage): IV ceftriaxone 1g/day x 7 days
Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chapter 93
This is a shared conversation. Sign in to Orris to start your own chat.