Explain Osteoporosis, osteomalacia,rickets in physiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive content from Ganong's Physiology, Robbins Pathology, and Tietz to write a thorough, well-structured answer. Let me compile the full explanation.
Osteoporosis, Osteomalacia, and Rickets - A Physiological Explanation
1. OSTEOPOROSIS
Definition
Osteoporosis is a condition of decreased bone mass where bone is structurally and histologically normal but simply reduced in quantity - making it susceptible to fracture. Radiographically it is diagnosed when bone mass falls 2.5 standard deviations below peak bone mass (T-score ≤ -2.5); between -1 and -2.5 SD is termed osteopenia.
Normal Bone Remodeling (Background)
Bone is constantly remodeled by two opposing cell types:
- Osteoclasts - resorb and erode bone
- Osteoblasts - synthesize new bone matrix (osteoid) and mineralise it
In health, these are tightly coupled. Osteoporosis arises when osteoclast activity exceeds osteoblast activity, resulting in net bone loss.
Pathogenesis
The key pathogenic mechanisms are illustrated below:
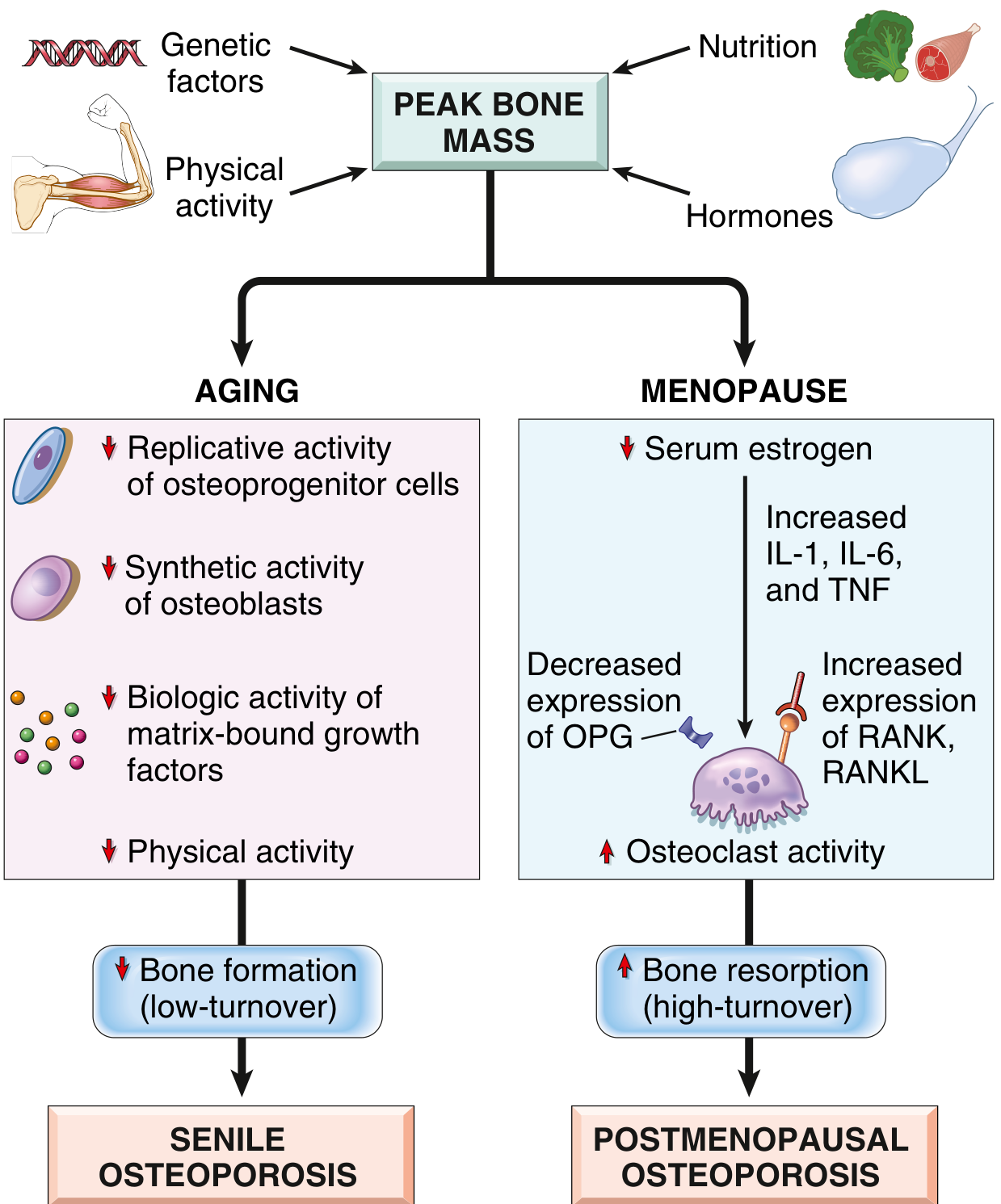
A. Postmenopausal Osteoporosis (High-Turnover)
- Estrogen deficiency is the primary driver
- Estrogen normally: inhibits secretion of pro-osteoclast cytokines (IL-1, IL-6, TNF-α), stimulates apoptosis of osteoclasts, and suppresses RANKL
- With estrogen loss: IL-6, TNF, IL-1 increase → increased RANKL expression, decreased osteoprotegerin (OPG) → osteoclast recruitment and activity surge
- Up to 2% cortical bone and 9% cancellous bone lost per year in the first decade post-menopause
- ~40% of postmenopausal women are affected
B. Senile Osteoporosis (Low-Turnover)
- Age-related decline in osteoprogenitor cell replication
- Reduced synthetic activity of osteoblasts and diminished response to growth factors
- Reduced physical activity (osteocytes sense mechanical load and regulate osteoblast/osteoclast balance)
- Calcium deficiency + reduced vitamin D + secondary hyperparathyroidism
C. Disuse Osteoporosis
- Immobilisation or space flight: bone resorption exceeds formation
- PTH and 1,25-dihydroxycholecalciferol fall; large amounts of calcium are lost in urine
- Plasma calcium not markedly elevated (renal excretion compensates)
D. Genetic Factors
- Polymorphisms in RANK, RANKL, OPG, HLA locus, estrogen receptor gene
- Determine peak bone mass attained in young adulthood
Morphology
- Histologically normal bone, but reduced in quantity
- Postmenopausal: mainly affects cancellous (trabecular) bone - vertebral bodies most severely hit
- Trabecular plates become perforated, thinned, lose interconnections → microfractures → vertebral collapse
- Senile: both cortical and cancellous bone thinned
Clinical Features
- Vertebral compression fractures (most common), hip fractures (most morbid), Colles (distal radius) fractures
- Loss of height, kyphosis ("dowager's hump")
- Often asymptomatic until fracture
Treatment Highlights
- Bisphosphonates (inhibit bone resorption - first-line)
- Raloxifene (SERM - mimics estrogen on bone without uterine/breast risk)
- Teriparatide (PTH analogue - stimulates bone formation)
- Calcitonin
- Weight-bearing exercise, calcium, vitamin D supplementation
Source: Ganong's Review of Medical Physiology, 26th Ed.; Robbins & Kumar Basic Pathology
2. RICKETS AND OSTEOMALACIA
Key Distinction
| Feature | Rickets | Osteomalacia |
|---|---|---|
| Age group | Children | Adults |
| Fundamental defect | Defective mineralisation at growth plates | Defective mineralisation of bone matrix during remodelling |
| Result | Interference with bone deposition in growth plates, bowing | Unmineralized matrix (osteoid) accumulates, fracture predisposition |
Both are fundamentally the same defect - impaired mineralisation - occurring in different skeletal contexts.
Core Physiology: Why Mineralisation Fails
Bone mineralisation requires adequate Ca²⁺ and PO₄³⁻ delivered to mineralisation sites. Vitamin D (specifically 1,25-dihydroxycholecalciferol = calcitriol) is essential for this:
- Promotes intestinal Ca²⁺ absorption
- Promotes renal Ca²⁺ and PO₄³⁻ retention
- Directly promotes mineralisation
The primary defect is failure to deliver adequate Ca²⁺ and PO₄³⁻ to sites of mineralisation, not merely vitamin D deficiency per se. The accumulation of unmineralized osteoid is the hallmark finding.
Causes
1. Vitamin D Deficiency (most common)
- Inadequate sunlight exposure (sun acts on 7-dehydrocholesterol in skin to form cholecalciferol/D₃)
- Inadequate dietary intake
- Malabsorption (celiac disease, Crohn's, postgastrectomy, hepatobiliary disease)
- At-risk groups: breast-fed infants, elderly, strict vegetarians, dark-skinned individuals
2. Disorders of Vitamin D Metabolism
- Liver disease: impaired 25-hydroxylation (first step)
- Kidney disease: impaired 1α-hydroxylation (second step to produce active 1,25-OH₂D)
- Responds to 1,25-dihydroxycholecalciferol but NOT to vitamin D itself
3. Type I Vitamin D-Resistant Rickets (Vitamin D-Dependent Rickets Type 1)
- Inactivating mutation in the gene for renal 1α-hydroxylase
- Cannot convert 25-OH-D to active calcitriol
- Responds normally to 1,25-OH₂D administration
- Presents in infancy
4. Type II Vitamin D-Resistant Rickets (Vitamin D-Dependent Rickets Type 2)
- Inactivating mutations in the Vitamin D Receptor (VDR) gene
- Deficient response to BOTH vitamin D and 1,25-dihydroxycholecalciferol
- Very high plasma 1,25-OH₂D levels (receptor resistance)
5. Phosphate Depletion
- X-linked hypophosphatemic rickets (most common rickets in USA): X-linked dominant, FGF23-mediated renal phosphate wasting
- Tumor-induced osteomalacia (FGF23 secretion by mesenchymal tumors)
- Fanconi syndrome (generalized tubular dysfunction)
6. Calcium Deficiency (developing countries)
- Dietary calcium deprivation → rickets without clear vitamin D or phosphate deficiency
7. Drug-Induced
- Anticonvulsants: increased hepatic catabolism of vitamin D metabolites
- Phosphate-binding antacids: prevent intestinal phosphate absorption
- Etidronate: direct mineralisation defect
Clinical Features
Rickets (Children):
- Bowing of weight-bearing bones (femur, tibia - classic "bow legs")
- Short stature
- Dental defects
- Rachitic rosary: costochondral junction swelling (beading of ribs)
- Harrison's sulcus: indentation of the lower ribs (diaphragmatic pull)
- Flattening of the skull (craniotabes)
- Widening and cupping/fraying of epiphyseal plates on X-ray
- Hypocalcemia, hypophosphatemia
Osteomalacia (Adults):
- Bone pain (most common symptom)
- Muscle weakness
- Stress fractures and frank fractures
- Pseudofractures (Looser zones) - characteristic radiolucent lines on X-ray, perpendicular to bone surface
- Waddling gait
Biochemical Profile
| Lab | Finding |
|---|---|
| Serum Ca²⁺ | Low or normal |
| Serum PO₄³⁻ | Low |
| Serum PTH | Elevated (secondary hyperparathyroidism) |
| Serum ALP | Elevated (osteoblast activity) |
| 25-OH-D | Low (in nutritional deficiency) |
| 1,25-OH₂D | Variable |
Treatment
- Nutritional rickets: vitamin D supplementation + adequate calcium intake; milk fortification with vitamin D has largely eliminated rickets in developed countries
- Type I VDDR: 1,25-dihydroxycholecalciferol (calcitriol)
- Type II VDDR: high-dose calcitriol (limited efficacy due to receptor defect)
- X-linked hypophosphatemic rickets: oral phosphate + calcitriol
- Orthopedic surgery for severe bowing in children
- Routine vitamin D milk supplementation has greatly reduced rickets in Western countries, but it remains one of the most common childhood diseases in developing countries
Sources: Ganong's Review of Medical Physiology, 26th Ed.; Robbins & Kumar Basic Pathology; Tietz Textbook of Laboratory Medicine, 7th Ed.
QUICK COMPARISON TABLE
| Feature | Osteoporosis | Osteomalacia / Rickets |
|---|---|---|
| Core defect | Reduced bone mass | Defective mineralisation of bone matrix |
| Bone quality | Normal mineralisation, less bone | Normal bone quantity, under-mineralised |
| Main cause | Estrogen deficiency, aging | Vitamin D deficiency, phosphate depletion |
| Serum Ca²⁺ | Normal | Low (or normal in phosphate type) |
| Serum ALP | Normal or mildly elevated | Elevated |
| PTH | Normal or mildly elevated | Elevated (secondary hyperPTH) |
| X-ray | Thinned trabeculae, fractures | Looser zones (adults), cupped epiphyses (children) |
| Who gets it | Postmenopausal women, elderly | Children (rickets), adults (osteomalacia) |
| Treatment | Bisphosphonates, SERMS, exercise | Vitamin D, calcium, phosphate |
Key Physiological Summary:
- Osteoporosis = the right bone, but not enough of it (a quantity problem)
- Osteomalacia/Rickets = enough bone matrix laid down, but it never gets properly hardened (a quality/mineralisation problem)
- Both ultimately relate to the Ca²⁺/PO₄³⁻/Vitamin D/PTH homeostasis axis, but at different points in bone physiology
This is a shared conversation. Sign in to Orris to start your own chat.