Teach me Audiometry in detail from scratch for my third year pg exam of ENT. Also include various types of Audiometry in detail
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Searching Images
audiogram types conductive sensorineural mixed hearing loss
I now have comprehensive content from the ENT textbooks. Let me compile this into a detailed, exam-ready guide.
🎧 Audiometry — Complete PG ENT Exam Guide
Sources: K J Lee's Essential Otolaryngology | Cummings Otolaryngology Head and Neck Surgery
1. INTRODUCTION & BASIC CONCEPTS
Audiometry is the science of measuring hearing sensitivity and diagnosing auditory disorders. It forms the cornerstone of any otological evaluation.
The Decibel (dB) Scale
- dB SPL (Sound Pressure Level): Absolute physical measure of sound intensity; reference 0.0002 dynes/cm²
- dB HL (Hearing Level): Clinically used; calibrated to average normal hearing thresholds at each frequency. "0 dB HL" = what a normal young adult barely hears at that frequency
- dB SL (Sensation Level): Intensity above the patient's own threshold
Frequency Range
- Human hearing: 20 Hz – 20,000 Hz
- Speech range: 500–3000 Hz (most critical)
- Standard audiometric test frequencies: 250, 500, 1000, 2000, 4000, 8000 Hz
- Inter-octave frequencies (1500, 3000, 6000 Hz) tested when ≥25 dB difference exists between adjacent octaves
Classification of Hearing Loss by Severity (dB HL)
| Degree | Threshold |
|---|---|
| Normal | ≤25 dB HL (adults); ≤15 dB HL (children) |
| Mild | 26–40 dB HL |
| Moderate | 41–55 dB HL |
| Moderately severe | 56–70 dB HL |
| Severe | 71–90 dB HL |
| Profound | >90 dB HL |
2. PURE-TONE AUDIOMETRY (PTA)
Principle
The foundation of audiometric testing. Measures hearing sensitivity to pure tones presented at specific frequencies.
Threshold = the lowest level at which a patient responds at least 50% of the time
Test Conditions
- Sound-treated booth (quiet enough to measure 0 dB HL thresholds)
- Calibrated equipment (complete calibration annually)
- Trained audiologist
- Otoscopic inspection prior to testing
- Clear instructions, patient comfort
Methods of Threshold Determination
- Modified Hughson-Westlake method (ascending): Standard clinical approach — decrease in 10 dB steps, increase in 5 dB steps; threshold = lowest level with ≥2/3 correct responses on ascent
- Test sequence: Better ear first → AC → BC if needed
Air Conduction (AC)
- Via earphones (supra-aural or insert)
- Tests entire auditory pathway: outer ear → middle ear → cochlea → auditory nerve → brainstem
- Symbols: O (right, unmasked), X (left, unmasked), △ (right, masked), □ (left, masked)
Bone Conduction (BC)
- Via bone oscillator placed on mastoid or forehead
- Bypasses outer and middle ear — tests only cochlea → auditory nerve → brainstem
- Symbols: < (right, unmasked), > (left, unmasked), [ (right, masked), ] (left, masked)
Air-Bone Gap (ABG)
- ABG = AC threshold − BC threshold
- ABG ≥ 10 dB is clinically significant
- Reflects conductive component of hearing loss (outer/middle ear pathology)
3. THE AUDIOGRAM — INTERPRETATION
Standard Symbols Table
| Symbol | Meaning |
|---|---|
| O | Right ear, AC, unmasked |
| X | Left ear, AC, unmasked |
| △ | Right ear, AC, masked |
| □ | Left ear, AC, masked |
| < | Right ear, BC, unmasked |
| > | Left ear, BC, unmasked |
| [ | Right ear, BC, masked |
| ] | Left ear, BC, masked |
Types of Audiograms
1. Normal Hearing
- All AC thresholds ≤25 dB HL (adults)
- No ABG; BC = AC
2. Conductive Hearing Loss (CHL)
- AC thresholds elevated (>25 dB HL)
- BC thresholds normal (≤25 dB HL)
- Significant ABG (≥10 dB)
- Causes: Otitis media with effusion, otosclerosis, tympanic membrane perforation, ossicular chain disruption
3. Sensorineural Hearing Loss (SNHL)
- Both AC and BC thresholds equally elevated
- No ABG (≤10 dB)
- Causes: Noise-induced, presbycusis, Ménière's disease, ototoxicity, acoustic neuroma
4. Mixed Hearing Loss
- Both AC and BC thresholds elevated
- AC > BC → ABG present
- Cause: Combination of conductive + sensorineural pathology
Special Audiometric Patterns
| Pattern | Description | Condition |
|---|---|---|
| Carhart notch | BC dip at 2000 Hz | Otosclerosis (impedance mismatch) |
| 4 kHz notch | AC dip at 4000 Hz | Noise-induced hearing loss (NIHL) |
| Flat | Equal loss across all frequencies | Otitis media with effusion |
| Cookie-bite | Mid-frequency loss (500–2000 Hz) | Genetic/hereditary SNHL |
| Low-frequency loss | Rising audiogram | Ménière's disease (early) |
| High-frequency loss | Falling audiogram | Presbycusis, ototoxicity |
Pure-Tone Average (PTA)
PTA = (AC at 500 + 1000 + 2000 Hz) ÷ 3
- Used to verify agreement with speech threshold (should be within ±10 dB)
4. MASKING
Why Mask?
When testing one ear, the sound can cross over through the skull and be heard by the non-test ear (NTE), giving a false response.
Interaural Attenuation (IA)
The reduction in sound as it travels from one side of the skull to the other:
- Supra-aural earphones (AC): 40–65 dB depending on frequency
- Insert earphones (AC): 70–90 dB (much less need for masking)
- Bone conduction: 0–10 dB (essentially no attenuation → mask BC almost always)
Rules for When to Mask
Rule A – Air Conduction:
Mask the NTE when:
AC stimulus level to test ear exceeds BC threshold of NTE by ≥40 dB (supra-aural) or ≥70 dB (insert earphones)
Rule B – Bone Conduction:
Mask the NTE when:
There is an ABG >10 dB in the test ear
Type of Masker Used
- For pure tones: Narrow-band noise (NBN) centered around the test frequency
- For speech: Speech-spectrum noise
5. SPEECH AUDIOMETRY
Speech audiometry assesses how well a patient processes speech, providing functional information beyond what pure-tone testing shows.
Components
A. Speech Awareness/Detection Threshold (SAT/SDT)
- Lowest level at which patient detects speech (not necessarily understands)
- Should be within 10 dB of the best pure-tone threshold anywhere in 250–8000 Hz range
- Used when SRT cannot be obtained (children, language barriers, disabilities)
B. Speech Recognition Threshold (SRT)
- Lowest level at which patient can repeat spondaic words correctly 50% of the time
- Spondee = two-syllable word with equal stress on both syllables (e.g., railroad, sidewalk, eardrum, icecream)
- Key rule: SRT should be within ±10 dB of the PTA
- Used to confirm pure-tone thresholds
C. Word Recognition Score (WRS) / Speech Discrimination Score (SDS)
- Percentage of phonetically balanced (PB) words correctly repeated at suprathreshold level (25–35 dB SL above SRT)
- Uses PB word lists (phonemes occur at same proportion as in normal English discourse)
- Presented via recorded material (CDs/digital) — NOT monitored live voice (less reliable)
WRS Interpretation Table
| Score | Interpretation |
|---|---|
| 90–100% | Normal |
| 76–88% | Slight difficulty |
| 60–74% | Moderate difficulty |
| 40–58% | Poor |
| ≤40% | Very poor |
Clinical Significance of WRS
- Rollover: WRS decreases at higher intensities → suggests retrocochlear lesion (acoustic neuroma)
- Disproportionately poor WRS relative to pure-tone loss → suggests retrocochlear pathology
- In Ménière's disease: WRS may fluctuate and be surprisingly poor during attacks
6. IMMITTANCE (IMPEDANCE) AUDIOMETRY
Objective tests of middle ear function. Does NOT require a behavioral response from the patient. Based on the concept of acoustic impedance/admittance at the tympanic membrane.
Impedance = energy rejected; Admittance = energy accepted. "Immittance" encompasses both.
6A. TYMPANOMETRY
Principle: Measures mobility (compliance) of the middle ear system as a function of applied air pressure in the ear canal.
- Probe tone: 226 Hz (standard); 1000 Hz in infants <6 months (more accurate in compliant neonatal canals)
- Compliance expressed as acoustic admittance (mmho or cm³/mL)
- Pressure expressed in daPa (dekapascals)
Tympanometric peak pressure (TPP): Pressure at which TM is most mobile = middle ear pressure
Normal peak pressure: −100 to +100 daPa (adults)
Tympanogram Types (Jerger Classification)
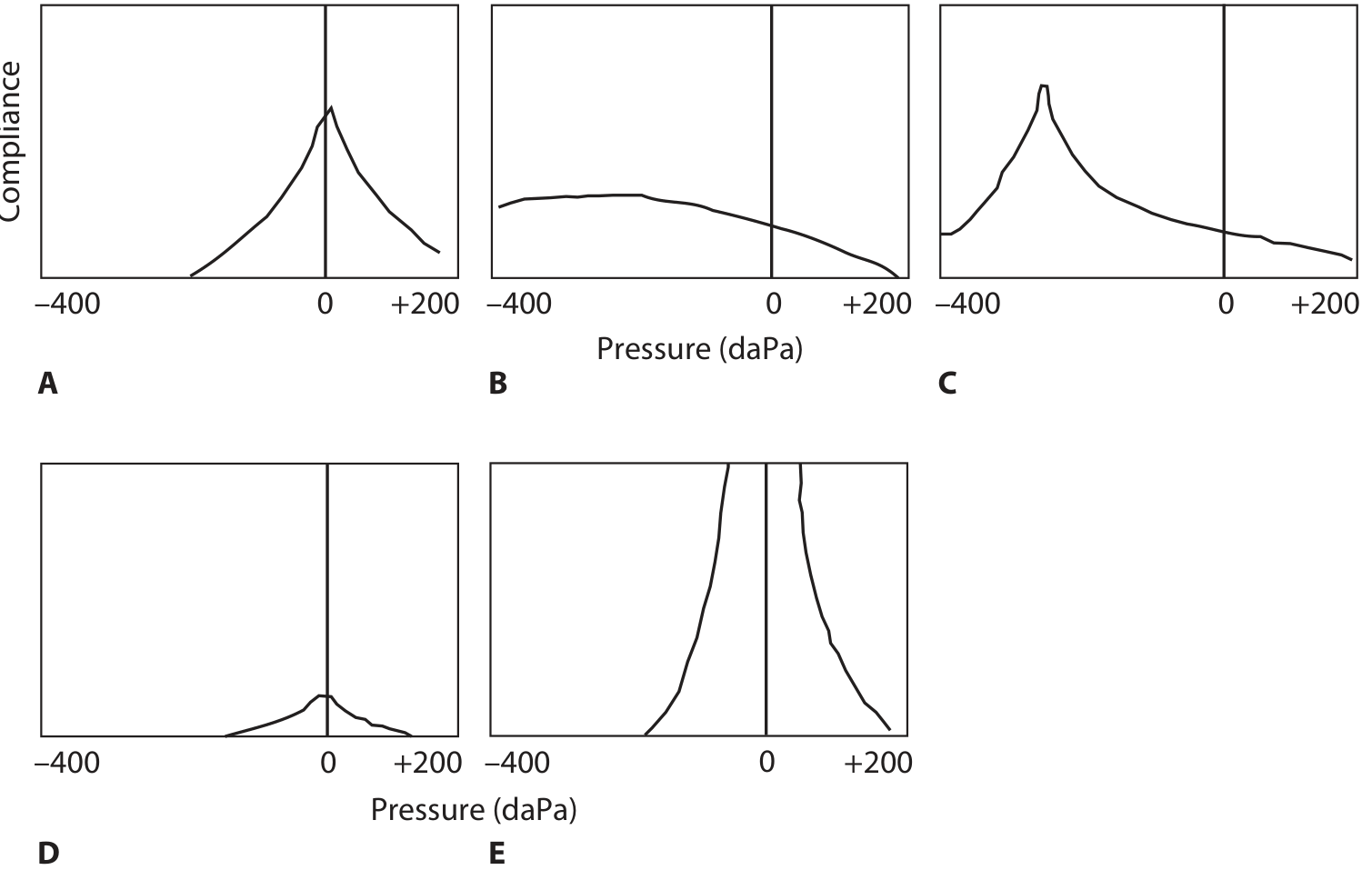
| Type | Shape | Compliance | Pressure | Clinical Association |
|---|---|---|---|---|
| A | Normal sharp peak | Normal | Normal (−100 to +100 daPa) | Normal middle ear |
| As (A-shallow) | Low/shallow peak | Reduced | Normal | Otosclerosis, tympanosclerosis, malleus fixation |
| Ad (A-deep) | Very high peak | Increased (hypercompliant) | Normal | Ossicular discontinuity, flaccid TM |
| B | Flat, no peak | Minimal | N/A | OME (fluid in middle ear), TM perforation (large ECV) |
| C | Peak shifted negative | Normal | < −100 daPa | Eustachian tube dysfunction, early OME |
ECV (Equivalent Ear Canal Volume):
- Normal: 0.6–1.5 cm³ (adults); 0.4–1.0 cm³ (children)
- High ECV + Type B = TM perforation or patent PE tube
- Low ECV = probe blocked against canal wall
6B. ACOUSTIC REFLEX TESTING
Principle: Loud sounds (≥70 dB SL) trigger contraction of the stapedius muscle (CN VII), stiffening the ossicular chain → measured as change in compliance.
Reflex arc: Sound → CN VIII → Superior olivary complex → CN VII nucleus → Stapedius muscle
Types of Reflexes:
- Ipsilateral reflex: Stimulus and probe in same ear
- Contralateral reflex: Stimulus in one ear, probe in other
Normal Acoustic Reflex Threshold (ART): 70–100 dB HL for pure tones
Acoustic Reflex Interpretation
| Finding | Clinical Significance |
|---|---|
| Absent ipsilateral + contralateral | CHL (probe ear), severe SNHL, CN VII lesion |
| Absent contralateral only | Lesion in crossed CN VIII/brainstem pathway |
| Present reflex with CHL | Rules out significant middle ear pathology |
| Reflex threshold elevated | Moderate-severe SNHL |
| Diphasic (on-off) reflex | Early stapedial fixation (otosclerosis) |
| Absent reflex (with normal audiogram) | Retrocochlear lesion |
Acoustic Reflex Decay
- Sustained tone at 10 dB above ART for 10 seconds
- Positive decay (>50% decrease in amplitude in ≤5 seconds) → CN VIII/retrocochlear lesion
- Key test for acoustic neuroma screening
7. OTOACOUSTIC EMISSIONS (OAE)
Principle: The outer hair cells (OHC) of the cochlea not only receive sound but actively vibrate, generating sounds that travel backward through the middle ear to the ear canal, where they can be recorded.
Pathway: OHC → Basilar membrane → Cochlear fluids → Oval window → Ossicles → TM → External canal → Microphone
Key Facts:
- Tests OHC function specifically — does not test inner hair cells, CN VIII, or central pathways
- Objective, non-invasive, no behavioral response needed
- Absent OAEs + normal ABR = central/neural lesion (Auditory Neuropathy)
- Present OAEs = cochlear hearing ≤30–40 dB HL (if retrocochlear is intact)
- Contraindicated/affected by: Middle ear pathology (fluid, perforation), ear canal debris
Types of OAE
A. Spontaneous OAE (SOAE)
- Present without any stimulus
- Found in ~35–60% of normally hearing individuals
- Absence is non-diagnostic (many normal ears have none)
- Rarely used clinically
B. Evoked OAE (EOAE)
i. Transient-Evoked OAE (TEOAE)
- Stimulus: Click or brief tone burst
- Response: Broad-frequency response (up to 4000 Hz)
- Present = cochlear function ≤30–40 dB HL
- Primary screening tool — used in Universal Neonatal Hearing Screening (UNHS)
- Low stimulus level (<30 dB SPL); requires quiet environment
ii. Distortion Product OAE (DPOAE)
- Stimulus: Two simultaneous pure tones (F1 and F2, with F2/F1 ratio ~1.2)
- The healthy cochlea generates a distortion product at 2F1–F2 frequency
- Stimulus levels: 55–65 dB SPL
- More frequency-specific than TEOAE
- Can sometimes be recorded even in moderate-to-severe hearing loss
- Used to monitor ototoxic drug effects (can detect early cochlear damage before threshold shifts occur)
OAE Summary Table
| Feature | TEOAE | DPOAE |
|---|---|---|
| Stimulus | Click | Two tones (F1, F2) |
| Main product | 2F1–F2 | 2F1–F2 |
| Frequency specificity | Low | High |
| Clinical use | Neonatal screening | Ototoxicity monitoring, frequency-specific cochlear assessment |
| Threshold correlate | >30–40 dB HL → absent | More sensitive |
8. ELECTRICAL RESPONSE AUDIOMETRY (ERA) / AUDITORY EVOKED POTENTIALS (AEP)
ERA records electrical potentials from the auditory pathway in response to sound. Used when behavioral tests are unreliable (infants, difficult-to-test patients).
Classification by Latency
| Category | Latency | Tests |
|---|---|---|
| Short-latency (<10 ms) | Cochlea + brainstem | ABR, ECoG |
| Middle-latency (10–50 ms) | Thalamo-cortical | MLR |
| Long-latency (>50 ms) | Cortical | CERA (N1-P2), P300, MMN |
8A. AUDITORY BRAINSTEM RESPONSE (ABR) / BERA / BAER
The most clinically important ERA.
Principle: Click or tone-burst stimuli evoke 5 waves (I–V) within 10 ms, representing sequential activation of auditory neural generators.
Stimulus: Click (broad spectrum, 2–4 kHz region) or tone burst (frequency-specific)
Recording: Surface electrodes (vertex positive, mastoid/earlobe negative)
ABR Wave Generators
| Wave | Generator |
|---|---|
| I | Distal end of CN VIII (cochlear) |
| II | Proximal CN VIII |
| III | Caudal brainstem (trapezoid body, superior olivary complex) |
| IV | Superior olivary complex |
| V | Lateral lemniscus → inferior colliculus |
| VI, VII | Inferior colliculus |
Most reliable waves: I, III, and V The I–V inter-peak latency is the key measure (~4 ms)
ABR — Clinical Applications
| Application | Details |
|---|---|
| Threshold ABR | Estimates hearing threshold (wave V tracked to lowest level); used in infants, non-cooperative patients |
| Neurologic ABR | High intensity (80–95 dB nHL); detects retrocochlear lesions; acoustic neuroma screening (90% sensitivity, 80% specificity) |
| Intraoperative monitoring | During posterior fossa/acoustic neuroma surgery |
| Neonatal screening | Automated ABR (AABR) used in UNHS |
ABR — Not Affected By:
Sedation, anesthesia, sleep state, most drugs → ideal for testing infants and uncooperative patients
ABR — Affected By:
Age, sex, body temperature, degree of hearing loss
ABR Abnormalities
| Finding | Interpretation |
|---|---|
| Absent all waves | Profound HL or no auditory function |
| Wave I present, V absent/delayed | Retrocochlear lesion |
| Prolonged I–V IPL | Acoustic neuroma, demyelination |
| No wave, but CM present | Auditory neuropathy spectrum disorder |
8B. ELECTROCOCHLEOGRAPHY (ECoG / ECochG)
Principle: Records electrical potentials from the cochlea and proximal CN VIII.
Three potentials recorded:
- Summating Potential (SP): DC potential from outer hair cells (>50%) and inner hair cells; represents receptor potential during sound stimulation
- Action Potential (AP / N1): From spiral ganglia and distal CN VIII afferents; equivalent to Wave I of ABR
- Cochlear Microphonic (CM): AC potential from outer hair cells; mirrors the acoustic waveform exactly
Key Measurement: SP/AP Ratio
- Normal: < 0.4 (or <40%)
- Elevated SP/AP ratio (>0.4) → Ménière's disease (endolymphatic hydrops)
- CM is used to differentiate auditory neuropathy
Electrode placement:
- Transtympanic (needle on promontory) — most accurate
- Extratympanic (ear canal) — less invasive
8C. AUDITORY STEADY-STATE RESPONSE (ASSR)
- Uses modulated tones at specific frequencies (500, 1000, 2000, 4000 Hz)
- Allows frequency-specific threshold estimation
- Can test multiple frequencies simultaneously
- Useful for fitting hearing aids in infants (predicts audiogram shape)
- Less affected by stimulus artifact than ABR clicks
8D. MIDDLE LATENCY RESPONSE (MLR)
- Latency: 10–50 ms
- Waves: Po, Na, Pa, Nb, Pb
- Generators: Thalamus (Na), Primary auditory cortex (Pa)
- Less commonly used clinically
- Useful in assessing auditory processing disorders and cortical hearing loss
8E. CORTICAL ELECTRIC RESPONSE AUDIOMETRY (CERA) — N1-P2
- Long-latency response (>50 ms)
- Generated in auditory cortex
- Waves: P1, N1, P2, N2
- Used for threshold estimation in cooperative patients, medicolegal assessment
8F. AUDITORY P300
- Latency ~300 ms
- Cognitive/event-related potential
- Tests auditory discrimination and cognitive processing
- Abnormal in dementia, auditory processing disorders
- Generator: Hippocampus (medial temporal lobe)
9. BEHAVIORAL AUDIOMETRY (Pediatric)
Since young children cannot perform standard audiometry, age-appropriate behavioral tests are used.
Age-Based Approach
| Age | Method |
|---|---|
| 0–6 months | Behavioral Observation Audiometry (BOA) |
| 6–30 months | Visual Reinforcement Audiometry (VRA) / COR |
| 30 months – 5 years | Conditioned Play Audiometry (CPA) |
| 5 years+ | Standard pure-tone audiometry |
A. Behavioral Observation Audiometry (BOA)
- Age: ≤6 months (neurodevelopmental age)
- No conditioning; observer watches for reflex responses (eye widening, startle, pause in activity, head turn)
- Sound field via loudspeakers or earphones
- Minimal Response Level (MRL) obtained — typically suprathreshold (not a true threshold)
- Limitations: Response fatigues rapidly, high inter-subject variability, unreliable
B. Visual Reinforcement Audiometry (VRA)
- Age: 6–30 months
- Child is operantly conditioned to turn head toward sound source, rewarded by animated toy/video
- Only requires head turn toward sound (does not need to localize direction)
- Insert earphones preferred (avoids collapsing canal)
- Conditioned Orienting Response (COR): Variant requiring correct direction localization (right sound → right head turn)
C. Conditioned Play Audiometry (CPA)
- Age: 30 months and above
- Game-based: Each tone → child performs play activity (drops block in bucket, places ring on peg)
- The game itself is the reinforcer
- By this age, most children tolerate earphones → ear-specific thresholds possible
10. SITE-OF-LESION TESTING
Tests to differentiate cochlear (sensory) vs. retrocochlear (neural) hearing loss.
Modern (Still Used)
| Test | Principle | Cochlear finding | Retrocochlear finding |
|---|---|---|---|
| Acoustic reflex decay | Sustained tone causes reflex to decay | No decay | Decay >50% in ≤5 sec |
| ABR | Inter-peak latency | Normal or mildly elevated | Prolonged I–V IPL; absent waves |
| OAE + ABR combination | OHC vs neural function | OAE absent + ABR present (sensory) | OAE present + ABR abnormal (neural = ANSD) |
Historical (No Longer Routinely Used)
| Test | Principle | Cochlear | Neural |
|---|---|---|---|
| ABLB (Alternate Binaural Loudness Balance) | Balance loudness between ears | Recruitment present | No recruitment |
| SISI (Short Increment Sensitivity Index) | Detects 1-dB increments | Score >70% (cochlear) | Score <30% (neural) |
| Tone Decay Test | Auditory adaptation to continuous tone | <25 dB decay | >25 dB decay |
| Bekesy Audiometry | Pulsed vs. continuous tone tracings | Type II | Type III/IV |
Bekesy Types
| Type | Tracing | Meaning |
|---|---|---|
| I | Continuous ≈ Pulsed (overlap) | Normal |
| II | Continuous 10–20 dB below pulsed | Cochlear lesion |
| III | Continuous drops dramatically >20 dB | Neural lesion (severe fatigue) |
| IV | Continuous consistently >20 dB below pulsed | Neural lesion |
| V | Continuous better than pulsed | Functional/nonorganic hearing loss |
11. AUDITORY NEUROPATHY SPECTRUM DISORDER (ANSD)
A distinct pattern:
- OAEs: Present (OHC intact)
- Cochlear Microphonic: Present
- ABR: Absent or severely abnormal (neural dyssynchrony)
- May or may not show threshold loss on PTA
- Speech understanding disproportionately poor
- Causes: Selective inner hair cell loss, synaptic dysfunction, CN VIII dyssynchrony
- Management: Cochlear implant (benefits more than hearing aids)
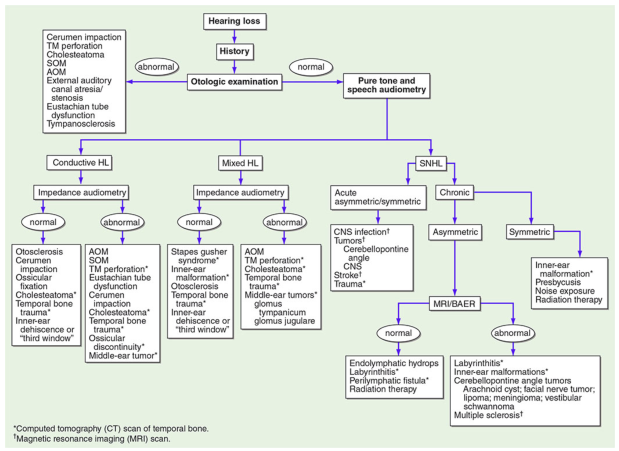
12. DIAGNOSTIC FLOWCHART (Harrison's Approach)
13. QUICK REVISION — HIGH-YIELD POINTS FOR PG EXAM
| Topic | Key Fact |
|---|---|
| Spondee | 2-syllable, equal-stress word (railroad, eardrum) |
| SRT vs PTA | Should agree within ±10 dB |
| Carhart notch | BC dip at 2000 Hz → otosclerosis |
| 4 kHz notch | Noise-induced hearing loss |
| Masking BC | Required when ABG >10 dB |
| Type B tympanogram | OME (normal ECV) vs. perforation (high ECV) |
| Type As | Otosclerosis, tympanosclerosis |
| Type Ad | Ossicular discontinuity |
| OAE absent + ABR normal | Not possible if cochlear; suggests neural |
| SP/AP ratio >0.4 | Ménière's disease (ECoG) |
| ABR wave V generator | Lateral lemniscus / inferior colliculus |
| ABR not affected by | Sedation, anesthesia, sleep |
| Rollover on WRS | Retrocochlear (acoustic neuroma) |
| Diphasic acoustic reflex | Early otosclerosis |
| ANSD pattern | OAE present + ABR absent |
| VRA age | 6–30 months |
| CPA age | 30 months + |
| BOA limitation | Response extinguishes quickly, suprathreshold only |
| DPOAE clinical use | Ototoxicity monitoring, frequency-specific OHC testing |
| AABR | Used in neonatal universal hearing screening |
14. SUMMARY OF AUDIOMETRY TYPES
| Type | Objective/Subjective | What It Tests | Key Use |
|---|---|---|---|
| Pure-Tone Audiometry | Subjective | Threshold sensitivity, AC & BC | Foundation of hearing assessment |
| Speech Audiometry (SRT, WRS) | Subjective | Speech detection, recognition, discrimination | Functional hearing, retrocochlear |
| Tympanometry | Objective | Middle ear pressure & compliance | OME, otosclerosis, perforation |
| Acoustic Reflex | Objective | Stapedius reflex arc integrity | CN VII/VIII, retrocochlear |
| OAE (TEOAE, DPOAE) | Objective | OHC function | Neonatal screening, ototoxicity |
| ABR/BERA | Objective | Auditory nerve + brainstem | Threshold in infants, acoustic neuroma |
| ECoG | Objective | Cochlear potentials (SP, AP, CM) | Ménière's, ANSD |
| ASSR | Objective | Frequency-specific cochlear sensitivity | Infant hearing aid fitting |
| MLR | Objective | Thalamo-cortical pathways | Auditory processing |
| CERA / P300 | Objective | Cortical processing | Medicolegal, cognitive assessment |
| BOA | Behavioral | Gross hearing in infants | <6 months |
| VRA / COR | Behavioral + conditioning | Threshold in toddlers | 6–30 months |
| CPA | Behavioral + conditioning | Threshold in young children | 30+ months |
| Bekesy Audiometry | Subjective (automated) | Auditory fatigue/adaptation | Site of lesion (historical) |
| SISI | Subjective | Recruitment | Site of lesion (historical) |
| Tone Decay | Subjective | Neural fatigue | Site of lesion (historical) |
Compiled from: K J Lee's Essential Otolaryngology (9781260122237) and Cummings Otolaryngology Head and Neck Surgery (9780323612173)
This is a shared conversation. Sign in to Orris to start your own chat.