Here is an exhaustive, fully detailed clinical guide on Diastasis Recti Abdominis (DRA) covering every requested domain.
DIASTASIS RECTI ABDOMINIS (DRA)
A Complete Clinical & Physiotherapy Reference
PART 1: FOUNDATIONAL ANATOMY
1.1 The Anterior Abdominal Wall
The anterior abdominal wall is a complex, multi-layered musculoaponeurotic structure responsible for:
- Containing and protecting abdominal viscera
- Generating and regulating intra-abdominal pressure (IAP)
- Transferring loads between the thorax, pelvis, and lower limbs
- Producing trunk flexion, rotation, and lateral bending
Layers from superficial to deep:
- Skin
- Subcutaneous fat (Camper's fascia)
- Scarpa's fascia
- External oblique muscle and aponeurosis
- Internal oblique muscle and aponeurosis
- Transversus abdominis (TrA) muscle and aponeurosis
- Transversalis fascia
- Preperitoneal fat
- Peritoneum
1.2 The Rectus Abdominis
- Two vertical, strap-like muscles running parallel to the midline
- Origin: Pubic crest and pubic symphysis
- Insertion: Costal cartilages of ribs 5, 6, 7 and xiphoid process
- Enclosed within the rectus sheath, formed by splitting aponeuroses of the three flat abdominal muscles
- Segmented by three to four tendinous intersections (giving the "six-pack" appearance)
- Function: Trunk flexion, posterior pelvic tilt, IAP regulation, stabilization
1.3 The Linea Alba — The Core Structure in DRA
The linea alba (Latin: "white line") is the central fibrous seam running vertically from the xiphoid process to the pubic symphysis, formed by the interdigitation and decussation of aponeurotic fibers from:
- External oblique (most superficial)
- Internal oblique (middle)
- Transversus abdominis (deepest)
Structural Properties
- Composed predominantly of type I collagen (tensile strength) and type III collagen (elasticity)
- Contains elastin fibers allowing stretch and recoil
- Has a three-dimensional cross-weave architecture that provides resistance to tensile, compressive, and shear forces
- Normal width:
- Above umbilicus: up to 15 mm at rest
- At umbilicus: up to 22 mm
- Below umbilicus: up to 16 mm
- The linea alba is an active load-transmitting structure, not merely passive connective tissue
Functional Significance
When the linea alba has adequate stiffness and tension, it:
- Transmits tensile forces across the midline between the two rectus muscles
- Allows efficient co-contraction of all abdominal muscles
- Maintains lumbopelvic stability during movement and loading
- Regulates IAP in coordination with the diaphragm and pelvic floor
In DRA, the linea alba widens, thins, and loses stiffness — these changes impair all of the above functions.
1.4 The Deep Stabilizing System ("Inner Unit")
This is the key system disrupted in DRA:
| Muscle | Role |
|---|
| Transversus abdominis (TrA) | Circumferential compressor; generates hoop tension; primary midline tensioner |
| Pelvic floor muscles | Inferior "base"; supports organs; pressure regulation |
| Diaphragm | Superior "lid"; primary respiratory muscle; IAP regulation |
| Multifidus | Segmental lumbar stabilizer; co-activates with TrA |
These four muscles fire tonically and anticipatorily before limb movements to pre-stiffen the spine and pelvis. In DRA, this coordination is disrupted.
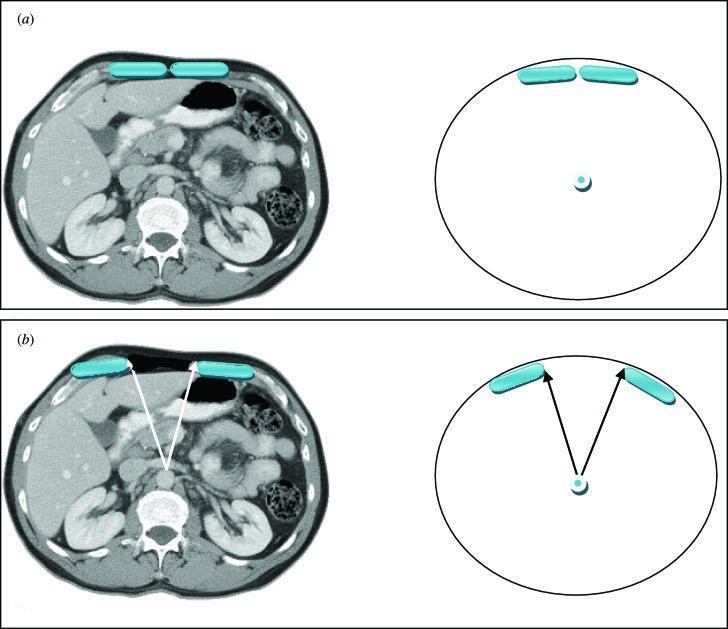
Axial CT scans: (a) Normal rectus abdominis with minimal linea alba gap; (b) Diastasis recti — significant lateral displacement of rectus muscles and widened inter-recti distance. The Component Separation Index (CSI) angle is markedly wider in diastasis. (Bailey & Love's Surgery, 28th Ed., p. 1079)
PART 2: DEFINITION & DIAGNOSTIC CRITERIA
2.1 Definition
Diastasis Recti Abdominis (DRA) is defined as the pathological separation of the two rectus abdominis muscles due to widening and structural weakening of the linea alba, resulting in impaired anterior abdominal wall function, reduced trunk stability, and a range of musculoskeletal and pelvic floor sequelae.
The term "divarication of the recti" is used interchangeably in surgical literature (Bailey & Love, 28th Ed., p.1079).
2.2 Diagnostic Threshold
| Measurement Site | Normal IRD | DRA Threshold |
|---|
| 4.5 cm above umbilicus | < 15 mm | ≥ 20 mm |
| At umbilicus | < 22 mm | ≥ 22 mm |
| 4.5 cm below umbilicus | < 16 mm | ≥ 16 mm |
Critical note: The inter-recti distance (IRD) alone is insufficient for diagnosis. The tension and stiffness of the linea alba is equally or more important functionally. A wide gap with good tension may be less disabling than a narrow gap with a flaccid, unstiff linea alba (Lee & Hodges, 2016).
2.3 DRA vs. Hernia
| Feature | DRA | Hernia |
|---|
| Gap content | No visceral herniation | Visceral herniation through defect |
| Peritoneal involvement | No | Yes |
| Risk of strangulation | No | Yes |
| Reducibility | N/A | Often reducible |
| Surgical urgency | Elective | May be urgent |
DRA can co-exist with umbilical or epigastric hernia — always exclude hernia during assessment.
PART 3: CAUSES & RISK FACTORS
3.1 Primary Etiological Mechanisms
A. Mechanical Stretching
The most straightforward mechanism. As the uterus enlarges during pregnancy, it pushes the abdominal wall forward and outward, placing sustained tensile load on the linea alba. This progressive stretch leads to:
- Plastic deformation of collagen fibers (permanent elongation beyond elastic limit)
- Widening and thinning of the linea alba
- Lateral displacement of rectus muscles
B. Hormonal Changes
During pregnancy, the body produces elevated levels of:
- Relaxin: Remodels collagen, increases ligament/tendon/fascia extensibility
- Progesterone: Further softens connective tissue
- Estrogen: Affects collagen synthesis and cross-linking
These hormones are adaptive (facilitate delivery) but cause the linea alba to become more extensible and less stiff, predisposing to DRA.
C. Elevated Intra-Abdominal Pressure (IAP)
Chronic or repetitive increases in IAP from any cause can stretch the linea alba:
- Obesity (chronic low-grade elevation)
- Heavy lifting (acute spikes)
- Chronic cough, constipation
- Pregnancy (sustained elevation)
D. Collagen Quality Deficiency
The structural integrity of the linea alba depends on:
- Adequate collagen cross-linking
- Proper type I:III collagen ratio (type I = strength; type III = early repair tissue, weaker)
- Elastin distribution
Conditions or states that reduce collagen quality increase DRA susceptibility.
3.2 Specific Risk Factors (Detailed)
Pregnancy-Related
| Risk Factor | Mechanism |
|---|
| Multiparity | Repeated mechanical stretching; cumulative collagen damage; each pregnancy adds to linea alba laxity |
| Multiple gestation (twins, triplets) | Greater uterine volume = greater mechanical distension |
| Macrosomia | Large fetus = greater abdominal distension |
| Polyhydramnios | Excess amniotic fluid = greater IAP and wall stretch |
| Rapid gestational weight gain | Accelerated mechanical loading |
| Short inter-pregnancy interval | Insufficient time for linea alba remodeling between pregnancies |
| Age > 35 | Reduced collagen quality and repair capacity |
| Caesarean section | Disrupts fascial planes; post-surgical adhesions alter abdominal wall mechanics |
| Vaginal instrumental delivery | Prolonged second stage = increased Valsalva and IAP |
Non-Pregnancy Related
| Risk Factor | Mechanism |
|---|
| Obesity (BMI > 30) | Chronic IAP elevation; visceral fat mechanically pushes abdominal wall outward; predominantly upper abdomen in middle-aged men (Bailey & Love, p.1079) |
| Male gender (middle-aged, overweight) | Upper abdominal DRA is classic in overweight males; hormonal factors absent but mechanical loading predominates |
| Connective tissue disorders | Ehlers-Danlos Syndrome: defective collagen (reduced cross-linking); Marfan Syndrome: FBN1 mutation affecting connective tissue |
| Previous abdominal surgery | Disrupted fascial architecture, adhesions, weakened repair zones |
| Chronic constipation / straining | Repeated Valsalva maneuver spikes IAP |
| Chronic obstructive pulmonary disease | Chronic cough = repeated IAP spikes |
| Heavy resistance training with improper technique | Valsalva maneuver without adequate abdominal bracing |
| Sedentary lifestyle | Poor intrinsic core muscle tone, reduced passive support |
| Genetics | Familial clustering reported; collagen gene variants may predispose |
| Neonatal / infant DRA | Normal developmental variant; rectus muscles not yet fused at midline; resolves spontaneously by 6–12 months in most cases |
3.3 Pathological Cascade
Mechanical load + Hormonal laxity
↓
Linea alba collagen fiber elongation and remodeling
↓
Increased inter-recti distance (IRD)
↓
Reduced linea alba stiffness and tension
↓
Impaired force transmission across midline
↓
Deep stabilizing system dysfunction
(TrA, pelvic floor, diaphragm, multifidus)
↓
Reduced lumbopelvic stability
↓
Low back pain + Pelvic girdle pain + Pelvic floor dysfunction
PART 4: CLINICAL FEATURES
4.1 Symptoms
Primary Complaint
Visible or palpable midline bulge/ridge along the abdomen — the most characteristic and distressing feature. The bulge appears as a dome or cone-shaped protrusion along the linea alba during:
- Sit-ups or curl-ups
- Rising from lying to sitting
- Coughing, sneezing, laughing
- Lifting or straining
This phenomenon is called "doming" or "coning" and represents herniation of abdominal contents through the weakened linea alba during increased IAP.
Musculoskeletal Symptoms
1. Lower Back Pain (LBP)
- One of the most prevalent and disabling symptoms
- Mechanism: Loss of deep stabilizing system function → excessive loading on passive structures (lumbar discs, facet joints, ligaments)
- Pain is typically dull, aching, postural; worse with prolonged standing, lifting, transitional movements
- Prevalence: Studies show ~50–70% of women with DRA report LBP
2. Pelvic Girdle Pain (PGP)
- Pain over sacroiliac joints, pubic symphysis, or general pelvic region
- Mechanism: Reduced force closure of the pelvis due to impaired abdominal wall function; cannot generate adequate tension through posterior and anterior pelvic ligaments
- Worsened by: walking, stair climbing, single-leg stance, rolling in bed
3. Abdominal Weakness and Fatigue
- Difficulty with functional tasks: getting up from bed, carrying children, lifting groceries
- Abdominal wall "gives out" feeling with sustained effort
- Unable to perform traditional abdominal exercises without doming
4. Hip and Gluteal Weakness
- Secondary to altered lumbopelvic stability; muscles around the hip work harder to compensate
- Piriformis, tensor fascia lata tightness common
Pelvic Floor Symptoms
(DRA and pelvic floor dysfunction are intimately linked — fascia from abdominal wall directly connects to pelvic floor)
5. Stress Urinary Incontinence (SUI)
- Leaking urine with cough, sneeze, jump, run
- Mechanism: Impaired IAP regulation; inability to pre-contract pelvic floor effectively
6. Urge Urinary Incontinence
- Sudden urgency with or without leakage
7. Pelvic Organ Prolapse (POP)
- Bladder (cystocele), rectum (rectocele), or uterine prolapse
- Mechanism: Reduced superior support from abdominal wall increases downward loading on pelvic floor
8. Dyspareunia — painful intercourse due to pelvic floor muscle hypertonia (overactive compensatory response)
9. Bowel dysfunction — constipation, incomplete evacuation, rectal pressure
General Symptoms
10. Abdominal Pain / Discomfort
- Pulling or aching sensation at midline
- Worse with activity, coughing, end of day
11. Bloating
- Altered IAP dynamics affect gastrointestinal motility
- Visceral contents bulge forward under reduced wall resistance
12. Breathing Difficulty
- Diaphragmatic excursion compromised by altered IAP dynamics
- Accessory muscle breathing patterns develop
13. Psychological Impact
- Body image disturbance; women feel their "stomach sticks out" despite weight loss
- Postpartum depression association reported
- Avoidance of exercise or intimacy
- Reduced quality of life
4.2 Signs (Objective Findings on Examination)
| Sign | Description |
|---|
| Palpable midline gap | Fingers sink into gap along linea alba when patient raises head; width measurable in finger-widths or centimeters |
| Doming/coning | Ridge or dome rises along midline during curl-up or cough |
| Flaccid linea alba | Tissue between recti feels soft, offers no resistance to palpation during activation |
| Reduced abdominal wall tension | Cannot generate taut anterior wall |
| Postural changes | Increased lumbar lordosis, anterior pelvic tilt, rib flare, forward head position |
| Altered breathing pattern | Paradoxical breathing, upper chest dominant, reduced lateral costal expansion |
| Trendelenburg gait | Pelvis drops on swing phase; hip abductors weak/over-loaded |
| Abdominal ptosis | Lower abdomen visually hangs forward |
| Umbilical deformity | Widened, flat, or everted umbilicus |
| Scar tissue | If post-caesarean: adhered suprapubic scar affecting fascial mechanics |
4.3 Classification Systems
By Location (Three-Level System)
| Level | Position | Clinical Significance |
|---|
| Supra-umbilical | 4.5 cm above umbilicus | Most common in men and non-pregnant individuals |
| Umbilical | At umbilicus | Hernia risk highest here |
| Infra-umbilical | 4.5 cm below umbilicus | Common postpartum; affects pelvic floor most |
| Combined (all three levels) | Full-length DRA | Most severe functional impairment |
By Severity (Clinical Grading)
| Grade | IRD | Tension | Functional Impact |
|---|
| Grade 1 (Mild) | 2.0–3.0 cm | Present but reduced | Minimal functional impairment |
| Grade 2 (Moderate) | 3.0–5.0 cm | Significantly reduced | Moderate LBP, pelvic dysfunction |
| Grade 3 (Severe) | > 5.0 cm | Absent | Severe dysfunction, hernia risk |
Lee & Hodges Functional Classification (2016)
This important classification emphasizes tension over width:
- Type 1: Wide IRD + Good tension → Functional; conservative management suitable
- Type 2: Normal/wide IRD + Poor tension → Dysfunctional; intensive rehabilitation or surgery
- Type 3: Wide IRD + Poor tension + Hernia → Surgical candidate
PART 5: SPECIAL TESTS
5.1 Clinical / Bedside Tests
TEST 1: Finger-Width Test (Head Lift Test / Curl-Up Palpation Test)
The most widely used clinical screening test
Setup: Patient supine, knees bent 90°, feet flat
Procedure:
- Examiner places index and middle fingers horizontally across the midline at three points:
- 4.5 cm above umbilicus
- At the umbilicus
- 4.5 cm below umbilicus
- Ask patient to perform a partial curl-up (lift only head and shoulders, chin tucked)
- Palpate the gap width and tissue tension simultaneously
Interpretation:
- Normal: Gap < 2 finger-widths (< 2 cm); linea alba taut
- Positive DRA: Gap ≥ 2 finger-widths (≥ 2 cm)
- Note texture: Taut (tension present) vs. soft/flaccid (no tension)
Limitations:
- Subjective; finger widths vary between examiners
- Does not quantify IRD accurately
- Poor inter-rater reliability
- Does not measure linea alba tension objectively
TEST 2: Doming / Coning Observation Test
Purpose: Identify pathological midline protrusion during abdominal activation
Procedure:
- Patient supine, knees bent
- Ask to slowly perform a curl-up
- Observe the midline for:
- Dome: rounded protrusion rising along midline (diastasis present)
- Cone: more acute protrusion (greater IAP spike)
- Flat midline: normal (no diastasis or well-controlled)
Clinical significance:
- Doming indicates the linea alba is not resisting IAP effectively
- Any exercise causing doming should be avoided or modified
- Doming is the primary exercise safety guide in DRA rehabilitation
TEST 3: Linea Alba Tension Test (Lee & Hodges, 2016)
Purpose: Qualitative assessment of linea alba stiffness — more clinically meaningful than IRD alone
Procedure:
- Locate the gap by palpation above the umbilicus
- Place fingertips into the gap at rest
- Ask patient to perform a head lift / curl-up
- Assess whether the tissue adjacent to your fingers becomes taut or remains soft
Interpretation:
| Finding | Clinical Meaning |
|---|
| Linea alba tightens → fingers are "pushed out" | Tension restored; good prognosis with conservative management |
| Linea alba remains soft/flaccid → fingers stay in gap | Poor tension; impaired load transfer; may need surgical consideration |
| Gap narrows + tension restored | Excellent; deep stabilizers functioning |
TEST 4: Active Straight Leg Raise (ASLR) Test
Purpose: Assess lumbopelvic force transfer and load management
Procedure:
- Patient supine, legs straight, 20 cm apart
- Ask: "Try to raise your right/left leg 20 cm off the table without bending the knee"
- Patient rates effort on scale 0–5 (0 = not difficult; 5 = impossible)
- Repeat with manual compression applied at ASIS bilaterally (simulates pelvic compression)
Interpretation:
- Positive: Difficulty raising leg, heaviness, pain, pelvic rotation
- Positive with improvement on compression: Confirms pelvic force closure deficit (classic in DRA + PGP)
- Assesses the entire lumbopelvic-hip unit, not just diastasis
TEST 5: Single Leg Stance Test
Purpose: Assess dynamic lumbopelvic stability and compensatory strategies
Procedure:
- Patient stands on one leg for 30 seconds
- Observe:
- Trunk lateral sway
- Pelvic drop (Trendelenburg sign)
- Hip hike or use of breath-holding to stabilize
Positive: Pelvic drop, trunk sway, compensatory breath-holding; suggests poor force closure
TEST 6: Heel Slide / Bent Knee Fall Out Test
Purpose: Assess ability to maintain neutral lumbar spine while loading abdominals
Procedure:
- Supine hook-lying, TrA gently activated
- Slowly slide one heel along the floor until leg straight OR allow one knee to fall out to the side
- Observe for: lumbar lordosis increase, pelvic rotation, breath-holding, midline doming
Positive: Loss of neutral spine control, compensatory breath-holding, doming
TEST 7: Plank Hold Test
Purpose: Functional assessment of sustained core stability (used in later-stage patients)
Procedure:
- Modified plank (knees down initially)
- Hold for up to 60 seconds
- Observe for: doming, inability to maintain neutral, breath-holding, pelvis sinking
Note: Only appropriate once basic core activation established (Stage 2+)
TEST 8: Valsalva Stress Test (Cough Test / Jump Test)
Purpose: Screen for pelvic floor dysfunction co-morbidity
Procedure:
- Ask patient to perform three strong coughs
- Ask: "Did you leak any urine?"
- Observe abdominal wall for doming on cough
Positive: Urine leakage (SUI present); significant doming (DRA + pelvic floor dysfunction)
TEST 9: Imaging-Based Diagnostic Tests
Ultrasound (Real-Time B-Mode) — GOLD STANDARD
- Most reliable clinical measurement tool
- Transducer placed transversely over midline at three levels
- Measures IRD in mm at:
- Rest
- ADIM (drawing-in maneuver)
- Curl-up
- Also qualitatively assesses linea alba thickness and echogenicity
- Advantages: Dynamic, real-time, no radiation, portable, inexpensive, widely available in physiotherapy practice
- IRD measurement: From medial border of right rectus sheath to medial border of left rectus sheath
| Position | Normal IRD | DRA Threshold |
|---|
| Rest, above umbilicus | < 15 mm | ≥ 20 mm |
| Rest, at umbilicus | < 22 mm | ≥ 22 mm |
| On ADIM | Decreases | No decrease (or worsens) = poor activation |
MRI
- Gold standard for surgical planning
- Best soft-tissue characterization of linea alba morphology, thickness, collagen integrity
- Assesses hernias, fascial defects, muscle atrophy
- Expensive; not routine in physiotherapy
CT Scan
- Used for surgical planning (abdominal wall reconstruction, hernia repair)
- Component Separation Index (CSI) calculated from CT
- Not first-line for physiotherapy assessment
Caliper Measurement
- Tissue-thickness calipers placed on medial borders of rectus muscles
- Less commonly used; moderate reliability
PART 6: PHYSIOTHERAPY ASSESSMENT — DETAILED FRAMEWORK
6.1 Subjective Assessment (Comprehensive History)
Patient Demographics & Background
- Age, sex, BMI
- Occupation (physical demands, prolonged sitting or standing)
- Activity level and sports participation
- Nutritional and hydration habits
Obstetric / Gynaecological History (for women)
- Number of pregnancies (gravida) and deliveries (para)
- Mode of delivery: vaginal vs. caesarean (number of CS, type of incision)
- Gestation at delivery
- Birth weight of neonates
- Instrumental delivery (forceps, ventouse)
- Immediate postpartum complications
- Time since delivery
- Breastfeeding status (prolactin suppresses estrogen; affects collagen quality)
- Menopausal status
Symptom History
- Primary complaint: What brought the patient in?
- Onset: Gradual or sudden? Linked to event (delivery, lifting)?
- Duration: Weeks, months, years
- Location: Where is the bulge/pain/weakness?
- Character of pain: Dull ache, sharp, burning, pressure
- Severity: NRS 0–10
- Aggravating factors: Lifting, coughing, sit-ups, prolonged standing, specific exercises
- Relieving factors: Rest, support garment, posture change
- 24-hour pattern: Worse morning / evening / end of day?
- Functional limitations: What can't you do? Getting out of bed, carrying children, running, exercise
Pelvic Floor Symptom Screening (MANDATORY)
- Urinary leakage: with cough/sneeze/jump (SUI) or urgency (UUI)?
- Frequency of voiding
- Nocturia
- Pelvic heaviness, dragging, or "something falling out" (prolapse symptoms)
- Bowel: constipation, straining, incomplete evacuation, fecal urgency/incontinence
- Sexual function: dyspareunia, reduced sensation
- Pelvic pain
Psychological / Quality of Life Screening
- Body image concerns
- Postpartum depression (Edinburgh Postnatal Depression Scale if appropriate)
- Anxiety related to returning to exercise
- Social participation restrictions
Previous Treatment
- Previous physiotherapy, what was done, outcomes
- Corsets, binders used
- Surgical history
- Medications (NSAIDs, relaxin supplements, collagen supplements)
Goals
- Patient's primary goals (return to running, weight training, pain relief, cosmesis)
- Timeline expectations
Red Flags — MUST EXCLUDE
| Red Flag | Concern |
|---|
| Palpable hard mass at gap | Incarcerated hernia |
| Sudden severe pain at bulge site | Strangulation |
| Nausea, vomiting, bowel obstruction signs | Hernia emergency |
| Neurological symptoms | Disc prolapse, nerve compression |
| Unexplained weight loss, night sweats | Malignancy |
| Fever, signs of infection | Post-surgical infection |
6.2 Objective Assessment
Postural Assessment (Standing, Full-Body)
Lateral view:
- Lumbar lordosis (increased = anterior pelvic tilt = increases abdominal wall loading)
- Thoracic kyphosis
- Head forward position
- Rib flare (lower ribs flared anteriorly = common in DRA; affects diaphragm position and TrA line of pull)
Anterior view:
- Pelvic obliquity
- Asymmetric muscle tone
- Abdominal ptosis (lower abdomen hang)
- Umbilical position/morphology
Posterior view:
- Pelvic level
- Shoulder height asymmetry
- Spinal curvature (scoliosis?)
Breathing Pattern Assessment
- Observed at rest: Chest-dominant vs. diaphragmatic?
- Lateral costal expansion: Adequate bilateral rib expansion?
- Abdominal wall movement: Rises anteriorly (normal) vs. sucks inward (dysfunctional)
- Pelvic floor response to breath: Descends on inhale, lifts on exhale (normal); reversed or absent (dysfunctional)
- Breath-holding tendency: Does patient hold breath for any trunk loading task?
Visual Inspection of Abdomen (Supine)
- Abdominal contour at rest
- Umbilical morphology
- Surgical scars (CS scar — assess for tethering, pain)
- Abdominal ptosis or asymmetry
- Ask patient to slowly perform a curl-up and observe for doming, coning
IRD Measurement (Ultrasound Preferred)
At three standardized levels:
- 4.5 cm above umbilicus
- At umbilicus
- 4.5 cm below umbilicus
Measured under three conditions:
- At rest (relaxed supine hook-lying)
- During ADIM (drawing-in maneuver)
- During partial curl-up
Recording format: Document exact IRD in mm at each level and each condition; compare at subsequent reviews
Linea Alba Tension Assessment
- Palpate gap with fingertips during head lift
- Record: taut / partially taut / flaccid / absent tension
- Determines conservative prognosis
Deep Core Activation Assessment
TrA Assessment:
- ADIM with palpation: Place fingers 2 cm medial to ASIS bilaterally; feel for gentle firm swelling (deep fascia tensioning) on drawing-in without global bracing
- Ultrasound: Measure TrA thickness at rest vs. during ADIM (should increase by ≥ 30%)
- Common faults: Global bracing (all muscles contract), breath-holding, posterior pelvic tilt instead of isolated TrA
Pelvic Floor Assessment:
- Verbal enquiry and symptom questionnaire
- Pelvic floor physiotherapist referral for internal assessment if indicated (PFDI-20, ICIQ)
Multifidus Assessment:
- Prone: Palpate 2 cm lateral to spinous processes L4/L5
- Ask for gentle heel lift — feel for multifidus contraction
- Ultrasound: Measure resting multifidus thickness (reduced thickness = atrophy)
Load Transfer Tests
- ASLR test (as described above)
- Hip hinge assessment: Can patient hinge with neutral spine and coordinated breathing?
- Single leg stance
- Step up/down: Observe trunk control and pelvic stability
Palpation
- Midline gap: width, depth, quality of tissue
- Linea alba texture: firm/fibrous vs. soft/empty
- CS scar (if applicable): mobility, tenderness, adherence
- Lumbar paraspinals: tenderness, hypertonicity
- Thoracolumbar fascia: tightness
- Iliopsoas, piriformis: tightness (common secondary findings)
Functional Movement Screen (Select Relevant Tests)
- Sit-to-stand: trunk control, breath management
- Squat: depth, knee tracking, trunk upright, IAP management
- Lunge: pelvic stability
- Overhead reach: rib flare, breathing pattern
- Carry: unilateral load management
Outcome Measures (Baseline and Progress Tracking)
| Outcome Measure | Domain Assessed |
|---|
| IRD (ultrasound, mm) | Structural |
| Linea alba tension (qualitative) | Functional structure |
| Numeric Pain Rating Scale (NPRS) | Pain |
| Patient-Specific Functional Scale (PSFS) | Patient-defined function |
| Oswestry Disability Index (ODI) | LBP disability |
| Active Straight Leg Raise (0–5) | Lumbopelvic load transfer |
| ICIQ-UI Short Form | Urinary incontinence |
| PFDI-20 | Pelvic floor dysfunction |
| PFIQ-7 | Pelvic floor quality of life |
| Edinburgh Postnatal Depression Scale | Psychological wellbeing (postnatal) |
| Global Rating of Change (GROC) | Overall perceived improvement |
PART 7: MANAGEMENT — COMPLETE PROTOCOL
7.1 Conservative Management (Physiotherapy-Led)
Guiding Principles
- Education first — the patient must understand their condition
- Linea alba tension restoration is the primary goal — not just gap closure
- Progressive loading — from deep activation to functional strength
- No doming rule — any exercise causing doming is stopped or modified
- IAP management — exhale on effort; never Valsalva
- Pelvic floor integration — always co-treat pelvic floor
- Individualize — severity, fitness, goals, postpartum stage all dictate pace
PHASE 1 — PROTECTION, EDUCATION & NEUROMUSCULAR ACTIVATION (Weeks 0–6)
Education Checklist
- ✅ Explain DRA mechanism in simple terms (show diagram)
- ✅ Why doming is harmful and how to recognize it
- ✅ Log-rolling technique: always roll to side before rising from lying (avoids sit-up motion)
- ✅ Posture correction: neutral pelvis, avoid anterior pelvic tilt and rib flare
- ✅ Avoid heavy lifting early on; if must lift, exhale while lifting
- ✅ Avoid: traditional crunches, sit-ups, double-leg raises, leg press with breath-holding
Abdominal Support
- Tubigrip / abdominal binder: Provides gentle midline compression, reduces discomfort, improves proprioception
- Worn during active tasks, not 24/7
- Avoid over-reliance — can inhibit intrinsic core training
- Consider in early postpartum (weeks 0–6), after CS, or severe DRA
- Kinesio taping (KT Tape): Strips applied horizontally across midline with 25% tension
- May reduce pain and provide tactile feedback for posture
- Evidence limited but low-risk adjunct
- Compression shorts / high-waisted leggings: Comfortable option for daily wear
CS Scar Management (if applicable)
- From 6–8 weeks postpartum (once healed): scar desensitization, mobilization
- Prevents scar tethering which restricts fascial mobility and abdominal mechanics
PHASE 2 — DEEP CORE RE-EDUCATION (Weeks 4–12)
Goal: Restore isolated TrA, pelvic floor, diaphragm, and multifidus activation. Restore their coordination.
Exercise 1: Diaphragmatic Breathing with Pelvic Floor Coordination
Purpose: Foundation of all further rehab; restores pressure regulation system
Technique:
- Supine, knees bent, hands on lower ribs
- Inhale: Ribs expand laterally and anteriorly; lower abdomen rises gently; pelvic floor descends naturally (do not force)
- Exhale: Ribs drop; lower abdomen draws gently inward; pelvic floor lifts naturally
- Key: pelvic floor and TrA response is passive and automatic with correct breathing
- 10 breath cycles, 3× daily
- Progress: seated, standing, then during movement
Exercise 2: Abdominal Drawing-In Maneuver (ADIM)
Purpose: Isolated TrA activation without global bracing
Technique:
- Supine hook-lying
- Gently draw lower abdomen inward and upward (navel toward spine)
- Do NOT: flatten the entire lumbar spine, hold the breath, or activate all abdominals together
- Feel for gentle tensioning of lower abdominal wall (not a hard brace)
- Hold: 8–10 seconds; Repetitions: 10; Sets: 3–4; Frequency: 2–3×/day
Progressions:
- Hook-lying → 4-point kneeling → sitting → standing
- Add limb movement (heel slides) while maintaining activation
Exercise 3: Pelvic Floor Contractions (Kegels)
Purpose: Restore pelvic floor neuromuscular control and coordination with TrA
Technique (slow-twitch, Type I fiber training):
- Identify pelvic floor: imagine stopping flow of urine AND stopping passing wind simultaneously
- Contract upward and inward (elevator going up)
- Hold: 8–10 seconds; Relax fully 4–8 seconds between
- Repetitions: 8–12; Sets: 3; Frequency: 3×/day
Technique (fast-twitch, Type II fiber training):
- Quick flick contractions
- 10 quick contractions; Sets: 3; Frequency: 3×/day
Coordination with breathing:
- Exhale + pelvic floor lift + TrA gentle activation — the three happen simultaneously
- Teaches proper IAP management for all activities
Exercise 4: 4-Point Kneeling Multifidus / Arm Lift
Purpose: Activate multifidus and co-activate TrA in quadruped
Technique:
- 4-point kneeling (wrists under shoulders, knees under hips)
- Neutral spine (not arched or flattened)
- Activate ADIM; lift one arm to shoulder height only
- Maintain spine position; do not rotate
- Hold: 5–8 seconds; 8–10 reps per side; 2–3 sets
PHASE 3 — FUNCTIONAL CORE LOADING (Weeks 8–16)
Goal: Load the deep core system progressively through increasingly challenging positions and movements. No doming at any point.
Clinical physiotherapy protocol for DRA rehabilitation: (A) Abdominal breathing with pelvic floor engagement using foam block; (B) Rotational oblique activation with therapist resistance; (C) Prone leg extension over abdominal pillow for TrA/multifidus co-activation; (D) Side-lying lateral core stability training.
Exercise 5: Dead Bug
Purpose: TrA endurance with contralateral limb loading; classic DRA-safe core exercise
Setup: Supine, arms pointing to ceiling, hips and knees both at 90° (tabletop)
Technique:
- Activate TrA (ADIM) and pelvic floor
- Exhale: slowly lower right arm overhead toward floor + simultaneously extend left leg toward floor (heel 5 cm above floor)
- Inhale: return to start
- Alternate sides
- Key: lumbar spine must NOT lift off floor; NO doming; NO breath-holding
- Progression: add resistance band on arms or ankle weight on leg
Dosage: 8–10 reps per side; 3 sets
Exercise 6: Bird-Dog
Purpose: Anti-extension and anti-rotation core stability in quadruped
Setup: 4-point kneeling, neutral spine
Technique:
- Activate TrA; exhale and extend right arm to shoulder height + left leg to hip height simultaneously
- Do not rotate hips; maintain completely level pelvis
- Hold 5–8 seconds; return slowly
- Alternate sides
Progression:
- Arm only → Leg only → Combined
- Add theraband resistance on arm
- Add ankle weight
- Perform on unstable surface (BOSU)
Dosage: 10 reps per side; 3 sets
Exercise 7: Glute Bridge
Purpose: Posterior chain activation, lumbopelvic stability, moderate core loading
Setup: Supine hook-lying, feet hip-width apart
Technique:
- Activate TrA + pelvic floor; exhale and push through heels
- Lift hips until shoulder-hip-knee alignment achieved
- Hold 2–3 seconds; lower slowly while maintaining TrA
- Do NOT hyperextend lumbar spine at top
- Progress: march in bridge (alternate leg lifts), single-leg bridge, bridge with resistance band around knees
Dosage: 3 × 15 reps
Exercise 8: Heel Slides
Purpose: TrA endurance while maintaining neutral spine under increasing limb load
Setup: Supine hook-lying, TrA activated
Technique:
- Exhale; slide one heel slowly along the floor until leg fully extended (heel hovers 2 cm above floor)
- Inhale; slowly return
- Maintain lumbar neutral throughout
- Progress to bilateral alternating, then double leg slides
Dosage: 10 reps per side; 3 sets
Exercise 9: Side-Lying Hip Abduction / Clamshell
Purpose: Hip external rotator and abductor strengthening; reduces compensatory lumbopelvic movement
Setup: Side-lying, hips and knees at 45°, pelvis stacked
Clamshell Technique:
- Maintain stacked pelvis; open top knee upward like a clamshell
- Do NOT allow pelvis to roll backward
- Resistance band around knees to increase load
Hip Abduction Technique:
- Straight top leg lifts to 30°; hold 2 seconds; lower
- Resistance band around ankles
Dosage: 3 × 15 reps per side
Exercise 10: Modified Kneeling Plank
Purpose: Anti-extension isometric core stability
Setup: Forearms on floor, knees on floor (short lever)
Technique:
- Maintain neutral spine (no sagging hips, no elevated hips)
- Activate TrA; breathe normally throughout (no breath-holding)
- Watch for: doming, hips sagging, lumbar overextension
- Progress to: full plank on toes (only if no doming observed)
Dosage: 3 × 20–30 seconds; progress to 60 seconds
Exercise 11: Pallof Press (Anti-Rotation Press)
Purpose: Challenges rotational stability without loading the linea alba in a harmful direction
Setup: Stand side-on to cable machine or resistance band anchor at chest height
Technique:
- Hold band/cable at chest; activate TrA
- Exhale: press arms straight forward; hold 3 seconds; maintain square pelvis and shoulders
- Inhale: return to chest
- The band pulls you rotationally — resist that rotation
Dosage: 10–12 reps per side; 3 sets
PHASE 4 — ADVANCED LOADING & RETURN TO SPORT (Weeks 16+)
Goal: Full functional strength and return to all activities including high-load exercise, running, jumping, sport
Clearance Criteria Before Phase 4
- IRD within acceptable range (or stable with good tension)
- No doming with plank, bird-dog, dead bug
- ASLR test improved / resolved
- Pelvic floor: no SUI with running or jumping
- Good breathing mechanics under moderate load
Advanced Exercises
Full Plank: Standard forearm or straight-arm plank (only if no doming)
Loaded Carries:
- Bilateral farmer's carry (dumbbells at sides)
- Suitcase carry (unilateral — increases anti-lateral flexion demand)
- Overhead carry
- Progress weight weekly
Hip Hinge Progression:
- Romanian deadlift → Barbell deadlift
- Teach: inhale + brace on descent; exhale on ascent
- Correct bracing (360° abdominal brace, not just drawing-in) appropriate in this phase for heavy loads
Squat Progression:
- Goblet squat → Front squat → Back squat
- Monitor for rib flare and lumbar overextension
Lunge Variations: Forward, reverse, lateral, walking lunges
Overhead Press: Seated → Standing; monitor rib flare and lumbar hyperextension
Return to Running Protocol:
- Only after: no pelvic floor leakage, adequate hip strength, single-leg stability
- Walk-run intervals progressively increasing run time
Plyometrics (Jumping):
- Assess for pelvic floor leakage first
- Begin with double-leg low hops → progress to HIIT, box jumps, sport-specific
7.2 Surgical Management
Indications for Surgical Referral
- IRD persistently > 3–4 cm with significant dysfunction after 6+ months of consistent physiotherapy
- Associated umbilical or epigastric hernia
- Absent linea alba tension non-responsive to conservative treatment
- Severe functional limitation (cannot perform ADLs)
- Patient preference for cosmetic correction with functional failure
- Severe abdominal ptosis not correctable conservatively
Surgical Procedures (Detailed)
| Procedure | Technique | Indication | Notes |
|---|
| Open midline plication | Suture repair of rectus sheaths in the midline under direct vision; no skin excision | Functional DRA without excess skin | Pitanguy or Callia technique; good durable result |
| Abdominoplasty ("tummy tuck") | Full plication of linea alba + excision of excess skin + umbilicoplasty | DRA + abdominal skin laxity + ptosis | Most common after massive weight loss or multi-parity |
| Mini-abdominoplasty | Partial plication (infra-umbilical) + limited skin excision | Isolated infra-umbilical DRA + minimal skin excess | Less scarring than full abdominoplasty |
| Endoscopic plication | Minimally invasive; laparoscope-assisted plication of linea alba | Supra-umbilical DRA without hernia | Less scarring, faster recovery; technically demanding |
| Laparoscopic/robotic repair | Combined hernia repair + myofascial component separation | DRA + large hernia + prior repairs | Complex abdominal wall reconstruction |
| Bariatric + body contouring | Post-weight loss abdominoplasty with plication | Obesity-related DRA after weight loss surgery | Often combined with lower body lift |
Post-Surgical Physiotherapy
Physiotherapy is essential after all surgical approaches:
- Weeks 0–4: Education, breathing, log-roll technique, gentle TrA activation, walking
- Weeks 4–8: Progressive ADIM, pelvic floor, scar mobilization (from 6 weeks)
- Weeks 8–16: Functional core loading (Phase 2–3 program)
- Weeks 16+: Return to sport protocol
PART 8: ROLE OF CORE EXERCISES IN DRA — IN DEPTH
8.1 Why Core Exercise is the Foundation of DRA Treatment
The anterior abdominal wall is a dynamic, active structure — not just a passive container. Its ability to transmit forces, regulate IAP, and stabilize the spine depends entirely on the coordinated activation of all muscular components. When DRA disrupts the linea alba, this coordination breaks down.
Core exercise rehabilitation works through the following mechanisms:
Mechanism 1: TrA Activation Narrows IRD
Multiple ultrasound studies demonstrate that ADIM reduces IRD by increasing linea alba tension through lateral pull of the TrA aponeurosis. While this effect is temporary (only during activation), repeated training leads to:
- Improved neuromuscular recruitment patterns
- Increased resting TrA tone over time
- Better anticipatory pre-activation before loading tasks
Mechanism 2: Restoration of Linea Alba Tension
The ultimate goal is not just narrowing the gap but restoring stiffness to the linea alba tissue. Controlled progressive loading stimulates:
- Collagen fiber remodeling (mechanotransduction)
- Improved cross-linking
- Restoration of the three-dimensional collagen weave architecture
Wolff's Law applied to soft tissue: controlled mechanical loading stimulates remodeling and strengthening of connective tissue.
Mechanism 3: Lumbopelvic Stability Restoration
As TrA, pelvic floor, multifidus, and diaphragm coordination returns:
- Pre-activation before limb movements is restored
- Passive structures (lumbar discs, ligaments) are protected from excessive load
- LBP and PGP resolve
- Functional tasks become less painful and easier
Mechanism 4: IAP Regulation
The "pressure canister" system (diaphragm above, pelvic floor below, TrA circumferentially, multifidus posteriorly) regulates IAP. Rehabilitation restores this coordinated system, preventing:
- Excessive spikes with coughing, lifting, exercise
- Pelvic floor overload
- Doming with effort
8.2 Core Exercise Safety Principles in DRA
These principles govern every exercise decision in DRA rehabilitation:
Principle 1: The No-Doming Rule
Any exercise that produces doming/coning of the midline is inappropriate at that stage.
Doming means:
- IAP exceeds linea alba resistance
- Abdominal contents herniate forward through the gap
- The linea alba is loaded beyond its capacity
- Progressive tissue damage may occur
Response to doming: modify or stop the exercise; regress to an easier progression.
Principle 2: Exhale on Effort
Every time effort/exertion occurs (lifting, pressing, rising), the patient exhales. This:
- Prevents Valsalva maneuver
- Coordinates pelvic floor contraction with abdominal effort
- Reduces IAP spike
- Protects linea alba
Principle 3: Tension Over Width
Exercises should aim to generate linea alba tension — feeling the midline tighten during activation is the goal. Gap width reduction alone is insufficient.
Principle 4: Progressive Overload
The linea alba (like all connective tissue) requires progressive mechanical loading to remodel. Start minimal → systematically increase:
- Lever arm length (bent knee → straight leg)
- External resistance (no weight → dumbbells → barbell)
- Instability (stable → unstable surface)
- Speed (slow → functional speed)
Principle 5: Pelvic Floor Co-Treatment
Pelvic floor and abdominal wall work as a unit. Neglecting pelvic floor rehabilitation:
- Leaves IAP dysregulation unresolved
- Fails to address SUI/prolapse
- Undermines abdominal wall rehabilitation
8.3 Exercises to AVOID in DRA (and Why)
| Exercise | Why to Avoid |
|---|
| Full sit-ups / crunches | Creates maximum IAP spike; produces doming; loads linea alba beyond tolerance |
| Double leg raises (straight legs) | Massive IAP increase; severe doming; linea alba cannot resist |
| Oblique crunches / Russian twists | Rotational shear force on weakened linea alba |
| Heavy barbell back squat (early) | Valsalva maneuver; excessive IAP |
| Heavy deadlift (early) | Same as above |
| Leg press machine (heavy) | Forced hip flexion compresses abdomen; high IAP |
| Plank (full, early stage) | Load may exceed linea alba resistance; causes doming |
| Boat pose (yoga) | Similar to double leg raise — high doming risk |
| Advanced Pilates V-sit | Extreme hip flexion + spinal flexion = high IAP |
| High-intensity interval training (early) | Running + jumping → pelvic floor + core overload |
Rule: Return to these exercises is possible — but only after establishing adequate linea alba tension and confirmed absence of doming.
8.4 Complete Evidence-Based Core Exercise Program
STAGE 1: Weeks 1–6
| # | Exercise | Sets × Reps | Key Cue |
|---|
| 1 | Diaphragmatic breathing + PF coordination | 3 × 10 breaths | Ribs expand laterally; PF lifts on exhale |
| 2 | ADIM (supine) | 3 × 10 × 10 sec hold | Gentle navel to spine; do not flatten spine |
| 3 | Kegels (slow + fast) | 3 × 10 each | Full relaxation between reps |
| 4 | Posterior pelvic tilt | 3 × 10 × 5 sec | Lower back gently flattens |
| 5 | 4-point kneeling arm lift | 2 × 8/side | Neutral spine; exhale on arm lift |
| 6 | ADIM in standing | 3 × 10 | Transfers to functional posture |
STAGE 2: Weeks 4–12
| # | Exercise | Sets × Reps | Key Cue |
|---|
| 1 | Dead bug (modified) | 3 × 8/side | Lumbar stays down; exhale on limb extension |
| 2 | Bird-dog | 3 × 10/side | Level pelvis; 5-second hold |
| 3 | Glute bridge | 3 × 15 | Exhale on lift; no lumbar hyperextension |
| 4 | Heel slides | 3 × 10/side | TrA activated; neutral lumbar |
| 5 | Clamshell (resistance band) | 3 × 15/side | Pelvis stacked; no pelvic roll |
| 6 | Side-lying hip abduction | 3 × 15/side | Controlled; slow eccentric |
| 7 | Wall sit | 3 × 30 sec | Breathing maintained; TrA active |
STAGE 3: Weeks 8–16
| # | Exercise | Sets × Reps | Key Cue |
|---|
| 1 | Modified plank (kneeling) | 3 × 30 sec | No doming; breathe throughout |
| 2 | Pallof press | 3 × 10/side | Square hips and shoulders; exhale on press |
| 3 | Single-leg bridge | 3 × 12/side | Pelvis level; exhale on lift |
| 4 | Romanian deadlift (light) | 3 × 12 | Hip hinge; neutral spine; exhale on ascent |
| 5 | Goblet squat | 3 × 12 | Upright torso; breathing controlled |
| 6 | Step-up with knee drive | 3 × 12/side | Core stable; exhale on step |
| 7 | TRX / ring row | 3 × 12 | Lat pull; posterior chain |
| 8 | Side plank (modified — knee down) | 3 × 20 sec | Lateral chain; no hip sag |
STAGE 4: Weeks 16+
| # | Exercise | Sets × Reps | Key Cue |
|---|
| 1 | Full plank | 3 × 45–60 sec | Confirm no doming before progressing |
| 2 | Farmer's carry (bilateral / suitcase) | 3 × 30 m | Tall posture; breathe rhythmically |
| 3 | Barbell Romanian deadlift | 4 × 8 | Progressive load; exhale on lift |
| 4 | Barbell back squat | 4 × 8 | Only with confirmed core competency |
| 5 | Overhead press | 3 × 10 | Ribs down; no lumbar hyperextension |
| 6 | Cable/band pull-through | 3 × 12 | Hip hinge pattern; core stable |
| 7 | Bulgarian split squat | 3 × 10/side | Pelvic stability; loaded |
| 8 | Plyometric progression | Progressive | Only after pelvic floor clearance |
8.5 Scientific Evidence Summary
| Study | Finding |
|---|
| Mota et al. (2015) | Both ADIM and curl-up reduce IRD on ultrasound; ADIM produces less doming |
| Lee & Hodges (2016) | Linea alba tension is more functionally important than IRD width alone |
| Thabet & Alshehri (2019) | RCT: core stabilization exercises significantly reduced IRD and improved functional outcomes vs. control group |
| Bø & Hilde (2013) | Systematic review: specific exercise reduces IRD but complete closure not always achievable |
| Benjamin et al. (2019) | Ultra-sound confirmed IRD reduction with progressive core training programs |
| Groom et al. (2019) | Return to exercise guidance post-partum: staged loading essential; avoid high-load early |
| Beamish et al. (2019) | Women with DRA have significantly worse lumbopelvic symptoms; physiotherapy improves outcomes |
PART 9: SPECIAL POPULATIONS
9.1 Postpartum DRA (Most Common Presentation)
Postpartum Staging
| Stage | Timeline | Priorities |
|---|
| Immediate | 0–2 weeks | Rest, education, log-roll, breathing, pelvic floor (gentle) |
| Early postpartum | 2–6 weeks | ADIM, pelvic floor, posture, scar care (CS) |
| Late postpartum | 6–12 weeks | Phase 2 core loading begins; GP clearance at 6 weeks |
| Beyond | 12+ weeks | Progressive functional loading; return to exercise |
Breastfeeding considerations: Prolactin suppresses estrogen → continued ligament and connective tissue laxity → go slower with loading progressions.
9.2 Male DRA
- Typically presents as upper abdominal bulge in overweight, middle-aged men (Bailey & Love, p.1079)
- Mechanism: chronic IAP elevation from obesity + poor abdominal wall tone
- Often associated with umbilical or epigastric hernia
- Management same principles; weight loss is an additional priority
- Higher surgical intervention rate (less hormonal resolution, often larger gap)
9.3 Neonatal / Infant DRA
- Normal variant at birth — rectus muscles have not yet fused
- Resolves spontaneously in > 95% of cases by 12 months
- No treatment required unless persists beyond 2 years
- Reassure parents
9.4 DRA with Connective Tissue Disorder (Ehlers-Danlos, Marfan)
- More severe, recurrent, and refractory DRA
- Conservative management aims to maximize muscle support of weakened fascia
- Surgical repair results less durable — inform patient
- Multidisciplinary management with rheumatology
PART 10: PROGNOSIS & OUTCOMES
| Factor | Favorable Prognosis | Unfavorable Prognosis |
|---|
| Linea alba tension on activation | Present | Absent |
| IRD | < 3 cm | > 5 cm |
| Duration | Recent (< 6 months) | Chronic (> 2 years) |
| Parity | Primipara | Grand multipara (≥ 5) |
| BMI | Normal | Obese |
| Compliance | High | Poor |
| Associated hernia | Absent | Present |
| Connective tissue disorder | Absent | Present |
Key statistic: Without treatment, ~39% of women still have clinically significant DRA at 6 months postpartum (Mota et al., 2015). With targeted physiotherapy, outcomes improve significantly — most women achieve functional recovery within 4–6 months of consistent rehabilitation.
SUMMARY REFERENCE TABLE
| Domain | Key Points |
|---|
| Anatomy | Linea alba = decussating aponeuroses of EO, IO, TrA; active force-transmitting structure |
| Definition | IRD ≥ 2 cm + reduced linea alba tension = DRA |
| Causes | Pregnancy (primary), obesity, CTD, chronic IAP, multiparity, surgical history |
| Clinical features | Midline bulge/doming, LBP, PGP, pelvic floor dysfunction, abdominal weakness, bloating |
| Special tests | Finger-width test, ultrasound (gold standard), tension test, ASLR, single-leg stance |
| Physio assessment | IRD measurement, tension, posture, breathing, deep core activation, load transfer, pelvic floor, functional movement |
| Phase 1 management | Education, log-roll, support garment, breathing, ADIM, Kegels |
| Phase 2 | Dead bug, bird-dog, bridges, heel slides |
| Phase 3 | Plank, Pallof press, deadlift pattern, squat pattern |
| Phase 4 | Heavy compound lifts, carries, plyometrics, return to sport |
| Core exercise role | Restores TrA tension, linea alba stiffness via mechanotransduction, IAP regulation, lumbopelvic stability |
| Avoid | Sit-ups, double leg raises, Russian twists, early heavy loading, Valsalva |
| Surgery | When conservative fails > 6 months, hernia present, IRD > 4 cm with absent tension |
| Prognosis | Good with early intervention, linea alba tension present, adequate compliance |