Coronory anastomosis of retinal vasculature
Reading File
search_medical_text
retinal vascular anastomosis collateral circulation
search_medical_image
retinal vasculature anastomosis fundus
GradeResponse
GradeResponse
The retrieved results are not specific to the topic. Drawing on established ophthalmology knowledge to provide a comprehensive answer:
Coronary Anastomoses of the Retinal Vasculature
Note on terminology: The term "coronary anastomosis" in the context of the retina refers to the circular (peripapillary/circumpapillary) anastomotic ring — the corona-like network of interconnections around the optic disc — not to cardiac coronary vessels.
Anatomy of the Retinal Vascular Supply
The retina is supplied by two independent systems:
| System | Source | Territory |
|---|---|---|
| Central retinal artery (CRA) | Ophthalmic artery (from internal carotid) | Inner retinal layers |
| Choroidal circulation | Short posterior ciliary arteries | Outer retinal layers (photoreceptors, RPE) |
The central retinal artery enters the eye through the optic nerve and divides at the disc into superior and inferior arcades, each further bifurcating into nasal and temporal branches. These are end arteries — they do not form true anastomoses within the retinal parenchyma under normal conditions.
The Circumpapillary (Coronary) Anastomotic Ring
Circle of Zinn-Haller
The most clinically important anastomotic ring in the posterior segment is the Circle of Zinn-Haller (also called the arterial circle of Zinn and Haller or intrascleral arterial circle):
- Formed by anastomoses of the short posterior ciliary arteries (SPCAs) within the sclera around the optic nerve head
- Provides collateral supply to the prelaminar and laminar portions of the optic nerve head
- Gives rise to recurrent choroidal arteries and centripetal branches to the CRA territory
- Acts as a bypass route when the CRA is compromised
Clinical Significance of Zinn-Haller Circle
- Its completeness (complete ring vs. incomplete arc) varies between individuals and determines susceptibility to anterior ischemic optic neuropathy (AION)
- Eyes with a small or absent circle or a "disc at risk" (small cup-to-disc ratio) are predisposed to NAION
- Can provide collateral rescue blood flow in central retinal artery occlusion (CRAO)
Optociliary Shunt Vessels (Retinociliary / Ciliochoroidal Anastomoses)
These are preformed channels between the retinal and choroidal circulations at the optic disc margin. They are normally not visible but dilate and become visible (as optociliary shunt vessels) when there is chronic obstruction of venous outflow (e.g., CRVO, optic nerve sheath meningioma, Behçet's disease).
Features:
- Located at the optic disc margin
- Represent venus-to-venous collaterals draining retinal blood into the choroidal venous system
- Distinguished from true neovascularization: they do not leak on fluorescein angiography
- Classic triad of chronic CRVO + optociliary shunts + optic atrophy is associated with central retinal vein occlusion and optic nerve sheath meningioma
Retino-Retinal Collaterals in Branch Retinal Vein Occlusion (BRVO)
After BRVO, collateral vessels can develop across the horizontal raphe:
- They bypass the occlusion site, draining affected quadrant blood into unaffected veins
- Appear as tortuous, corkscrew vessels on fundus examination
- Take months to develop; reduce macular edema when well-established
- Do not leak on FA (unlike neovascularization)
Cilioretinal Arteries — A Natural Anastomotic Variant
Cilioretinal arteries arise from the ciliary circulation (not the CRA) and supply part of the papillomacular bundle in ~15–30% of the population. They emerge at the disc margin, typically on the temporal side.
Protective role:
- When CRAO occurs, patients with a cilioretinal artery may preserve central vision if the macula is within the cilioretinal territory
- Conversely, isolated cilioretinal artery occlusion can paradoxically cause central scotoma in an eye with an otherwise intact CRA
Coronary Anastomoses in Diabetic Retinopathy (Intraretinal Microvascular Abnormalities — IRMA)
IRMA represents dilated, tortuous intraretinal collateral channels forming within zones of capillary non-perfusion:
- Act as arterio-venous shunts bypassing occluded capillary beds
- Signify severe non-proliferative diabetic retinopathy (NPDR) — part of the 4-2-1 rule for high-risk NPDR
- Distinguished from neovascularization elsewhere (NVE): IRMA lies within the retina and does not extend onto the vitreous face; does not leak profusely on FA
Summary Table: Key Retinal Anastomotic Structures
| Structure | Type | Clinical Relevance |
|---|---|---|
| Circle of Zinn-Haller | Arterial (ciliary-ciliary) | NAION susceptibility; CRA occlusion collateral |
| Optociliary shunt vessels | Venous (retinociliary) | Chronic CRVO, optic nerve meningioma |
| Cilioretinal artery | Arterial (ciliary-retinal) | Vision preservation in CRAO |
| BRVO collaterals | Venous (retino-retinal) | Recovery after branch vein occlusion |
| IRMA | Arteriovenous (retinal) | Severe NPDR progression marker |
The retinal vasculature, while largely an end-artery system, possesses several anatomical and pathological anastomotic networks — particularly at the optic disc — that are of major diagnostic and prognostic significance in conditions ranging from vascular occlusions to optic nerve disease.
Carotid sinus reflex
search_medical_text
carotid sinus reflex anatomy physiology baroreceptor
search_medical_text
carotid sinus hypersensitivity syndrome clinical management
GradeResponse
GradeResponse
search_medical_text
carotid sinus syncope vasodepressor cardioinhibitory types pacemaker
search_medical_image
carotid sinus baroreceptor reflex arc diagram
GradeResponse
Carotid Sinus Reflex
Anatomy of the Carotid Sinus
The carotid sinus is a slight dilatation at the bifurcation of the common carotid artery into the internal and external carotid arteries. Its wall contains a dense network of mechanoreceptors (baroreceptors) — stretch-sensitive nerve endings within the adventitia — supplied by the carotid sinus nerve (nerve of Hering), a branch of the glossopharyngeal nerve (CN IX).
Reflex Arc
Afferent Limb
- Baroreceptors in the carotid sinus wall detect wall tension (a surrogate for arterial pressure)
- Signals travel via the carotid sinus nerve → glossopharyngeal nerve (CN IX) to the nucleus tractus solitarius (NTS) in the dorsomedial medulla
- Aortic arch baroreceptors contribute via the vagus nerve (CN X) to the same NTS
Central Processing (Harrison's, p. 698)
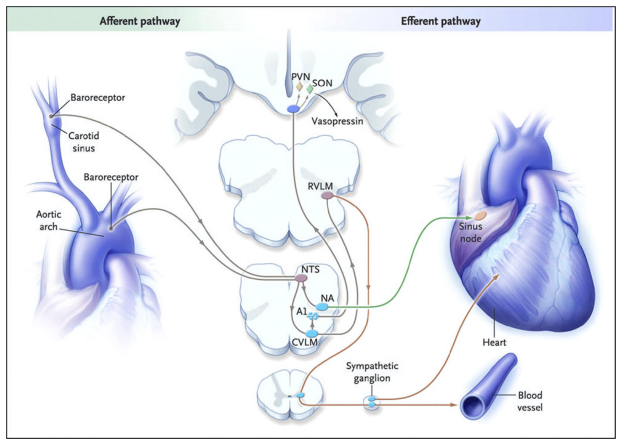
| Central Node | Role |
|---|---|
| NTS | Primary integration center; receives all baroreceptor afferents |
| Nucleus Ambiguus (NA) | Parasympathetic (vagal) output to the SA node |
| CVLM | Inhibits RVLM (excitatory interneuron) |
| RVLM | Drives sympathetic preganglionic neurons; suppressed by high BP |
| PVN / SON (hypothalamus) | Modulate vasopressin release |
Efferent Limb
↑ Blood pressure → ↑ baroreceptor firing →
- ↑ Vagal tone to SA node → bradycardia
- ↓ Sympathetic output → vasodilation + ↓ cardiac contractility
- Net effect: ↓ BP (buffering response)
↓ Blood pressure → ↓ baroreceptor firing →
- ↓ Vagal tone → tachycardia
- ↑ Sympathetic output → vasoconstriction + ↑ cardiac output
- Net effect: ↑ BP restoration
Physiological Role
- Acts as a short-term, beat-to-beat blood pressure buffer (not a long-term BP regulator)
- Responds within seconds; resets to the prevailing mean BP over hours (explains why it cannot correct chronic hypertension)
- Particularly sensitive to dynamic (pulsatile) pressure changes rather than static mean pressure
Carotid Sinus Hypersensitivity (CSH)
An exaggerated response to carotid sinus stimulation, defined as:
- Cardioinhibitory type: Asystole ≥ 3 seconds induced by carotid sinus massage (CSM)
- Vasodepressor type: Systolic BP drop ≥ 50 mmHg without significant bradycardia
- Mixed type: Both components present (most common in clinical practice)
Triggers of CSH (Carotid Sinus Syncope)
- Tight collar or necktie
- Head turning
- Shaving over the neck
- Neck tumors or lymphadenopathy compressing the sinus
- Post-carotid endarterectomy hypersensitivity
Epidemiology
- Predominantly affects older males (> 60 years)
- Associated with coronary artery disease, hypertension, and atherosclerosis
Carotid Sinus Massage (CSM) — Diagnostic Test
Per ACC/AHA Evaluation and Management of Bradycardia and Cardiac Conduction Delay guidelines (p. 11):
Technique:
- Auscultate both carotids — exclude significant carotid bruit (carotid Doppler/ultrasound if uncertain); mandatory before proceeding as strokes have been reported
- Apply firm longitudinal pressure over the carotid sinus (below the angle of the jaw) for 5–10 seconds
- Perform in both supine and upright (tilt) positions — upright position increases diagnostic yield
- Continuous ECG and blood pressure monitoring required
Contraindications:
- Recent stroke or TIA (< 3 months)
- Significant ipsilateral carotid stenosis
- History of carotid endarterectomy (relative)
- Recent MI (relative)
Management of Carotid Sinus Syncope
| Type | Management |
|---|---|
| Cardioinhibitory | Dual-chamber pacemaker (Class IIa indication in recurrent syncope with cardioinhibitory CSH) |
| Vasodepressor | Avoid precipitating factors; compression stockings; fludrocortisone or midodrine (limited evidence) |
| Mixed | Pacemaker + vasopressor agents; lifestyle modification |
Lifestyle measures applicable to all types:
- Avoid tight collars, sudden head turns
- Rise slowly from supine
- Maintain adequate hydration
Clinical Pearls
- The carotid sinus reflex is the fastest-acting cardiovascular reflex in the body
- It is vagally dominant — the bradycardic response is typically more pronounced than vasodilation
- Atropine abolishes the cardioinhibitory component; does not fully reverse the vasodepressor component
- In denervation (post-carotid surgery, radiation), patients may develop baroreceptor failure syndrome — labile hypertension, tachycardia, and orthostatic hypotension
- The glossopharyngeal nerve is also responsible for the gag reflex and swallowing syncope — distinct but anatomically related reflexes
This is a shared conversation. Sign in to Orris to start your own chat.