Hi
What is headache? explain type and cure in detaisl
Search the medical database for: "headache definition classification types primary secondary". Return all relevant content including causes, subtypes, and distinguishing features.
Search the medical database for: "headache treatment management pharmacological non-pharmacological cure". Return all relevant content including medications, lifestyle changes, and therapies.
headache definition classification types primary secondary
Management of Headache
Page 6
primary headache causes subtypes migraine tension cluster
Management of Headache
Page 7
headache classification types primary secondary diagram
Hugging Face pmc clinical VQA raw
Page 0
headache treatment management pharmacological
Acute Treatment of Migraine in Children and Adolescents
Page 2
headache non-pharmacological therapy lifestyle changes
Management of Headache
Page 115
secondary headache causes distinguishing features red flags
Management of Headache
Page 30
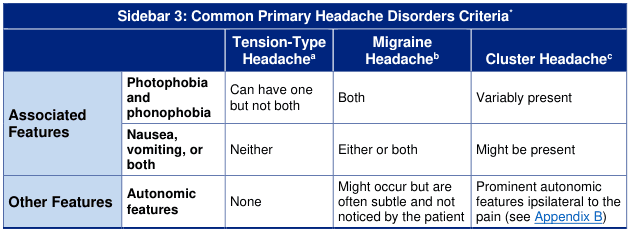
tension-type headache migraine cluster headache distinguishing features criteria ICHD-3
migraine tension cluster headache features comparison
Management of Headache
Page 31
migraine acute medications triptans NSAIDs analgesics
Integrating New Migraine Treatments Into Clinical Practice
Page 13
headache preventive treatment medications prophylaxis
migraine pharmacological treatment algorithm
Hugging Face pmc clinical VQA raw
Page 0
Headache: Definition, Types & Treatment
What is a Headache?
- Primary Headaches - Idiopathic, recurrent, and stereotyped, with no identifiable underlying disease causing them.
- Secondary Headaches - Caused by another identifiable condition or disorder.
Part 1: Types of Headaches
🔵 Primary Headaches
1. Tension-Type Headache (TTH)
| Feature | Description |
|---|---|
| Pain quality | Pressing or tightening (non-pulsating), like a band around the head |
| Location | Bilateral (both sides) |
| Severity | Mild to moderate |
| Duration | 30 minutes to 7 days |
| Nausea/Vomiting | Neither |
| Photophobia/Phonophobia | Can have one but NOT both |
| Autonomic features | None |
| Worsening with activity | Does not worsen |
2. Migraine Headache
| Feature | Description |
|---|---|
| Pain quality | Pulsating/throbbing |
| Location | Usually unilateral (one side) |
| Severity | Moderate to severe |
| Duration | 4–72 hours |
| Nausea/Vomiting | Either or both (hallmark feature) |
| Photophobia/Phonophobia | Both present |
| Autonomic features | May occur but often subtle |
| Worsening with activity | Yes - worsened by routine activity |
3. Cluster Headache
| Feature | Description |
|---|---|
| Pain quality | Sharp, stabbing, burning |
| Location | Strictly unilateral, around/behind one eye |
| Severity | Excruciating (9–10/10) |
| Duration | 15–180 minutes per attack |
| Pattern | Occur in "clusters" - daily attacks for weeks/months, then remission |
| Nausea/Vomiting | May be present |
| Photophobia/Phonophobia | Variably present |
| Autonomic features | Prominent - tearing, red eye, nasal congestion, drooping eyelid (ptosis), all on the same side as pain |

🔴 Secondary Headaches
- The headache is new AND develops in temporal relation to a known causative disorder, OR
- A pre-existing headache significantly worsens in temporal relation to the causative disorder.
| Category | Examples |
|---|---|
| Trauma/Injury | Post-concussion headache, whiplash |
| Vascular | Stroke, subarachnoid hemorrhage, hypertensive crisis |
| Intracranial | Brain tumor, hydrocephalus, meningitis |
| Infection | Meningitis, encephalitis, sinusitis, COVID-19 |
| Substance/Withdrawal | Medication overuse headache (MOH), alcohol, caffeine withdrawal |
| Homeostasis disorder | High altitude, hypoxia, fasting, hypothyroidism |
| Structural | Cervicogenic (neck-related), dental problems, glaucoma |
| Psychiatric | Depression, anxiety, somatization |
⚠️ Red Flags ("SNOOP4"): Sudden severe onset ("thunderclap"), headache with fever/stiff neck, new headache after age 50, headache with neurological symptoms, headache after trauma, or headache that is rapidly worsening - these require urgent medical evaluation to rule out dangerous secondary causes.
Part 2: Treatment & Management
💊 Acute (Abortive) Treatments
For Tension-Type Headache:
- Simple analgesics: Paracetamol (acetaminophen), Ibuprofen, Aspirin, Naproxen
- Combination analgesics: Caffeine + paracetamol + aspirin combinations
- Avoid overuse (>10–15 days/month) to prevent Medication Overuse Headache (MOH)
For Migraine:
| Drug Class | Examples | Notes |
|---|---|---|
| NSAIDs | Ibuprofen, Naproxen, Aspirin | First-line for mild-moderate attacks |
| Triptans (5-HT1B/1D agonists) | Sumatriptan, Rizatriptan, Zolmitriptan | Gold standard for moderate-severe migraine |
| Gepants (CGRP receptor antagonists) | Ubrogepant, Rimegepant | Newer class; no cardiovascular risk; useful if triptans are contraindicated |
| Ditans (5-HT1F agonists) | Lasmiditan | Newer class; does not cause vasoconstriction |
| Ergotamine derivatives | Ergotamine, Dihydroergotamine (DHE) | For prolonged attacks; use is more limited now |
| Antiemetics | Metoclopramide, Prochlorperazine | Adjunct to treat nausea and can enhance absorption |
For patients with severe nausea/vomiting, non-oral routes (nasal sprays, injections, suppositories) are preferred. (Integrating New Migraine Treatments, p. 13)
For Cluster Headache:
- 100% high-flow oxygen (10–15 L/min via non-rebreather mask) - highly effective
- Sumatriptan injection (subcutaneous) - fastest acting triptan
- Zolmitriptan nasal spray
- Intranasal lidocaine - used as adjunct
🛡️ Preventive (Prophylactic) Treatments
| Drug Class | Examples | Used For |
|---|---|---|
| Beta-blockers | Propranolol, Metoprolol | Migraine prevention |
| Antidepressants (TCAs) | Amitriptyline | TTH & migraine prevention |
| Anticonvulsants | Topiramate, Valproate | Migraine prevention |
| CGRP monoclonal antibodies | Erenumab, Fremanezumab, Galcanezumab | Newer, highly targeted migraine prevention (monthly injections) |
| OnabotulinumtoxinA (Botox) | Botox injections | Chronic migraine (≥15 headache days/month) |
| Calcium channel blockers | Verapamil | Cluster headache prevention |
| Lithium | Lithium carbonate | Chronic cluster headache |
🧘 Non-Pharmacological Treatments
| Intervention | Evidence Level | Notes |
|---|---|---|
| Cognitive Behavioral Therapy (CBT) | Strong | Addresses pain catastrophizing and coping |
| Biofeedback | Strong | Teaches control of physiological responses like muscle tension |
| Relaxation training | Moderate | Progressive muscle relaxation, deep breathing |
| Aerobic exercise | Moderate | Regular exercise reduces migraine frequency |
| Sleep hygiene | Moderate | Consistent sleep schedule is key |
| Stress management | Moderate | Mindfulness, yoga |
| Acupuncture | Moderate | Supported for both TTH and migraine |
| Trigger identification & avoidance | Practical | Headache diary to track food, sleep, stress triggers |
| Hydration & regular meals | Practical | Dehydration and skipping meals are common triggers |
| Neuromodulation devices | Emerging | Transcranial magnetic stimulation (TMS), vagus nerve stimulation (VNS) |
Summary Table
| Type | Location | Quality | Severity | Duration | Key Features |
|---|---|---|---|---|---|
| Tension-Type | Bilateral | Pressing/band-like | Mild-Moderate | 30 min–7 days | No nausea, no autonomic symptoms |
| Migraine | Unilateral | Throbbing | Moderate-Severe | 4–72 hours | Nausea, light/sound sensitivity, aura possible |
| Cluster | Unilateral (periorbital) | Stabbing/burning | Severe-Excruciating | 15–180 min | Autonomic symptoms (tearing, red eye), restlessness |
| Secondary | Varies | Varies | Varies | Varies | Linked to underlying disease; red flags present |
Important: Always consult a healthcare professional for persistent, severe, or unusual headaches. Self-treatment is appropriate for mild, occasional headaches, but recurring or disabling headaches deserve formal evaluation and a personalized treatment plan.