Metallazone in dcmp
Reading File
search_medical_text
metolazone diuretic use in dilated cardiomyopathy heart failure
search_medical_text
metolazone mechanism action thiazide diuretic resistant heart failure
GradeResponse
GradeResponse
Metolazone in Dilated Cardiomyopathy (DCMP)
Overview
Metolazone is a thiazide-like diuretic used as an add-on agent for managing fluid overload in heart failure, including dilated cardiomyopathy. Its role is specifically in the context of diuretic resistance or inadequate response to loop diuretics alone.
Mechanism of Action
Metolazone acts at the distal convoluted tubule (and proximal tubule) to inhibit sodium-chloride reabsorption. When combined with a loop diuretic (e.g., furosemide, torsemide):
- It blocks compensatory distal tubular sodium reabsorption that occurs in response to loop diuretics
- This results in synergistic/enhanced natriuresis and diuresis
- The combination is sometimes called "sequential nephron blockade"
Clinical Use in DCMP / Heart Failure
Indication: Metolazone is added to loop diuretics when:
- There is diuretic resistance (inadequate urine output or weight loss despite adequate loop diuretic doses)
- The patient has refractory fluid overload in decompensated heart failure
- Volume overload persists despite escalating loop diuretic doses
Typical approach:
- Ensure adequate loop diuretic dose first
- If response is insufficient → add metolazone (typically 2.5–5 mg orally, 30 minutes before the loop diuretic)
- Monitor closely for electrolyte disturbances and renal function
Risks and Adverse Effects
Despite its utility, metolazone carries significant risks (Management of Heart Failure, p. 40):
| Adverse Effect | Clinical Significance |
|---|---|
| Hypokalemia | Risk of arrhythmias; monitor K⁺ closely |
| Hyponatremia | Particularly dangerous in heart failure patients |
| Worsening renal function | Azotemia; monitor creatinine/BUN |
| Mortality risk | Propensity-matched analyses show increased mortality with metolazone vs. high-dose loop diuretics alone |
Evidence Considerations
- A propensity-score matched analysis in hospitalized HF patients showed that adding metolazone to loop diuretics increased risk of hypokalemia, hyponatremia, worsening renal function, and mortality compared to using higher doses of loop diuretics alone (Management of Heart Failure, p. 40)
- The DOSE trial (Diuretic Optimization Strategies Evaluation) lends support for high-dose IV loop diuretics as a preferred strategy before adding metolazone
- Randomized controlled data directly comparing metolazone combination vs. loop diuretic dose escalation remain limited
Key Takeaway
Metolazone can be a useful rescue diuretic in DCMP with decompensated heart failure and diuretic resistance, but it should be used cautiously and with close monitoring of electrolytes (K⁺, Na⁺) and renal function. Current evidence suggests preferring high-dose IV loop diuretics before adding metolazone, given the potential for serious adverse effects including increased mortality.
Infective endocarditis
Reading File
Finding Sources
Searching Images
infective endocarditis vegetation valve echocardiography
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Infective Endocarditis (IE)
Definition
Infective endocarditis is an infection — usually bacterial — of the endocardial surface of the heart, primarily affecting cardiac valves. It may also involve the septa, mural endocardium, prosthetic valves, pacemaker leads, or other cardiovascular implantable electronic devices (CIEDs). It leads to the formation of vegetations composed of thrombotic debris, fibrin, inflammatory cells, and organisms, often with destruction of underlying cardiac tissue. — Goldman-Cecil Medicine, p. 700; Robbins & Kumar Basic Pathology, p. 367
Classification
| Type | Course | Virulence | Substrate |
|---|---|---|---|
| Acute IE | Days; rapidly destructive | High (e.g., S. aureus) | Can attack normal valves |
| Subacute IE | Weeks to months; indolent | Low (e.g., viridans streptococci) | Requires damaged/deformed valves |
Note: The distinction is not always clear-cut — many cases fall along a spectrum. — Robbins, p. 367
Epidemiology
- Incidence: 3–14 cases per 100,000 persons/year in Western Europe and USA
- 10,000–20,000 new cases/year in the United States
- Accounts for ~1 case per 1,000 US hospital admissions
- S. aureus has emerged as the most common cause in most high-income countries, driven by healthcare-associated IE and injection drug use (IDU)
- The opioid epidemic has contributed significantly to rising IDU-related IE in rural settings
- Rheumatic heart disease, once the leading predisposing factor, has declined in developed countries — Braunwald's, p. [block10]; Goldman-Cecil, p. 700
Risk Factors / Predisposing Conditions
More Common:
- Mitral valve prolapse (especially with regurgitation) — now the leading preexistent risk factor
- Degenerative valvular disease
- Injection drug use
- Congenital heart disease (uncorrected VSD)
- Previous endocarditis
- Prosthetic heart valves (10–20% of all IE cases)
Less Common:
- Rheumatic heart disease
- Idiopathic hypertrophic subaortic stenosis
- Coarctation of the aorta
- Complex cyanotic congenital heart disease
- Pacemaker/CIED implantation
- IV catheters, hyperalimentation lines, hemodialysis
Host factors increasing risk: Neutropenia, immunodeficiency, HIV (risk increases as CD4 falls), malignancy, diabetes, alcohol use, end-stage renal disease on hemodialysis — Goldman-Cecil, p. 700–701; Robbins, p. 368
Pathogenesis
The sequence of events is predictable:
- Endothelial damage → turbulent blood flow (jets) disrupts endocardium
- Sterile vegetation (nonbacterial thrombotic endocarditis, NBTE) forms — platelet-fibrin deposits at damaged sites
- Transient bacteremia → seeding of the sterile vegetation
- Microbial proliferation within the vegetation (up to 10⁹–10¹¹ CFU/gram of tissue)
- Metastatic infection to high-flow organs — kidneys, spleen, brain
- Avascularity of valve surfaces impairs antibiotic penetration and healing
NBTE may also occur spontaneously in malignancy (marantic endocarditis) or SLE (Libman-Sacks endocarditis). — Goldman-Cecil, p. 701
Microbiology
| Organism | Setting | Type |
|---|---|---|
| Streptococcus viridans (VGS) | Community-acquired, damaged valves, oral procedures | Subacute |
| Staphylococcus aureus | Healthcare, IDU, healthy valves | Acute, aggressive |
| Enterococci | Genitourinary/GI procedures, elderly | Subacute |
| HACEK group (Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, Kingella) | Oral commensals | Subacute |
| Gram-negative bacilli, Fungi | Rare | Variable |
| Culture-negative (~10%) | Prior antibiotics or fastidious organisms | — |
— Robbins, p. 368; Goldman-Cecil, p. 701
Morphology / Pathology
- Vegetations: friable, bulky, potentially destructive masses on heart valves — containing fibrin, inflammatory cells, and microorganisms
- Aortic and mitral valves are most commonly affected (left-sided)
- Tricuspid valve predominates in IDU-related IE (right-sided)
- Vegetations may cause:
- Valve destruction, perforation, regurgitation
- Septic emboli (systemic in left-sided; pulmonary in right-sided)
- Chordae tendineae rupture
- Myocardial abscess formation (especially with S. aureus)
— Robbins, p. 368
Clinical Features
Symptoms (variable onset):
- Fever (most common), chills, night sweats, malaise, fatigue
- Back pain, arthralgia, myalgia
- Symptoms of heart failure (dyspnea, orthopnea)
- Neurological symptoms (embolic stroke, mycotic aneurysm)
Classic Peripheral Signs (more common in subacute IE):
| Sign | Description |
|---|---|
| Janeway lesions | Non-tender erythematous hemorrhagic macules on palms/soles (septic emboli) |
| Osler nodes | Tender, raised nodules on finger/toe pads (immune complexes) |
| Splinter hemorrhages | Linear hemorrhages under fingernails |
| Roth spots | Oval retinal hemorrhages with pale centers |
| Petechiae | Conjunctival, mucosal, skin |
| Clubbing | In chronic/subacute IE |
| Splenomegaly | In subacute IE |
Cardiac:
- New or changing murmur (regurgitant)
- Signs of heart failure
Diagnosis: Modified Duke Criteria
Major Criteria:
- Positive blood cultures (≥2 separate cultures with typical IE organisms, or persistent bacteremia)
- Evidence of endocardial involvement on echocardiography (oscillating vegetation, abscess, new prosthetic dehiscence, new valvular regurgitation)
Minor Criteria:
- Predisposing heart condition or IDU
- Fever ≥38°C
- Vascular phenomena (emboli, Janeway lesions, conjunctival hemorrhage)
- Immunological phenomena (Osler nodes, Roth spots, glomerulonephritis, positive rheumatoid factor)
- Microbiological evidence not meeting major criteria
Definite IE = 2 major, OR 1 major + 3 minor, OR 5 minor
Possible IE = 1 major + 1 minor, OR 3 minor
Rejected = Firm alternate diagnosis, resolution with ≤4 days antibiotics, or no pathological evidence at surgery/autopsy
Investigations
- Blood cultures: At least 3 sets from different sites before antibiotics — cornerstone of diagnosis
- Echocardiography:
- TTE (transthoracic echo) — first-line; sensitivity ~60–70% for native valves
- TEE (transesophageal echo) — gold standard; sensitivity >90%; preferred for prosthetic valves, poor TTE windows, high suspicion despite negative TTE
- CBC: leukocytosis, normocytic anemia
- ESR, CRP: elevated
- Urinalysis: hematuria, proteinuria (immune-complex glomerulonephritis)
- CT/MRI: for embolic complications (stroke, septic pulmonary emboli in right-sided IE)
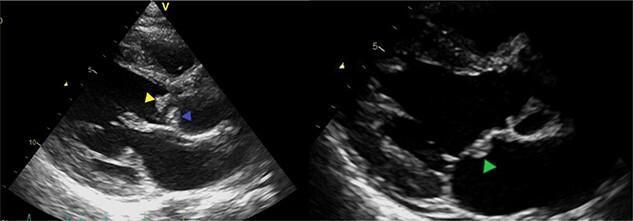
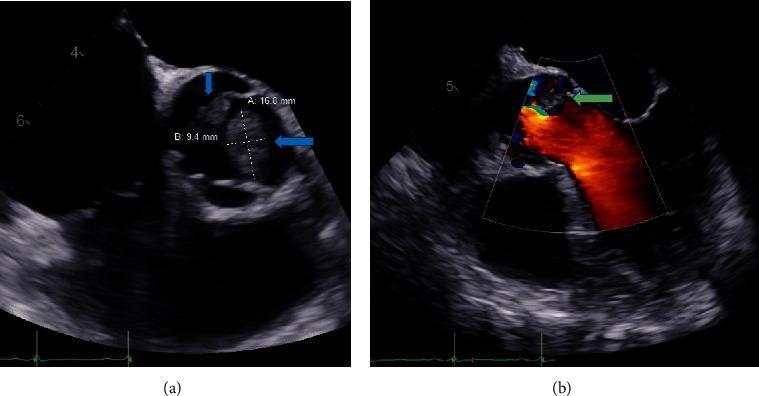
Echocardiographic Images

Management
1. General Principles
- Multidisciplinary team (Infectious Disease + Cardiology + Cardiac Surgery) — mandatory; managed at centers with IE expertise — Braunwald's, block10
- Inpatient management — all patients
- Prolonged IV antibiotics (4–6 weeks typically)
- Obtain blood cultures before starting antibiotics
2. Antibiotic Therapy (Empiric → Organism-Directed)
| Organism | Regimen |
|---|---|
| Viridans streptococci (penicillin-sensitive) | Penicillin G or Amoxicillin IV × 4 weeks; or + Gentamicin × 2 weeks (short course) |
| S. aureus (MSSA) — native valve | Nafcillin/Oxacillin IV × 6 weeks |
| S. aureus (MRSA) | Vancomycin IV × 6 weeks |
| Enterococci | Ampicillin + Gentamicin × 4–6 weeks (or Ampicillin + Ceftriaxone) |
| HACEK | Ceftriaxone × 4 weeks |
| Prosthetic valve MRSA | Vancomycin + Rifampicin + Gentamicin |
3. Surgical Indications
Early surgery is indicated for:
- Heart failure due to valve dysfunction (most common indication)
- Uncontrolled infection — abscess, fistula, enlarging vegetation, persistent bacteremia despite antibiotics
- Prevention of embolism — large vegetation (>10 mm) with prior embolic events
- Fungal IE
- Prosthetic valve dysfunction or dehiscence
4. AHA 2021 Prophylaxis Recommendations
Antibiotic prophylaxis (amoxicillin 2g PO, 30–60 min before dental procedure) is recommended for high-risk patients undergoing invasive dental procedures:
- Prosthetic cardiac valves/material
- Previous IE
- Unrepaired cyanotic CHD
- LVADs and implantable hearts
- Cardiac valve repair with devices
Clindamycin has been removed as an alternative (due to C. difficile risk); doxycycline added as alternative for truly penicillin-allergic patients — Braunwald's, block11
Complications
| Complication | Notes |
|---|---|
| Heart failure | Most common cause of death; acute AR or MR |
| Embolic stroke | ~20–40% of left-sided IE |
| Mycotic aneurysm | Intracranial; rupture risk |
| Perivalvular abscess | Especially S. aureus; AV block on ECG |
| Septic pulmonary emboli | Right-sided/IDU-related IE |
| Renal failure | Immune-complex GN or septic emboli |
| Splenic abscess | Requires drainage ± splenectomy |
Prognosis
- In-hospital mortality: 15–30%, higher with S. aureus, prosthetic valves, heart failure, and perivalvular complications
- Relapse rate ~10% for native valve IE
- Outcomes significantly improved with the multidisciplinary "endocarditis team" approach
Key Sources: Braunwald's Heart Disease (blocks 10–11) | Goldman-Cecil Medicine, p. 700–701 | Robbins & Kumar Basic Pathology, p. 367–369
This is a shared conversation. Sign in to Orris to start your own chat.