
1000162083.jpg
According to gynae. Datta book, Williamson ... Explain me with details plus cause, treatment, types everything
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Searching the Web
Williamson classification vesicovaginal fistula Datta gynecology genital tract injuries types
I now have comprehensive data from multiple authoritative sources. Let me compile the full detailed answer covering all the topics from the image.
Genital Tract Injuries, U-V Prolapse, Vesico-Vaginal Fistula, Recto-Vaginal Fistula, Complete Perineal Tear & Vaginal Stenosis
(Based on Datta's Gynecology, Bailey & Love's Short Practice of Surgery 28th Ed., Berek & Novak's Gynecology, Schwartz's Principles of Surgery, and Fischer's Mastery of Surgery)
1. GENITAL TRACT INJURIES
Genital tract injuries occur during childbirth (most commonly), surgery, or trauma. They involve the vulva, vagina, cervix, uterus, and perineum.
Causes
- Obstetric: Precipitate or prolonged labor, instrumental delivery (forceps, vacuum), large fetus (macrosomia), malposition, shoulder dystocia
- Surgical: Hysterectomy, anterior colporrhaphy, pelvic surgery
- Traumatic: Sexual assault, pelvic fractures, foreign body
- Congenital: Abnormal tissue
Types / Classification
| Site | Description |
|---|---|
| Perineal lacerations | 1st to 4th degree (see below) |
| Vaginal lacerations | Anterior, posterior, lateral walls; may be deep, bleeding may be concealed |
| Cervical lacerations | Common with instrumental delivery; may extend to uterine isthmus |
| Uterine rupture | Life-threatening; complete or incomplete |
| Vulvar/paravaginal hematoma | Rapid blood collection after vascular injury |
Management
- Vaginal lacerations: Inspect fully, repair primarily. Ensure apex is incorporated to prevent ongoing hemorrhage. Close in layers.
- Cervical lacerations: Running locking suture from apex downward. If apex is high, use distal suture for traction first.
- Hematoma: Small ones - conservative (observe, monitor). Expanding or patient-unstable - surgical incision and drainage; hemostasis with electrosurgery or fine absorbable sutures; packing if needed. Vaginal pack placed and removed at 24 hours.
2. UTEROVAGINAL (U-V) PROLAPSE
Pelvic organ prolapse is the protrusion/displacement of pelvic organs from their normal anatomical position into or through the vagina. It affects up to 40% of women at some point in their lifetime.
(Bailey & Love's Surgery, p. 1611)
Anatomical Types
| Type | Structure Prolapsing | Features |
|---|---|---|
| Urethrocele | Urethra only | Bulge in anterior wall |
| Cystocele | Bladder | Lump in vagina, urinary urgency, recurrent UTIs |
| Cystourethrocele | Bladder + urethra | Combined anterior wall prolapse |
| Uterine descent | Uterus descends | Dragging sensation, lump; procidentia = complete prolapse with ulceration |
| Enterocele | Small intestine (POD) | Posterior fornix bulge |
| Rectocele | Rectum into vagina | Difficulty defecating, incomplete emptying; relieved by digitation |
| Vaginal vault prolapse | Vault after hysterectomy | Posthysterectomy complication |
Risk Factors / Causes
- Older age, multiparity, prolonged or difficult vaginal labors
- Obesity, chronic constipation, heavy lifting occupations
- Estrogen deficiency (postmenopause - reduced tissue elasticity)
- Connective tissue disorders: Ehlers-Danlos syndrome, Marfan syndrome
- Family history / genetic predisposition
Grading - POP-Q System (Pelvic Organ Prolapse Quantification)
- Grade 0: No prolapse
- Grade 1: Distal portion of prolapse is >1 cm above the hymen
- Grade 2: Distal portion is ≤1 cm above or below the hymen
- Grade 3: Distal portion is >1 cm below the hymen but < (total vaginal length - 2 cm)
- Grade 4: Maximal descent - complete prolapse (procidentia)
Treatment
Non-surgical (Grade 1-2 preferred):
- Lifestyle modification: avoid constipation, reduce weight, avoid heavy lifting
- Pelvic floor physiotherapy for at least 16 weeks
- Topical estrogen (if estrogen deficient) - increases tissue strength
- Ring pessary: Most commonly used. Inserted between posterior fornix and pubic bone. Replaced every 3-6 months. Complications: vaginal ulceration, infection, discharge/bleeding.
Surgical (Table 87.12, Bailey & Love):
| Condition | Surgical Option |
|---|---|
| Cystocele/urethrocele | Anterior colporrhaphy (anterior vaginal wall repair, no mesh) |
| Uterine prolapse (family complete) | Vaginal hysterectomy ± sacrospinous fixation |
| Uterine prolapse (uterus preserving) | Manchester repair (cervical amputation + transverse cervical ligament suture); laparoscopic McCall suture; sacrohysteropexy |
| Enterocele | Hernial sac repair via vaginal mucosa opening |
| Vaginal vault prolapse | Sacrospinous fixation (vaginal) or sacrocolpopexy (abdominal/laparoscopic using mesh) |
| Rectocele | Posterior colpoperineorrhaphy (no mesh) |
| Patient unfit for surgery / no coitus | Colpocleisis |
Note: ~30% of women experience recurrence of symptoms after surgical treatment.
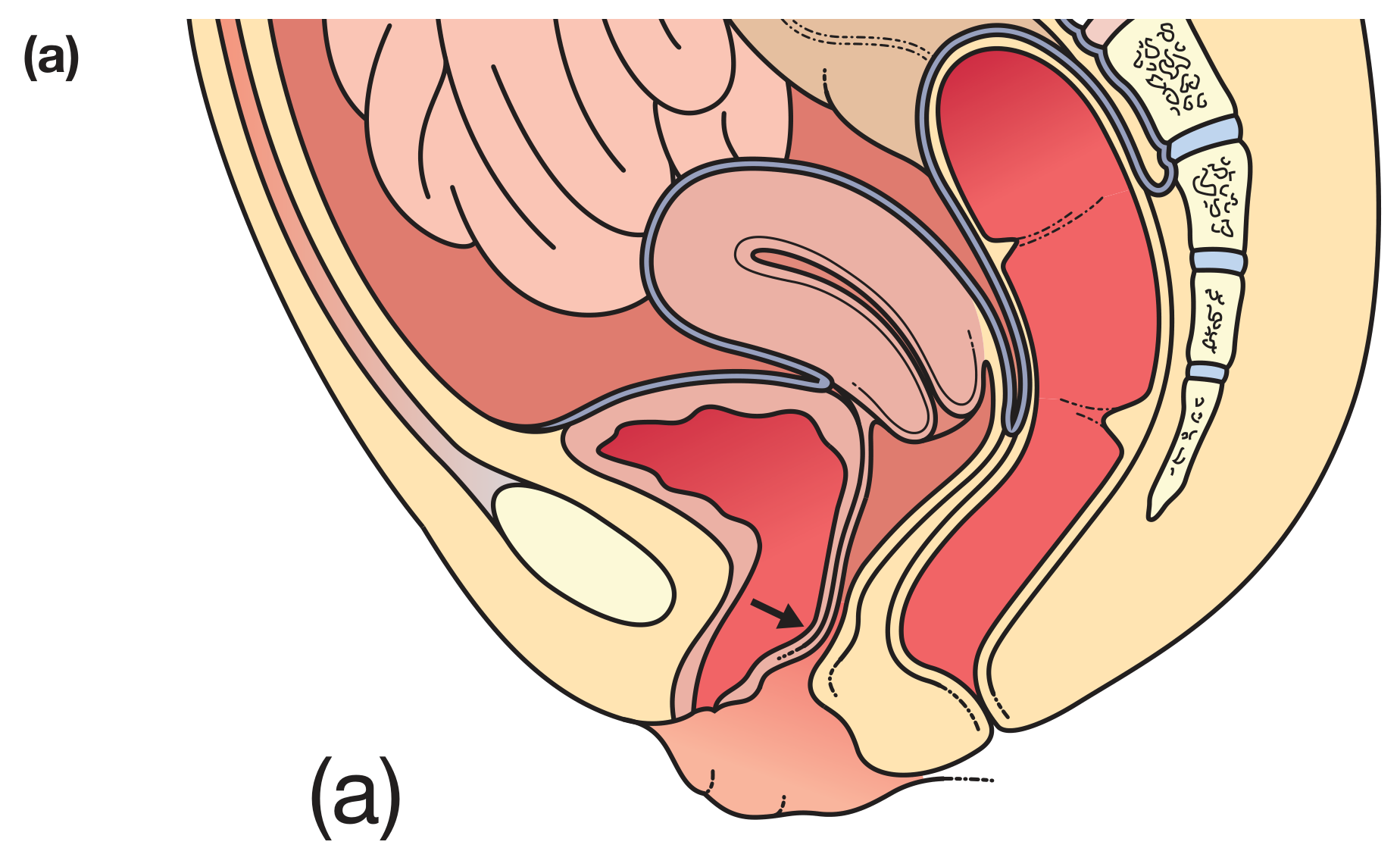
3. VESICO-VAGINAL FISTULA (VVF)
An abnormal communication between the bladder and the vagina resulting in continuous involuntary leakage of urine through the vagina.
Causes / Etiology
In developed countries: Post-surgical (most common) - most often after total abdominal hysterectomy for benign disease (incidence ~0.2%). Caused by:
- Failure to identify proper plane between bladder and cervix
- Blunt rather than sharp bladder dissection
- Incorrect clamping/suturing of vaginal cuff
- Unrecognized bladder laceration
In developing countries: Obstructed labor (ischemic pressure necrosis from prolonged impaction of fetal head against pelvis)
Other causes:
- Radiation therapy (for pelvic malignancy)
- Advanced pelvic malignancy
- Forceps laceration, uterine rupture, Cesarean section injury
- Anti-incontinence surgery, anterior colporrhaphy
- Infectious/inflammatory causes, foreign body
Types (Anatomical)
| Type | Location |
|---|---|
| Utero-vesical fistula | Between uterus and bladder |
| Cervico-vesical fistula | Cervix to bladder |
| Mid-vaginal VVF | Mid vagina to bladder |
| VVF involving bladder neck | At bladder neck |
| Urethro-vaginal fistula | Urethra to vagina |
Goh Classification (most widely used)
Based on distance from external urinary meatus (urethral length remaining):
- Type 1: Distal edge >3.5 cm from meatus (good prognosis)
- Type 2: 2.5-3.5 cm
- Type 3: 1.5-2.5 cm
- Type 4: <1.5 cm (worst prognosis - near/at bladder neck)
Size (a-c): (a) <1.5 cm; (b) 1.5-3 cm; (c) >3 cm
Scarring (i-iii): (i) None/mild fibrosis, vaginal length >6 cm; (ii) Moderate/severe fibrosis, reduced vaginal length; (iii) Special - post-radiation, ureteric involvement, circumferential fistula, previous repair
Simple vs. Complicated (OBG Management):
- Simple: <2-3 cm, supratrigonal, no radiation/malignancy, normal vaginal length
- Complicated: Previous radiation, malignancy present, shortened vagina, >3 cm, trigonal involvement
Clinical Features
- Continuous involuntary leakage of urine from vagina (most characteristic)
- Watery vaginal discharge appearing 10-14 days post-surgery (or 48-72 hours in early cases)
- Excoriation of vulva and thighs
- Recurrent UTIs, dyspareunia
Diagnosis
- Dye test (Double Dye test): Insert cotton tampon vaginally + instill methylene blue via urethral catheter. Blue staining = VVF confirmed.
- If no blue staining, give oral pyridium: orange staining within 20 minutes = ureterovaginal fistula
- CT urogram: Evaluates ureteral integrity, rules out obstruction
- Cystoscopy, vaginoscopy
Treatment
- Conservative (early): Insert Foley catheter for prolonged continuous bladder drainage. Up to 15% close spontaneously with 4-6 weeks of drainage.
- If no closure by 6 weeks: Surgical repair required
- Timing of surgery: Wait 3-4 months from diagnosis to allow inflammation to subside and improve vascular supply.
- Surgical approach: Vaginal repair for most post-hysterectomy fistulas (fistula site is above bladder trigone, away from ureters). Four-layer closure: (1) bladder mucosa, (2) seromuscular layer, (3) endopelvic fascia, (4) vaginal epithelium.
- Abdominal (O'Connor) or laparoscopic approach for complex/high fistulas.
- Martius flap (labial fat pad) used as interposing layer for complex cases.
4. RECTO-VAGINAL FISTULA (RVF)
An abnormal communication between the rectum and vagina, causing passage of flatus/feces through the vagina.
Types / Classification (by Location)
- Low RVF: Between lower rectum/anus and posterior vaginal wall near fourchette (most common obstetric type)
- Mid RVF: Mid-rectum to mid-vagina
- High RVF: High rectum or sigmoid to posterior vaginal fornix (usually related to Crohn's, diverticular disease, malignancy)
Goh Classification (anorectal-vaginal fistulas):
- Type 1: Distal edge >3 cm from hymen
- Type 2: 2.5-3 cm from hymen
- Type 3: 1.5-2.5 cm from hymen
Causes
- Obstetric (most common low RVF): Third or fourth-degree perineal tear with defect between the two viscera; unrecognized or improperly repaired sphincter injury
- Cryptoglandular infection: Anorectal abscess/fistula
- Iatrogenic: Previous surgical procedures
- Crohn's disease (perianal Crohn's)
- Diverticular disease, rectal malignancy, radiation injury (Fischer's Mastery of Surgery, p. 4304)
Clinical Features
- Passage of flatus and/or feces through vagina
- Fecal incontinence (large fistulas)
- Excoriation of perianal skin, raw red vagina
- Recurrent vaginal infections, dyspareunia
Diagnosis
- Vaginal speculum examination - identifies vaginal opening
- Proctoscopy/proctosigmoidoscopy - excludes malignancy, Crohn's, radiation damage; identifies dentate line opening (cryptoglandular origin)
- MRI perineum - most helpful for complex/obscure fistulas; almost always diagnostic
- Examination under anesthesia with fistula probes and dye injection
- Biopsy of any suspicious fistula to exclude malignancy
- Colonoscopy to identify inflammatory/malignant bowel disease
Treatment
Preliminary fecal diversion (colostomy) is MANDATORY for:
- Severe fecal incontinence
- Fistula complicated by pelvic sepsis
- Fistulas occurring within 2 weeks of vaginal birth
Definitive Surgical Treatment:
- High RVF (pouch of Douglas / posterior fornix): Resection when possible. For Crohn's, diverticular disease, or malignancy - bowel resection ± radical hysterectomy + partial vaginectomy
- Carcinoma of middle third rectum: Abdominoperineal excision + hysterectomy + partial vaginectomy; occasionally sphincter-saving procedures with coloanal anastomosis
- Low obstetric RVF: Direct layered perineal repair after adequate preparation (endorectal advancement flap, perineoproctotomy + layered closure, sphincteroplasty if sphincter defect present)
- Interposing tissue (Martius flap, gracilis muscle) for complex recurrent fistulas
5. COMPLETE PERINEAL TEAR (4th Degree)
A complete perineal tear (also called 4th degree laceration or obstetric anal sphincter injury - OASI) is one that extends through the entire perineal body, external AND internal anal sphincter, and the anorectal mucosa.
Classification of Perineal Lacerations
(Schwartz's Principles of Surgery, p. 1832-1833)
| Degree | Structures Involved |
|---|---|
| 1st degree | Perineal skin only; may or may not need repair |
| 2nd degree | Perineal body muscles (bulbocavernosus); vaginal mucosa; no sphincter involvement |
| 3rd degree | Perineum + external anal sphincter (EAS) |
| 4th degree / Complete | Perineum + EAS + internal anal sphincter (IAS) + anorectal mucosa |
In 4-5% of vaginal deliveries, the anal sphincter or anorectal mucosa is involved (3rd/4th degree tear).
Causes / Risk Factors
- Precipitate labor
- Large baby (macrosomia), occiput posterior position
- Instrumental delivery (forceps > vacuum)
- Shoulder dystocia
- Previous 3rd/4th degree tear
- Midline episiotomy (increases risk; mediolateral episiotomy is protective)
- Nulliparity, shorter perineum
Clinical Features
- Visible defect in perineum extending to anus
- Immediate postpartum bleeding
- If unrecognized/improperly repaired: fecal incontinence, RVF, perineal pain, dyspareunia
Repair (Surgical)
Sequence: Repair deepest layers first, then work superficially.
- Close anorectal mucosa first (interrupted 2-0 or 3-0 absorbable suture in submucosal layer)
- Close Internal Anal Sphincter (IAS) as a separate layer
- Reconstruct External Anal Sphincter (EAS): Identify severed ends and reconstruct using:
- End-to-end technique (approximation), OR
- Overlapping technique (preferred for EAS, better long-term continence)
- Then proceed with 2nd-degree repair: Approximate perineal body, vaginal epithelium from apex down, perineal skin closed subcuticularly.
Suture: 2-0 or 3-0 synthetic delayed absorbable (polyglycolic acid).
Incomplete reconstruction of 3rd/4th-degree tears leads to pelvic floor disorders, fecal incontinence, and future fistula formation.
Follow-up
- Stool softeners, laxatives
- Broad-spectrum antibiotics (to prevent infection of repair)
- Pelvic floor physiotherapy postoperatively
- Long-term follow-up for continence assessment
6. VAGINAL STENOSIS
Narrowing or obliteration of the vaginal lumen, which may be congenital or acquired.
Causes
- Post-radiation therapy (most common acquired cause for gynecologic malignancy) - fibrosis and scarring
- Post-surgical: After colpocleisis, vaginoplasty, fistula repair, or radical surgery
- Post-obstetric: Poorly repaired perineal tears, excessive tissue excision during episiotomy repair
- Inflammatory: Lichen sclerosus, lichen planus, pemphigoid
- Congenital: Imperforate hymen, transverse vaginal septum, vaginal agenesis (Mayer-Rokitansky syndrome)
- Infections: Severe chronic infections, tropical infections
Types / Classification (by site)
- Distal (introital) stenosis: Near vaginal opening - most common post-obstetric or post-surgical
- Mid-vaginal stenosis: Most common site after radiation
- Proximal stenosis: Near vault - post-hysterectomy, radiation
- Complete stenosis: Entire vaginal canal obliterated (severe radiation damage)
Clinical Features
- Dyspareunia (painful intercourse) or inability to have intercourse
- Difficulty with vaginal examination and speculum insertion
- Difficulty with vault smear follow-up after cervical cancer treatment
- Urinary symptoms if involving anterior wall
Treatment
- Vaginal dilators: Progressive dilation using vaginal trainers/dilators, starting from smallest size; combined with topical estrogen cream. First-line treatment after radiation therapy.
- Surgical: Incision/excision of scar tissue; vaginal reconstruction with skin grafts (McIndoe procedure for vaginal agenesis) or flaps (gracilis, pudendal thigh flap) for severe cases
- Topical estrogen: Improves tissue quality and elasticity
- Postoperative dilation is mandatory after surgical repair to prevent re-stenosis
Summary Table
| Condition | Key Feature | Key Treatment |
|---|---|---|
| Genital tract injuries | Obstetric/surgical trauma; hematoma | Layered repair; drain hematoma |
| U-V Prolapse | Protrusion of pelvic organs | Pessary (conservative); colporrhaphy/hysterectomy (surgical) |
| VVF | Continuous urine leakage per vaginum | Foley drainage 6 weeks; then 4-layer surgical repair |
| RVF | Flatus/feces per vaginum | Fecal diversion; definitive layered repair/resection |
| Complete perineal tear (4th°) | Sphincter + rectal mucosa involved | Layered repair: mucosa → IAS → EAS → perineal body |
| Vaginal stenosis | Narrowed vaginal lumen | Vaginal dilators; estrogen; surgical reconstruction |
Note on "Williamson" Classification: The Williamson classification referenced in Datta's textbook specifically classifies VVF based on anatomical site in relation to the bladder trigone and urethra - the same principles as the Goh classification described above. It stratifies fistulas into simple (supratrigonal, small, no radiation) vs. complex (trigonal involvement, radiation, large, scarred) to guide surgical approach and predict prognosis. This is consistent with the Datta gynecology context of Indian postgraduate examinations.
(Sources: Bailey & Love's Short Practice of Surgery 28th Ed., p. 1611-1612; Berek & Novak's Gynecology; Schwartz's Principles of Surgery 11th Ed., p. 1832-1833; Fischer's Mastery of Surgery 8th Ed., p. 4304-4305)
This is a shared conversation. Sign in to Orris to start your own chat.