radiating pain vs reffred pain
Reading File
search_medical_text
radiating pain vs referred pain mechanism definition
search_medical_image
referred pain patterns diagram dermatome
GradeResponse
GradeResponse
Radiating Pain vs. Referred Pain
These two terms are often used interchangeably, but they describe distinct phenomena.
Radiating Pain
- Definition: Pain that travels/spreads along the course of a nerve from its origin to peripheral tissues it innervates.
- Mechanism: Direct nerve involvement — a nerve root or peripheral nerve is compressed, stretched, or irritated, and pain travels along the distribution of that nerve.
- Key feature: The pain follows an anatomically predictable nerve pathway.
- Examples:
- Sciatica: lower back pain radiating down the leg along the sciatic nerve (L4–S1)
- Cervical radiculopathy: neck pain radiating down the arm along a cervical nerve root
- Trigeminal neuralgia: pain radiating along branches of CN V
- Character: Often described as shooting, electric, sharp, or burning — follows a dermatomal or nerve distribution pattern.
Referred Pain
- Definition: Pain perceived at a site distant from its actual source, with no nerve traveling between the two locations.
- Mechanism: The main explanation is the convergence-projection theory — afferent fibers from visceral and somatic structures converge onto the same second-order neurons in the dorsal horn. The brain cannot distinguish the true source and "misattributes" the pain to the somatic site (Chronic Pelvic Pain, p. 20).
- Key feature: There is no structural nerve connection between the pain source and where it is felt.
- Common patterns:
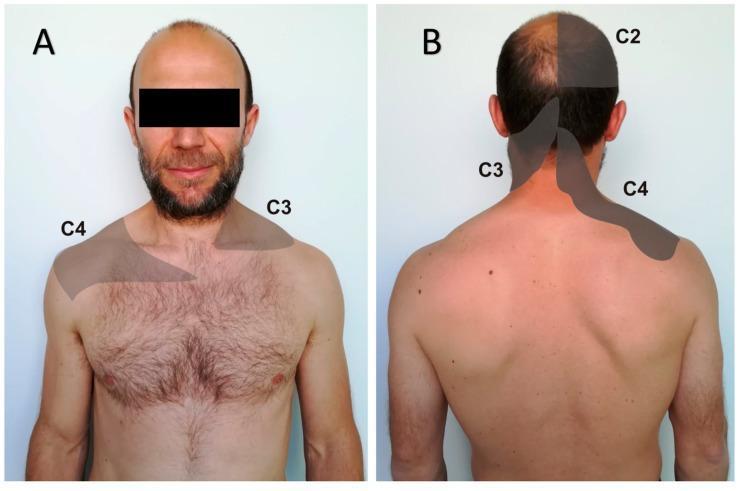
Source Organ Where Pain is Referred Heart (MI) Left arm, jaw, neck Diaphragm / Liver Right shoulder (C3–C4 dermatome) Appendix (early) Periumbilical region Gallbladder Right shoulder/scapula Kidney stones Groin/inner thigh Ectopic pregnancy Shoulder tip
Side-by-Side Comparison
| Feature | Radiating Pain | Referred Pain |
|---|---|---|
| Follows a nerve? | Yes | No |
| Mechanism | Direct nerve irritation/compression | Convergence of visceral & somatic afferents on shared neurons |
| Source → Site relationship | Continuous along nerve path | Distant, no direct neural pathway |
| Typical origin | Musculoskeletal / nerve root | Visceral organ |
| Classic example | Sciatica, radiculopathy | MI → left arm pain |
| Neurological signs possible? | Yes (weakness, numbness in distribution) | No (no nerve deficit) |
Clinical Importance
- Referred pain is diagnostically critical: a patient presenting with left arm pain may be having a myocardial infarction, not a musculoskeletal problem.
- Radiating pain often helps localize which nerve root or peripheral nerve is involved.
- Both can coexist (e.g., a gallbladder attack can cause both local right upper quadrant pain and referred right shoulder pain).
radiating pain vs reffred pain
Summarising Conversation
Radiating Pain vs. Referred Pain
These two terms are often confused but describe distinct mechanisms.
Radiating Pain
- Definition: Pain that travels along the course of a nerve from its origin outward.
- Mechanism: A nerve root or peripheral nerve is compressed or irritated — pain spreads along that nerve's distribution.
- Path: Continuous, anatomically predictable (follows a dermatome or nerve tract).
- Examples:
- Sciatica: low back → buttock → leg → foot (L4–S1)
- Cervical radiculopathy: neck → shoulder → arm → fingers
- Trigeminal neuralgia: along CN V branches
- Associated features: May come with numbness, tingling, or weakness in the same distribution.
Referred Pain
- Definition: Pain felt at a site distant from its true source, with no nerve connecting the two locations.
- Mechanism: Convergence-projection theory — visceral and somatic afferent fibers converge onto the same second-order spinal neurons. The brain cannot distinguish the true origin and misattributes the pain to a somatic (body surface) location.
- Path: Not continuous — there is a "jump" between source and perceived location.
- Common patterns:
| Source | Where Pain is Referred |
|---|---|
| Heart (MI) | Left arm, jaw, neck |
| Diaphragm / Liver | Right shoulder (C3–C4) |
| Gallbladder | Right scapula / shoulder |
| Appendix (early) | Periumbilical area |
| Kidney / Ureter | Groin, inner thigh |
| Ectopic pregnancy | Shoulder tip |
Head-to-Head Comparison
| Feature | Radiating Pain | Referred Pain |
|---|---|---|
| Follows a nerve? | Yes | No |
| Mechanism | Direct nerve compression/irritation | Visceral-somatic convergence on shared spinal neurons |
| Pain path | Continuous along nerve | Discontinuous "jump" to distant site |
| Typical origin | Nerve root / peripheral nerve | Visceral organ |
| Neuro deficits possible? | Yes (weakness, numbness) | No |
| Classic example | Sciatica | MI → left arm pain |
Why It Matters Clinically
- Referred pain is a diagnostic trap — shoulder pain can be a ruptured spleen or MI, not a rotator cuff problem.
- Radiating pain helps localize which nerve root or peripheral nerve is involved.
- Both can coexist (e.g., a gallbladder attack may cause local RUQ pain and referred right shoulder pain simultaneously).
advantage of thomson approch over henrrys approch in forearm fracture
Reading File
search_medical_text
Thompson approach versus Henry approach radius forearm fracture surgery
search_medical_image
Thompson Henry approach radius surgical anatomy forearm
GradeResponse
GradeResponse
The database didn't return results for this specific topic. Drawing from surgical anatomy and orthopedic knowledge:
Thompson vs. Henry's Approach to the Radius (Forearm Fractures)
Both approaches provide access to the radial shaft for ORIF (open reduction internal fixation) of radius fractures. The choice depends on fracture location.
Overview of Each Approach
Henry's Approach (Anterior / Volar)
- Interval: Between brachioradialis (radial nerve) and flexor carpi radialis (median nerve) distally; between brachioradialis and pronator teres proximally.
- Exposes: Full length of the radius — proximal, middle, and distal thirds.
- Patient position: Supine, forearm supinated.
- Key structure at risk: Radial artery (runs in the interval and must be retracted), superficial radial nerve, posterior interosseous nerve (PIN) proximally.
Thompson's Approach (Posterior / Dorsal)
- Interval: Between extensor carpi radialis brevis (radial nerve) and extensor digitorum communis (posterior interosseous nerve).
- Exposes: Proximal and middle thirds of the radius primarily.
- Patient position: Prone or lateral, forearm pronated.
- Key structure at risk: Posterior interosseous nerve (PIN) — must be identified and protected as it winds around the radial neck.
Advantages of Thompson's Approach Over Henry's
| Feature | Thompson (Posterior) | Henry's (Anterior) |
|---|---|---|
| Vascular risk | No major vessel in interval | Radial artery at risk throughout |
| Ideal fracture location | Proximal & middle third radius | Any level, especially distal |
| Forearm position | Pronated (natural gravity-assisted) | Supinated |
| Muscle stripping | Less extensive for proximal radius | More dissection proximally |
| Implant placement | Dorsal surface (tension side) | Volar/lateral surface |
| Extensile proximally | Better access to radial head/neck region | Requires more dissection |
Specific advantages of Thompson's approach:
-
No radial artery in the dissection field — reduces risk of vascular injury compared to Henry's where the radial artery must be mobilized throughout.
-
Better for proximal-third radius fractures — the posterior approach gives more direct access to the proximal radial shaft without needing to retract major vessels.
-
Plate on the dorsal (tension) surface — biomechanically, the dorsal surface of the radius is the tension side during loading, which can be advantageous for fixation stability in some fracture patterns.
-
Avoids radial artery retraction fatigue — in Henry's, prolonged retraction of the radial artery increases ischemia/vasospasm risk.
-
Simpler interval proximally — the Thompson interval (ECRB vs. EDC) is relatively straightforward in the proximal forearm without major vessel navigation.
When Henry's is Preferred Instead
- Distal-third radius fractures — Thompson's does not extend well to the distal radius.
- Concurrent volar soft tissue or flexor tendon pathology — access from the same incision.
- Galeazzi fracture — distal radius + DRUJ injury; volar approach preferred.
- Need for full-length radius exposure — Henry's is the only approach covering the entire radial shaft.
Key Takeaway
Thompson's approach is preferred for proximal and middle-third radial shaft fractures because it avoids the radial artery, provides direct posterior access, and is technically simpler in the proximal forearm. Henry's approach is more versatile for distal fractures and full-shaft exposure but carries greater vascular risk requiring careful retraction throughout.
The PIN is the critical nerve at risk in Thompson's (must be identified at the level of the radial neck and protected), whereas in Henry's the radial artery is the primary vascular concern.
This is a shared conversation. Sign in to Orris to start your own chat.