Cervical Cancer
Reading File
Finding Sources
Searching PubMed
"cervical cancer"[MeSH Terms] AND ("screening" OR "treatment")
Searching the Web
cervical cancer 2025 2026 guidelines screening treatment updates
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Excellent - I now have comprehensive content covering epidemiology, pathobiology, clinical features, staging, and treatment. Let me compile the full answer.
Cervical Cancer
Epidemiology
Cervical cancer is the third most common gynecologic cancer in the United States. Over 14,000 new cases and more than 4,000 cancer-related deaths occur annually in the US. A greater than 80% decline in incidence since the 1950s is directly attributed to screening - first with Papanicolaou (Pap) cytology and now with high-risk HPV testing. Despite this progress in developed nations, cervical cancer remains a leading cause of cancer death in women worldwide, particularly in Central/South America and Africa, due to limited access to screening and treatment.
Cervical cancer presents at a median age of 48 years. Disparities exist, with higher rates among Hispanic and Black American women.
Etiology - HPV is Central
HPV infection is detected in >99% of cervical cancers and is the essential etiologic agent.
- There are >200 HPV strains; ~40 infect the genital tract
- Low-risk HPV (e.g., types 6, 11): causes genital warts
- High-risk HPV: causes anogenital and oropharyngeal cancers
- HPV 16 & 18 cause 70% of cervical cancers
- HPV 31, 33, 45, 52, 58 cause an additional 20%
- HPV is sexually transmitted (genital-genital or genital-oral contact); most sexually active individuals will be infected at some point, usually early in sexual activity
Risk Factors
| Category | Specific Factors |
|---|---|
| Sexual behavior | Early onset of sexual activity, multiple sexual partners |
| Viral | HPV 16/18 infection (50-fold increase in precancerous lesion risk) |
| Immune status | HIV infection, other immunodeficiency states |
| Reproductive | Multiparity |
| Hormonal | Long-term oral contraceptive use (>5 years), in utero DES exposure |
| Lifestyle | Cigarette smoking |
| Socioeconomic | Lower socioeconomic status, lack of screening access |
| Demographic | Hispanic and Black American women |
A 2007 meta-analysis found a pooled RR of 1.9 (95% CI: 1.69-2.13) for invasive cervical cancer with 5+ years of OC use; this risk returned to baseline within 10 years of stopping. An IUD was associated with approximately one-third reduction in invasive cervical cancer risk.
Pathobiology
HPVs are small, non-enveloped, double-stranded DNA viruses with a capsid formed by late proteins L1 and L2.
Oncogenic mechanism:
- HPV infects the basal cell layer of stratified squamous epithelium at the squamocolumnar junction (transformation zone) of the cervix
- The E6 and E7 oncoproteins of high-risk HPV types are the primary drivers of carcinogenesis:
- E6 binds to and degrades p53 (tumor suppressor), inhibiting apoptosis and contributing to cellular immortalization
- E7 binds to and degrades pRB (retinoblastoma protein) and disrupts cyclins and cyclin-dependent kinases - dysregulating the cell cycle
- Both E6 and E7 have immunosuppressive effects, contributing to immune evasion
Natural history:
- Most HPV infections are transient and clear within 1-2 years
- In ~10% of infected women, HPV persists - producing viral proteins continuously
- Persistent HPV infection is necessary for the development of precancerous cervical intraepithelial neoplasia (CIN) and invasive cancer
- The carcinogenic process takes approximately a decade to progress to malignancy
- The squamocolumnar junction is most susceptible in adolescents and younger women, with declining susceptibility as the cervix matures hormonally
Histology: ~80-85% squamous cell carcinoma; ~10-15% adenocarcinoma (rarer, harder to detect on Pap smear, incidence appears to be increasing)
Precancerous Lesions (CIN)
| Grade | Description |
|---|---|
| CIN 1 (LSIL) | Low-grade dysplasia; often regresses spontaneously |
| CIN 2 | Moderate dysplasia |
| CIN 3 / CIS | High-grade dysplasia / carcinoma in situ; high risk of progression |
Clinical Manifestations
Early-stage disease is largely asymptomatic - detected by screening.
Advanced disease may present with:
- Abnormal vaginal bleeding (postcoital bleeding is classic)
- Vaginal discharge (may be watery, bloody, or foul-smelling)
- Pelvic pain or pain with intercourse (dyspareunia)
- Bowel or bladder dysfunction (hematuria, rectal bleeding) in very advanced disease
- Flank pain from ureteral obstruction
Spread: Local extension to the uterine corpus, vagina, bladder, and parametria is typical. Lymphatic spread to pelvic and para-aortic nodes.
Diagnosis
- Pap smear - detects abnormal cytology; primary screening tool
- HPV testing - high-risk HPV DNA testing (co-test or primary HPV screen)
- Colposcopy - directed biopsy of abnormal areas under magnification
- Cone biopsy / LEEP - for women without gross lesions or with microinvasive disease to define depth of invasion
- Direct biopsy - for obvious lesions; Pap smear is not adequate diagnostically in these cases
Staging (FIGO 2018)
The 2018 FIGO system incorporates imaging and pathologic findings (updated from the purely clinical 1971 system).
| Stage | Description |
|---|---|
| I | Confined to cervix |
| IA | Microscopic invasive carcinoma; depth ≤5 mm |
| IA1 | Depth ≤3 mm |
| IA2 | Depth 3-5 mm |
| IB | Clinically visible lesion or microscopic >stage IA |
| IB1 | <2 cm (fertility-sparing surgery candidates) |
| IB2 | 2-4 cm |
| IB3 | >4 cm |
| II | Beyond cervix, not to pelvic wall or lower third of vagina |
| IIA | Without parametrial involvement |
| IIB | With parametrial involvement |
| III | Extends to pelvic wall, lower third vagina, or causes hydronephrosis; includes nodal metastases (added 2018) |
| IIIC1 | Pelvic lymph node metastases |
| IIIC2 | Para-aortic lymph node metastases |
| IVA | Adjacent organ invasion (bladder/rectum) |
| IVB | Distant metastases |
Incidence by stage at diagnosis: Stage I 38%, Stage II 32%, Stage III 26%, Stage IV 4%.
CT scan demonstrating stage IVA cervical cancer (tumor invading bladder wall, hydronephrosis, and enlarged pelvic lymph node):
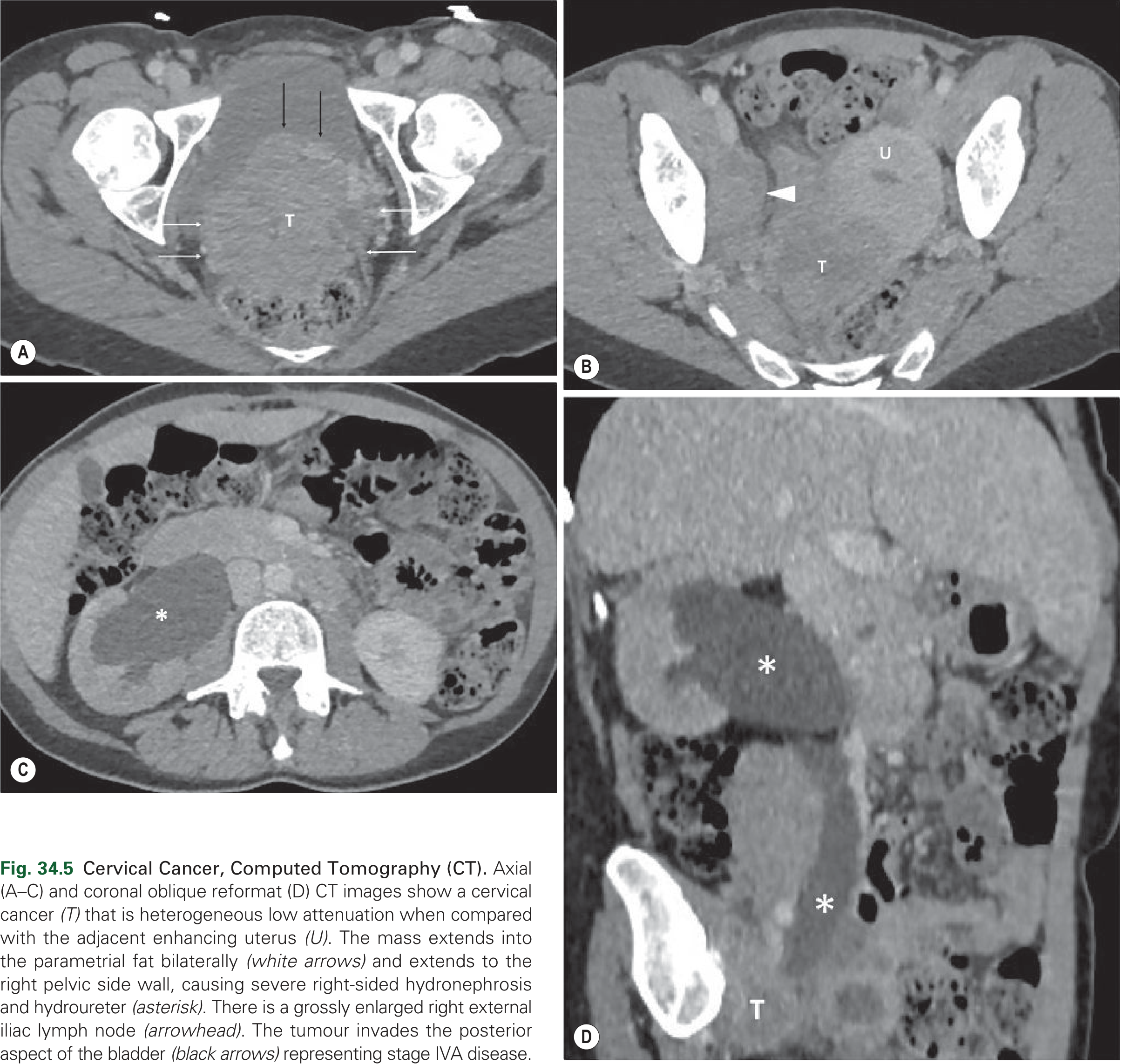
From Grainger & Allison's Diagnostic Radiology: Axial and coronal CT images show a heterogeneous cervical tumor (T) extending into parametrial fat bilaterally, invading the posterior bladder wall (black arrows), causing right-sided hydronephrosis, and with an enlarged right external iliac lymph node - representing stage IVA disease.
Imaging in Staging
- MRI pelvis: best for local extent, parametrial involvement, and tumor size
- CT chest/abdomen/pelvis: assesses lymph nodes and distant metastases
- FDG-PET/CT: particularly useful for advanced disease (FIGO IIB-IVB); sensitivity 75-100% and specificity 87-100% for lymph node metastases; can detect unexpected supra-diaphragmatic nodal spread; less useful for early-stage (I-IIA)
- Cystoscopy and proctoscopy may be used for suspected bladder/bowel involvement
Treatment
Treatment is guided by stage, tumor size, fertility desire, age, and comorbidities. Survival is better when managed by a gynecologic oncologist.
Early-Stage Disease (Stage IA-IB1/IIA1)
| Situation | Treatment |
|---|---|
| Microscopic disease / Stage IA1 | Cone biopsy (conization) or LEEP may suffice |
| Low-volume disease limited to cervix | Radical hysterectomy (open approach preferred over minimally invasive - provides better disease-free survival) |
| Very-low-risk disease | Simple hysterectomy is an alternative |
| Fertility desired (selected patients, stage IB1) | Radical trachelectomy (removal of cervix only) |
Adjuvant Therapy Indications Post-Hysterectomy
When pathology reveals high-risk features: lymphovascular space invasion, deep cervical stromal involvement, larger-than-expected tumor, positive margins, parametrial involvement, or nodal metastases - adjuvant radiation therapy is recommended.
Locally Advanced Disease (Stage IIB-IVA)
Definitive chemoradiation is the standard of care:
- Weekly cisplatin (radiation sensitizer) + external beam radiation therapy (EBRT) + brachytherapy
Recurrent / Metastatic Disease
- Platinum-taxane doublet chemotherapy (e.g., cisplatin/paclitaxel or carboplatin/paclitaxel)
- Bevacizumab (anti-VEGF monoclonal antibody): added to chemotherapy; provides incremental survival benefit
- Pembrolizumab (PD-1 checkpoint inhibitor): used in combination with chemotherapy +/- bevacizumab for PD-L1-positive tumors
- Pelvic exenteration: highly selected patients with central recurrence; very morbid but curative in 25-50%
- Palliative localized radiation for symptom management
Screening Guidelines
| Age Group | Recommendation |
|---|---|
| <21 years | No screening |
| 21-29 years | Pap smear alone every 3 years |
| 30-65 years | Pap + HPV co-test every 5 years (preferred) OR Pap alone every 3 years OR primary HPV test every 5 years |
| >65 years | Discontinue if adequate prior negative screening |
| Post-hysterectomy (benign) | Discontinue |
Prevention: HPV Vaccination
- Gardasil-9 (9-valent): covers HPV 6, 11, 16, 18, 31, 33, 45, 52, 58 - potentially prevents up to 90% of cervical cancers
- Recommended: ages 9-26 routinely; may be given up to age 45 with shared decision-making
- Most effective when given before sexual debut (before HPV exposure)
- HPV vaccination does NOT eliminate the need for ongoing cervical cancer screening
Prognosis (5-Year Survival by Stage)
| Stage | Approximate 5-Year Survival |
|---|---|
| IA | ~93-98% |
| IB | ~80-90% |
| IIA | ~70-80% |
| IIB | ~65-70% |
| III | ~40-50% |
| IVA | ~15-20% |
| IVB | ~<10% |
Sources: Goldman-Cecil Medicine, 26th Ed.; Berek & Novak's Gynecology, 16th Ed.; Grainger & Allison's Diagnostic Radiology; Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.