Malaria
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"malaria" AND "diagnosis"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have thorough content. Let me compile the comprehensive answer.
Diagnosis & Investigations of Malaria
Sources: Harrison's Principles of Internal Medicine 22E (2025), Goodman & Gilman's Pharmacological Basis of Therapeutics, Sherris & Ryan's Medical Microbiology 8E, Park's Textbook of Preventive and Social Medicine
Core Principle
Malaria is NOT a clinical diagnosis. Any patient from or returning from a malarious area with fever must have blood smears prepared and examined immediately. A negative smear by an experienced microscopist effectively rules out malaria. - Harrison's, p.1810
1. Peripheral Blood Smear - The Gold Standard
The definitive diagnosis rests on demonstrating asexual forms of the parasite in stained peripheral blood smears.
Staining
- Giemsa stain at pH 7.2 - preferred Romanowsky stain
- Field's, Wright's, or Leishman's stains are acceptable alternatives
- Acridine orange (fluorescent dye) - allows more rapid diagnosis at low-level parasitemia, but cannot identify species
Thick Film vs. Thin Film
| Feature | Thick Film | Thin Film |
|---|---|---|
| Purpose | Screening / detection | Species identification |
| Sensitivity | 40-100x more concentrated | Lower |
| Preparation | Dried without fixing | Air-dried, fixed in anhydrous methanol |
| Examination | Oil immersion after staining unfixed | Oil immersion (x1000) |
| Result | Parasites per µL (using WBC count) | Parasites per 1000 RBCs |
- A minimum of 200 WBCs should be counted under oil immersion on the thick film
- Before declaring a thick smear negative, examine 100-200 fields
- Parasitemia is expressed as parasitized erythrocytes per 1000 RBCs on thin film, or per µL on thick film (assuming WBC 8000/µL if count unavailable)
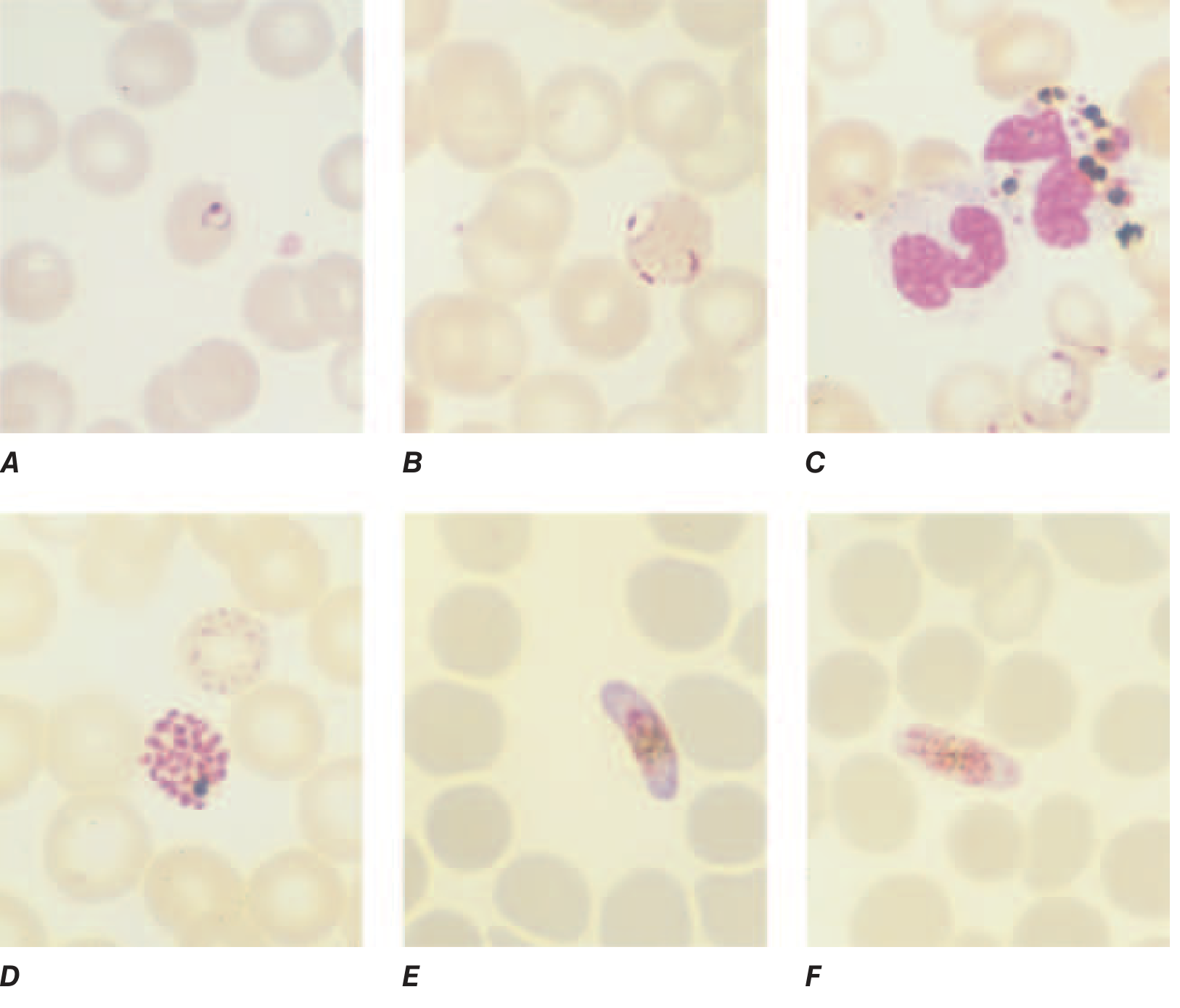
P. falciparum thin film appearances:
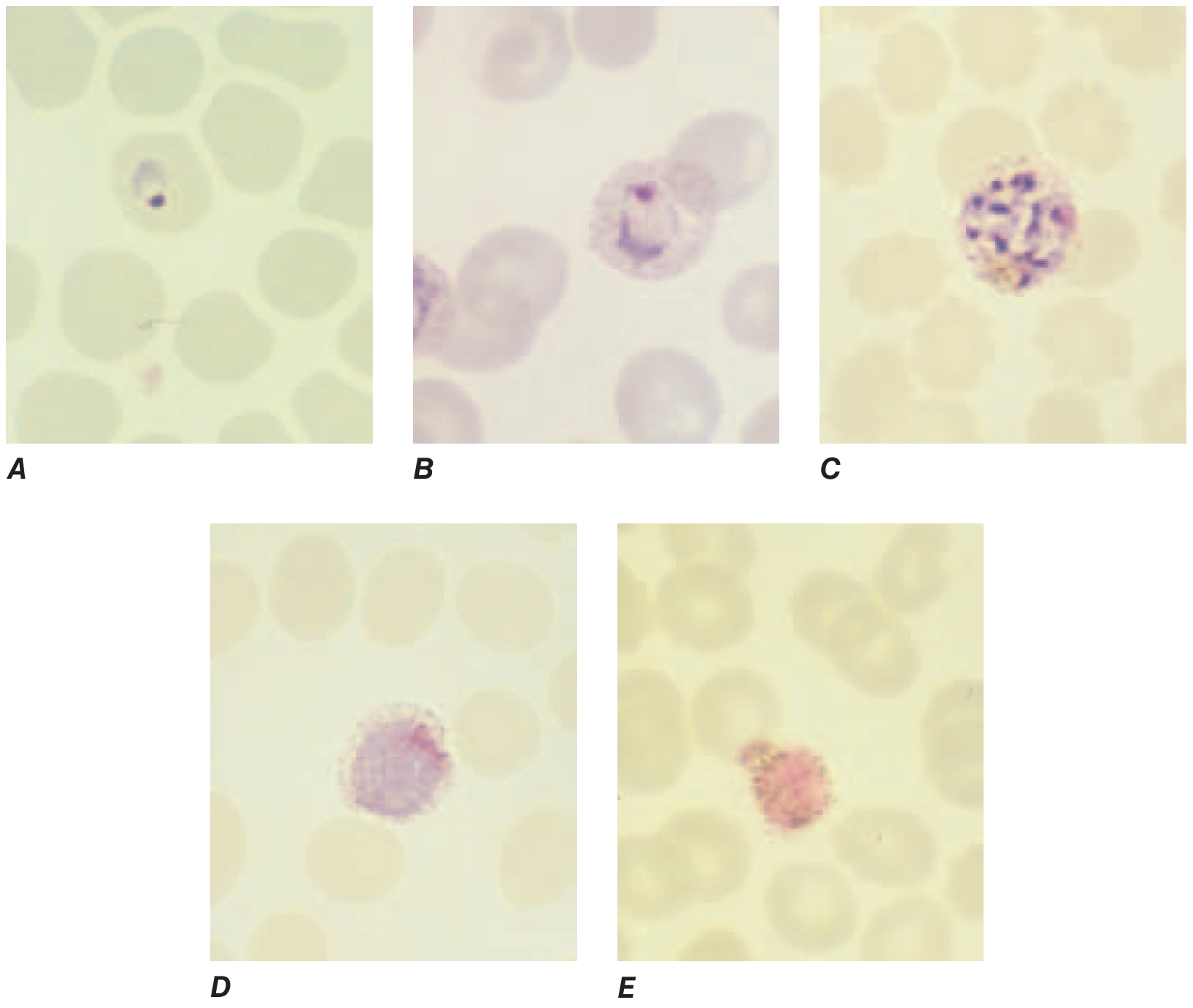
P. vivax thin film appearances:
2. Rapid Diagnostic Tests (RDTs)
When reliable microscopy is unavailable, an RDT must be performed. RDTs detect parasite antigens in finger-prick blood samples:
| Antigen Detected | Parasite | Notes |
|---|---|---|
| PfHRP2 (histidine-rich protein 2) | P. falciparum only | Remains positive for weeks post-infection - useful in severe malaria after drug clearance; risk of false-negative with PfHRP2/3 gene deletions (increasingly common in Horn of Africa) |
| pLDH (parasite lactate dehydrogenase) | Pan-malaria or species-specific | Clears more rapidly after treatment |
| Aldolase | Pan-malaria | Less common |
- Dual-antibody RDTs (PfHRP2 + pan-malaria or P. vivax-specific) can distinguish falciparum from non-falciparum malaria
- Key limitation: RDTs do not quantify parasitemia
- Smear should always accompany or follow an RDT to confirm species and assess parasite density
3. Parasitemia Density and Prognosis
- >10⁵ parasites/µL - increased risk of death
- Non-immune patients may die at lower counts; partially immune individuals may tolerate much higher counts
- Poor prognostic signs on smear in P. falciparum:
-
20% of parasites with visible pigment (mature forms)
- Malarial pigment in >5% of neutrophils (indicates recent schizogony)
-
- Gametocytemia of P. falciparum peaks ~1 week after peak of asexual parasitemia; gametocytes persist after treatment - do not indicate treatment failure
- Intraphagocytic malarial pigment in monocytes may suggest recent infection even if no live parasites visible
4. Molecular Diagnosis (PCR)
- More sensitive than both microscopy and RDTs for detecting parasites and identifying species
- Used in reference centres and for confirmation of low-density infections
- Not used for primary diagnosis in endemic areas due to cost and turnaround time
- Useful for detecting mixed infections, drug-resistance genotyping, and epidemiological studies
5. Supporting Laboratory Investigations
These are not diagnostic but help assess severity:
| Investigation | Typical Findings in Malaria |
|---|---|
| FBC | Anaemia (normocytic), thrombocytopenia |
| Blood film | Parasitaemia (as above) |
| Reticulocyte count | Raised (haemolytic anaemia) |
| LFTs | Raised bilirubin (jaundice from haemolysis), elevated transaminases |
| RFTs | Raised creatinine/urea in severe disease (acute kidney injury) |
| Blood glucose | Hypoglycaemia - especially with P. falciparum or quinine treatment |
| Coagulation screen | DIC in severe falciparum malaria |
| Blood cultures | To exclude co-infection with bacteraemia |
| Urinalysis | Haemoglobinuria ("blackwater fever" in severe P. falciparum) |
| Chest X-ray | If pulmonary oedema (ARDS) suspected |
| Lumbar puncture | If cerebral malaria vs bacterial meningitis cannot be distinguished |
6. Species Identification - Key Microscopy Differentials
| Feature | P. falciparum | P. vivax | P. ovale | P. malariae |
|---|---|---|---|---|
| RBC size | Normal or small | Enlarged | Slightly enlarged | Normal or small |
| Schüffner's dots | Absent (Maurer's clefts instead) | Present | Present | Absent |
| Trophozoite | Delicate ring, often multiple per RBC, "appliqué" (accolé) position | Amoeboid, irregular | Compact | Band form |
| Gametocyte | Crescent/banana-shaped (pathognomonic) | Round/oval | Round/oval | Round |
| Max. merozoites in schizont | 8-24 | 12-24 | 6-12 | 6-12 |
7. Approach by Clinical Setting
Where microscopy is available within 24 hours: Use smear as primary test, treat according to species identified.
Where microscopy is delayed and monovalent RDT (PfHRP2) is used: Treat positive as P. falciparum; if negative and symptoms persist, arrange microscopy.
Where bivalent RDT (PfHRP2 + pan) is used: Can distinguish falciparum from non-falciparum and guide treatment accordingly. (Park's Preventive Medicine, p.308)
In the United States: The CDC Malaria Hotline is available for guidance: (770) 488-7100 after hours / (855) 856-4713 toll-free. Smear is mandatory even if RDT is performed - results should be available as soon as possible. (Sherris & Ryan Medical Microbiology 8E, Fig. 51-7)
Summary Flow
Fever + travel to endemic area
↓
Thick + thin blood smear (Giemsa, ×1000)
↓
Positive → species ID + count parasitemia → guide treatment
Negative → repeat smear every 12-24h × 3 if clinical suspicion remains
↓
If microscopy unavailable → RDT immediately
↓
All positives → smear when possible to confirm species + density
↓
PCR if species uncertain or mixed infection suspected
This is a shared conversation. Sign in to Orris to start your own chat.