CVP monitoring for MD anaesthesia exam answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive data to write a thorough MD anaesthesia exam answer. Let me compile this into a complete, exam-quality response:
Central Venous Pressure (CVP) Monitoring - MD Anaesthesia Exam Answer
Definition
CVP is the pressure exerted by blood against the walls of the intrathoracic venae cavae. Because pressure in the venae cavae is generally within 1 mmHg of right atrial pressure, CVP reflects the pressure under which blood is returning to the heart. It is measured by placing a catheter tip in any of the great systemic veins of the thorax or the right atrium.
- Normal CVP: 2-8 mmHg (approximately 3-10 cmH2O)
- Conversion: 1 mmHg = 1.36 cmH2O
Physiology
CVP has two important hemodynamic effects:
- Preload determinant - promotes filling of the heart during diastole (reflects RV end-diastolic volume)
- Venous return back-pressure - opposes return of blood from the peripheral venous circulation to the heart
CVP values are determined by the interaction of:
- Intravascular volume
- Right atrial and ventricular function
- Venomotor tone
- Intrathoracic pressures
CVP reflects right heart filling pressure only. It does not reliably reflect left heart pressures unless both ventricles function normally.
- Miller's Anesthesia, 10e, p. 4806
The CVP Waveform
The normal CVP waveform has three positive deflections (waves) and two negative deflections (descents):
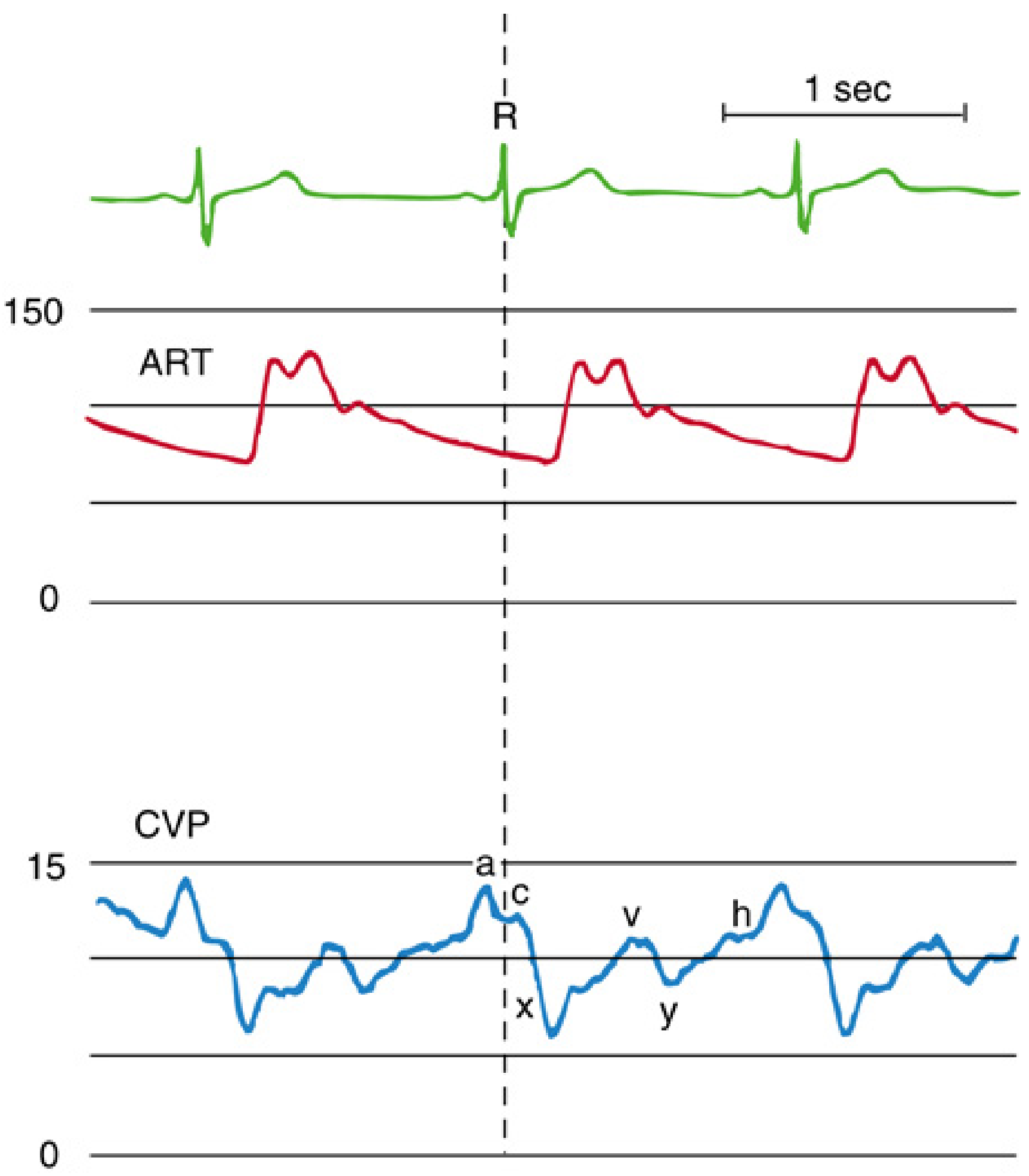
Waveform Components (Table)
| Component | Phase of Cardiac Cycle | Mechanical Event |
|---|---|---|
| a wave | End-diastole | Atrial contraction ("a = atrial kick") |
| c wave | Early systole | Isovolumic ventricular contraction; tricuspid valve closure moves toward RA |
| x descent | Mid-systole | Atrial relaxation + descent of tricuspid annulus toward apex (systolic collapse) |
| v wave | Late systole | Venous filling of atrium while tricuspid valve is closed |
| y descent | Early diastole | Tricuspid valve opens; blood flows from atrium to ventricle (diastolic collapse) |
| h wave | Mid- to late diastole | Diastolic plateau (only seen with slow heart rate or elevated CVP) |
Timing relative to ECG:
-
a wave follows the P wave
-
c wave follows the QRS (R wave)
-
v wave peaks just after the T wave
-
Miller's Anesthesia, 10e, p. 4806-4808
Abnormal CVP Waveforms
| Condition | Waveform Change | Mechanism |
|---|---|---|
| Atrial fibrillation | Loss of a wave; prominent c wave | No organised atrial contraction; greater atrial volume at onset of systole |
| AV dissociation / junctional rhythm / ventricular pacing | Cannon a waves | Atrium contracts against closed tricuspid valve |
| Tricuspid regurgitation | Tall systolic c-v wave; loss of x descent | Retrograde systolic filling of RA; "ventricularised" trace |
| Tricuspid stenosis | Tall a wave; attenuated y descent | Increased atrial work; slow diastolic emptying |
| RV ischaemia / pericardial constriction | Tall a and v waves; steep x and y descents; M or W configuration | Impaired RV compliance |
| Cardiac tamponade | Dominant x descent; attenuated y descent | Pericardial fluid limits diastolic filling |
Key exam pearl: In tricuspid regurgitation, the monitor displays an overestimated mean CVP. True RVEDP is best measured at the ECG R wave, before the regurgitant wave.
- Miller's Anesthesia, 10e, p. 4811-4813
Indications for CVP Monitoring
- Acute circulatory failure / haemodynamic instability
- Major surgery with anticipated large fluid shifts (esophagectomy, pneumonectomy, hepatic resection, cardiac surgery)
- Anticipated massive blood transfusion
- Cautious fluid replacement in patients with compromised cardiovascular status
- Suspected cardiac tamponade
- Fluid resuscitation in severe sepsis (goal-directed therapy)
- Additional uses of the central venous catheter (not purely for pressure monitoring):
- Administration of vasoactive drugs, total parenteral nutrition, chemotherapy, concentrated electrolytes
- Transvenous cardiac pacing
- Temporary haemodialysis
- Pulmonary artery catheter introduction
- Aspiration of venous air embolism
- Inadequate peripheral IV access
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 518; Miller's Anesthesia, 10e, p. 4792-4793
Contraindications
| Absolute | Relative |
|---|---|
| Other resuscitative interventions that take priority | Coagulopathy (prefer site compressible with direct pressure, e.g., internal jugular over subclavian) |
| SVC syndrome | Severe emphysema (subclavian approach risky) |
| Large vegetations on tricuspid valve | Infection at proposed insertion site |
| Right atrial tumour or thrombus | Thrombocytopenia |
Sites of Insertion
| Site | Advantages | Disadvantages |
|---|---|---|
| Right internal jugular | Best route to right heart; highest success rate; safe in coagulopathy (compressible); preferred for PA catheter and pacing | Risk of carotid puncture; patient discomfort; difficulty in obese/short necks |
| Subclavian | Comfortable for patient; lower infection risk | Higher pneumothorax risk (~2%); non-compressible if arterial puncture; avoid in emphysema/bilateral disease |
| Femoral | Easiest in emergency/resuscitation; no pneumothorax risk | Higher infection rate; DVT risk; less reliable CVP if intra-abdominal pressure elevated; slower drug delivery to central circulation |
| External jugular | Visible, safe | May kink; tortuous angle; less reliable positioning |
Catheter tip position: Superior vena cava, at the cavo-atrial junction. Confirmed by CXR. Tip within 2 cm of the cardiac silhouette on AP film.
Ultrasound guidance is strongly recommended (mandated by most guidelines) for internal jugular cannulation and should be considered for subclavian or femoral access.
- Miller's Anesthesia, 10e, p. 4792-4795
Measurement Technique
Manometric method (water column):
- Zero the manometer at the level of the right atrium (mid-axillary line, 4th intercostal space, with patient supine)
- Fill the column with IV fluid; open to the patient
- Water level falls and oscillates with respiration
- Read at end-expiration
Electronic transducer method:
- Transducer zeroed at the phlebostatic axis (same reference point as above)
- Provides continuous waveform display and digital mean value
- Read at end-expiration in spontaneously breathing patients; read at end-expiration (before ventilator breath) in mechanically ventilated patients
Sources of error in CVP measurement:
-
Failure to zero or calibrate the transducer
-
Incorrect reference point (transducer not at right atrial level)
-
Catheter tip malposition
-
Air bubbles in the circuit
-
Catheter obstruction
-
Reading during the wrong phase of ventilation
-
Increased intrathoracic pressure (IPPV, PEEP, coughing, straining, pneumothorax)
-
Vasopressors (may falsely elevate readings)
-
Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 518-519
Normal Values and the Fluid Challenge
Static CVP value alone is a poor predictor of volume status or fluid responsiveness - many studies have confirmed this. In shocked patients, there is no single "normal" CVP target; some patients need a CVP of 5 cmH2O while others may require 15 cmH2O or more. Ventricular compliance changes rapidly in shock, making CVP a poor reflection of RVEDP.
Dynamic assessment - the fluid challenge:
- Infuse 250-500 mL rapidly over 5-10 minutes
- Assess CVP response:
| Response | Interpretation | Action |
|---|---|---|
| No change in CVP | Volume depleted - empty ventricle, steep portion of Starling curve | Further fluid resuscitation |
| Rise of 2-5 cmH2O that drifts back to baseline over 10-20 minutes | Normal/adequate response | Continue monitoring |
| Large, sustained rise in CVP | High preload - cardiac insufficiency or volume overload | Stop fluids; consider inotropes |
- Bailey & Love's Short Practice of Surgery, 28e, p. 40
Limitations of CVP
This is a high-yield exam area. The main limitations are:
- Does not reflect left heart filling - PCWP (pulmonary artery occlusion pressure) is needed to estimate left atrial pressure
- Poor predictor of fluid responsiveness - static CVP cannot reliably predict whether a patient will respond to a fluid challenge (landmark meta-analyses have confirmed this)
- Affected by ventricular compliance - conditions like RV ischaemia, tamponade, pericardial constriction, and PEEP alter the CVP-volume relationship
- Intrathoracic pressure effects - IPPV, PEEP, and pneumothorax elevate CVP without a corresponding increase in preload
- Venomotor tone changes - vasoconstriction may maintain a "normal" CVP despite hypovolaemia
- Tricuspid valve disease - distorts waveform and numeric value
- Right vs. left heart discordance - in conditions with primary left heart failure or pulmonary hypertension, CVP may not reflect left-sided haemodynamics at all
- Practical sources of error (zeroing, tip position, ventilation phase - as above)
Current status: CVP has largely been supplanted in the ICU by dynamic preload indicators (pulse pressure variation [PPV], stroke volume variation [SVV]), point-of-care echocardiography, and functional haemodynamic tests. However, the central venous catheter remains indispensable for drug delivery, pacing, and haemodialysis.
- Barash's Clinical Anesthesia, 9e, p. 3161; Miller's Anesthesia, 10e, p. 4789-4790
Complications of CVP Catheterisation
Mechanical (immediate)
- Arterial puncture (most common acute complication; 1.9-15%)
- Pneumothorax (~2% with subclavian; less with internal jugular)
- Haemothorax, haemomediastinum, hydrothorax, chylothorax
- Cardiac tamponade - most life-threatening; results from tip perforation of intrapericardial SVC, RA, or RV (especially with malpositioned tip abutting at steep angle)
- Air embolism
- Catheter malposition (coiling, migration into wrong vessel)
- Nerve injury (brachial plexus, phrenic nerve)
Thromboembolic
- Deep vein thrombosis (especially femoral)
- Catheter-related thrombosis; pulmonary embolism
Infectious
- Catheter-related bloodstream infection (CRBSI / CLABSI)
- Up to 15% of patients experience some adverse event related to central venous catheterisation
Prevention
-
Ultrasound guidance
-
Maximal sterile barrier precautions (cap, mask, sterile gown and gloves, large sterile drape)
-
Checklist/protocol use
-
Tip confirmation by CXR before use
-
Waveform manometry or pressure measurement to confirm venous placement before securing
-
Miller's Anesthesia, 10e, p. 4795-4796
CVP vs. Other Haemodynamic Monitors
| Monitor | Measures | Advantage over CVP |
|---|---|---|
| PCWP (PA catheter) | Left atrial pressure surrogate; CO by thermodilution | Left heart filling; cardiac output; SVR |
| PPV/SVV | Dynamic preload responsiveness | Superior predictor of fluid response (in mechanically ventilated, sinus rhythm patients) |
| Echocardiography (TTE/TOE) | Direct ventricular volume; wall motion; valve function | Real-time, visual, no assumptions |
| Passive Leg Raise (PLR) | Functional fluid challenge | Reversible; valid even in arrhythmia, spontaneous breathing |
Key Exam Points to Remember
- CVP = RAP = RVEDP (only when tricuspid valve is normal and no pericardial constraint)
- The a wave is absent in atrial fibrillation
- Cannon a waves = AV dissociation (atrium contracts against closed tricuspid)
- Tricuspid regurgitation = "ventricularised" trace (c-v wave, loss of x descent)
- Tamponade = prominent x, attenuated y descent
- Constrictive pericarditis = deep x AND deep y descent (M/W pattern)
- Always read CVP at end-expiration
- Fluid challenge (250-500 mL) is more informative than a static CVP reading alone
- CVP is NOT a reliable single-time-point predictor of volume status or fluid responsiveness
- Ultrasound guidance is the current standard of care for central venous cannulation
Sources: Miller's Anesthesia, 10e (Elsevier); Barash's Clinical Anesthesia, 9e; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Bailey & Love's Surgery, 28e
This is a shared conversation. Sign in to Orris to start your own chat.