Acl reconstruction surgery in short with grafting and physiotherapy sports rehab week protocol
Reading File
Finding Sources
Finding Sources
Searching PubMed
"anterior cruciate ligament reconstruction" AND "rehabilitation protocol"
Finding Sources
Finding Sources
Searching the Web
ACL reconstruction surgery grafting options physiotherapy week by week sports rehabilitation protocol 2024
Reading File
Reading File
Reading File
Reading Web Page
ACL rehabilitation week by week protocol phases
Loading Image
Reading Web Page
ACL rehabilitation week by week phases return to sport criteria
I now have comprehensive information from Miller's Review of Orthopaedics, Rockwood & Green's Fractures, MGH protocol, and recent PubMed evidence. Here is the complete structured answer:
ACL Reconstruction: Surgery, Grafting & Sports Rehab Protocol
1. Anatomy & Mechanism of Injury
The ACL is the primary restraint to anterior tibial translation and resists internal rotation. Injuries typically occur via noncontact pivoting, cutting, or landing mechanisms — often with an audible pop followed by hemarthrosis within 12 hours. The Lachman test is the most sensitive acute examination; the pivot shift test correlates most closely with functional outcome.
2. Pre-Surgical Preparation ("Prehab")
- Avoid reconstruction in the acute inflammatory phase
- Achieve full ROM and good quadriceps control before surgery — this minimizes arthrofibrosis risk
- Immobilization is avoided; early motion and swelling control are prioritized
- Prehab: quad sets, heel slides, ROM exercises, straight leg raises (SLR)
3. Surgical Technique
ACL reconstruction is performed arthroscopically under general or spinal anaesthesia. The technique is single-bundle reconstruction in the vast majority of cases (double-bundle shows no difference in patient-reported outcomes).
Key Surgical Steps
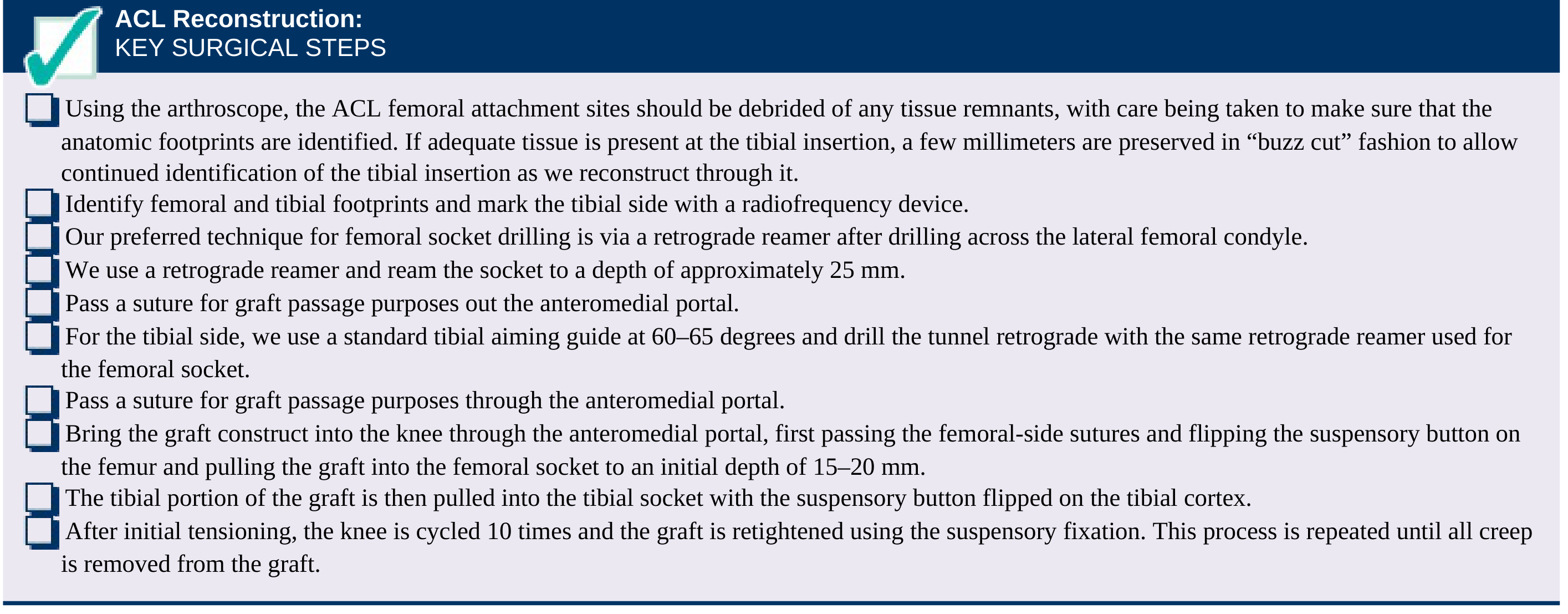
- Débride ACL femoral/tibial footprints (preserve tibial remnant if possible for proprioception)
- Drill femoral socket via retrograde reamer at the anatomic ACL origin on the lateral wall — ~25 mm deep (10–11 mm diameter)
- Drill tibial tunnel at 60–65° using tibial ACL guide, referencing the anterior horn of the lateral meniscus
- Pass graft through anteromedial portal; flip suspensory button on lateral femoral cortex
- Pull tibial limb into tibial socket; flip tibial suspensory button
- Cycle the knee 10 times; retighten until all creep is removed
- Final fixation (interference screw or suspensory device)
"Anatomic" reconstruction — femoral tunnel at 10- or 2-o'clock position centers the graft in the native footprint, reducing rotational instability compared to traditional transtibial drilling.
4. Graft Options
| Graft | Strengths | Weaknesses | Best For |
|---|---|---|---|
| Bone-Patellar Tendon-Bone (BPTB) Autograft | Fastest bone-to-tunnel incorporation; gold standard strength | Anterior knee pain, pain with kneeling, quad weakness, patellar fracture risk, higher arthritis risk at 5–7 yrs | Athletes demanding early return |
| 4-Strand Hamstring Autograft (semitendinosus ± gracilis) | Less donor site morbidity, lower arthritis risk | Less stiff than native ACL; risk of hamstring/hip IR weakness, saphenous nerve injury | Most common general use |
| Quadriceps Tendon Autograft | Strong, all-soft tissue possible, favorable early data | Larger incision, patellar fracture risk | Growing preference (especially knee dislocations <40 yrs) |
| Allograft | No donor site morbidity, shorter OR time | Slower incorporation; higher rupture rate in active patients <25; infection risk (1:6 million); avoid irradiated/chemically processed | Older/less active patients, revision, multi-ligament cases |
Chemically processed or irradiated allografts have significantly higher failure rates than fresh-frozen allograft. Autograft remains preferred in young, active athletes. — Miller's Review of Orthopaedics 9th Ed.
5. Graft Ligamentization ("Ligamentization Process")
The graft is weakest at weeks 4–8 — this is when avascular necrosis of the graft occurs (especially with autograft) before revascularization begins. This is the critical window when loading must be controlled.
| Timeframe | Biological Process |
|---|---|
| Weeks 1–3 | Graft avascularization, necrosis of central core |
| Weeks 4–8 | Weakest point — revascularization begins |
| Months 3–6 | Cellular repopulation, collagen remodeling |
| Months 6–12 | Progressive maturation toward ligament-like tissue |
| 12–24 months | Full maturation (allograft slower than autograft) |
6. Week-by-Week Physiotherapy & Sports Rehab Protocol
🟡 PRE-OP PREHAB (1–3 Weeks Before Surgery)
- Goals: reduce swelling, restore full ROM, activate quads
- Exercises: quad sets, SLR, heel slides, ankle pumps, stationary cycling
- Neuromuscular activation (VMO, glutes, hamstrings)
🔴 PHASE 1 — Protection & Swelling Control (Weeks 1–2)
Goals: Graft protection, pain/oedema management, prevent muscle atrophy
| Element | Details |
|---|---|
| Weight-bearing | Partial → full WBAT with crutches; wean by end of week 2 |
| Brace | Hinged brace locked at 0° (some protocols omit brace) |
| ROM target | 0–90° |
| Exercises | Quad sets, SLR (4 planes), heel slides, ankle pumps, patellar mobilization |
| Modalities | Ice 20 min q2h, elevation, compression |
| Avoid | OKC knee extension, pivoting, running |
🟠 PHASE 2 — Strength & Proprioception (Weeks 3–6)
Goals: Full ROM, quad activation, basic proprioception
| Element | Details |
|---|---|
| Weight-bearing | Full weight-bearing; wean from crutches |
| ROM target | 0–130° by week 6 |
| CKC Exercises | Mini squats (0–60°), step-ups, leg press (0–60°), wall sits |
| Balance | Single-leg balance, wobble board, BOSU |
| Cardio | Stationary cycling (resistance-free), pool walking |
| Avoid | OKC knee extension especially near full extension (stress concentrates on graft); running |
Closed kinetic chain (CKC) exercises are emphasized — foot planted with compressive loading allows physiologic co-contraction and is safer for the graft than OKC exercises. — Miller's Review of Orthopaedics 9th Ed.
🟡 PHASE 3 — Advanced Strengthening (Weeks 7–12)
Goals: Progressive strength, neuromuscular control, cardiovascular conditioning
| Element | Details |
|---|---|
| Exercises | Lunges, lateral step-downs, single-leg press, Romanian deadlifts (hamstrings) |
| OKC | Leg extension may begin cautiously 50–90° only (not near full extension) |
| Proprioception | Single-leg squats, perturbation training |
| Cardio | Swimming, cycling with resistance |
| Criteria to progress | Single-leg squat ×10 with proper form through 60° flexion; no swelling/instability |
🟢 PHASE 4 — Running & Functional Training (Months 3–5)
Goals: Return to jogging, introduce agility
| Element | Details |
|---|---|
| Running | Criteria-based: start straight-line jogging on flat surfaces when quad index >70% |
| Return-to-run protocol | Walk/jog intervals: start W5/J1×5, progress over 3 weeks to continuous jog |
| Agility intro | Straight-line acceleration/deceleration, side shuffles, backward jogging |
| Plyometrics | Double-leg box jumps, lateral hops over line, small drop jumps |
| Criteria | Quad index >80%; no pain/swelling with loading |
🔵 PHASE 5 — Sport-Specific Training (Months 5–9)
Goals: Plyometrics, sport-specific movement, neuromuscular patterns
| Element | Details |
|---|---|
| Plyometrics | Box jumps with direction change, 90°/180° jump-turns, single-leg hops |
| Agility | Zig-zag runs, T-drill, 5-10-5 shuttle, cross-over drills |
| Sport-specific | Position-specific drills, ball work, reactive movements |
| Blood Flow Restriction (BFR) | Evidence-based adjunct — 2025 meta-analysis (PMID: 38889851) shows BFR enhances quad/hamstring recovery |
| Criteria | Quad/HS/glut index ≥95%; Hamstring:Quad ratio ≥66%; hop testing ≥90% vs. contralateral side |
✅ PHASE 6 — Return to Full Sport (Months 9–12)
Clearance Criteria (all must be met):
| Criterion | Threshold |
|---|---|
| Quad strength index | ≥95% of contralateral leg |
| Hamstring:Quad ratio | ≥66% |
| Single-leg hop test | ≥95% limb symmetry index |
| KOOS-Sports questionnaire | >90% |
| ACL-RSI (psychological readiness) | ≥90 |
| No swelling | Confirmed |
| Full ROM | Confirmed |
Progression: Non-contact practice → Full practice → Full match play
A 2025 systematic review in AJSM (PMID: 38622858) of soccer players found variable return-to-sport timelines and emphasized criterion-based rather than purely time-based clearance.
7. Key Complications to Watch
| Complication | Notes |
|---|---|
| Arthrofibrosis | Most common post-op complication; prevented by achieving full ROM before surgery |
| Graft failure | Usually tunnel malposition (vertical graft = poor rotational stability; anterior femoral tunnel = flexion loss) |
| Infection | Irrigation + débridement with graft retention successful in ~85% |
| Re-rupture | Posterior tibial slope >12° increases graft failure risk; allograft in young athletes carries higher rupture rate |
8. Summary Timeline
Pre-op Prehab → Reduce swelling, restore ROM, activate quads
Weeks 1–2 → Protect graft, pain/oedema control, quad sets
Weeks 3–6 → Full WB, CKC strengthening, proprioception
Weeks 7–12 → Lunges, advanced strengthening, cycling
Months 3–5 → Jogging, early plyometrics, agility
Months 5–9 → Sport-specific drills, cutting, plyometrics
Months 9–12 → Criterion-based return to full sport
Total timeline: 9–12 months for most athletes; up to 24 months for allograft full maturation.
Sources: Miller's Review of Orthopaedics 9th Ed. | Rockwood & Green's Fractures in Adults 10th Ed. | MGH Sports Medicine ACL Protocol (2024) | PMID 38889851 | PMID 38622858
This is a shared conversation. Sign in to Orris to start your own chat.