Anatomy of parotid gland and its applied anatomy. Ms ent university exam pattern for 20 marks.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
I now have all the material needed to write a comprehensive 20-mark MS ENT university exam answer. Let me compile it:
Anatomy of the Parotid Gland and Applied Anatomy
(MS ENT University Exam Pattern - 20 Marks)
INTRODUCTION (1 mark)
The parotid gland is the largest of the three paired major salivary glands. It is a purely serous gland and is unique among salivary glands in containing intraglandular lymph nodes. Its anatomical complexity - particularly its intimate relationship with the facial nerve - makes it clinically and surgically significant.
PART I: ANATOMY OF THE PAROTID GLAND (12 marks)
1. Position and Extent
The parotid gland occupies the parotid region on the lateral face, anterior to and below the lower half of the ear. Its boundaries are:
| Border | Relation |
|---|---|
| Anterior | Masseter muscle (halfway across) |
| Superior | Zygomatic arch |
| Posterior | Tragal cartilage + anterior border of sternocleidomastoid |
| Inferior | Lower border of mandible; inferior tail overlies the digastric muscle between ramus of mandible and SCM |
| Deep | Pretyloid compartment of the parapharyngeal space |
(Gray's Anatomy for Students)
2. Lobes and Fascial Covering
The gland is enclosed in the parotidomasseteric fascia (investing layer of deep cervical fascia), which:
- Attaches superiorly to the root of the zygoma
- Attaches posteriorly to the mastoid process (thick)
- Is thin anteriorly, separating from tragal/conchal cartilage by blunt dissection
- Has a thick inferior portion separating the parotid from the submandibular gland
The gland is divided into superficial and deep lobes by the plane of the facial nerve:
- 80% of parenchyma (and the majority of intraglandular lymph nodes) lie in the superficial lobe
- The deep lobe lies medial to the facial nerve plane and extends into the parapharyngeal space
- This division is primarily a surgical/functional concept, not a true anatomical lobation
(K.J. Lee's Essential Otolaryngology; Cummings Otolaryngology)
3. Parotid Duct (Stensen's Duct)
- Leaves the anterior border of the gland, midway between the zygomatic arch and the corner of the mouth
- Traverses horizontally over the masseter muscle
- At the anterior border of masseter, it turns medially, piercing the buccinator muscle
- Opens into the oral cavity opposite the upper second molar tooth
- An accessory parotid gland may lie along the duct (1% of parotid tumors arise here)
(Gray's Anatomy for Students; K.J. Lee's)
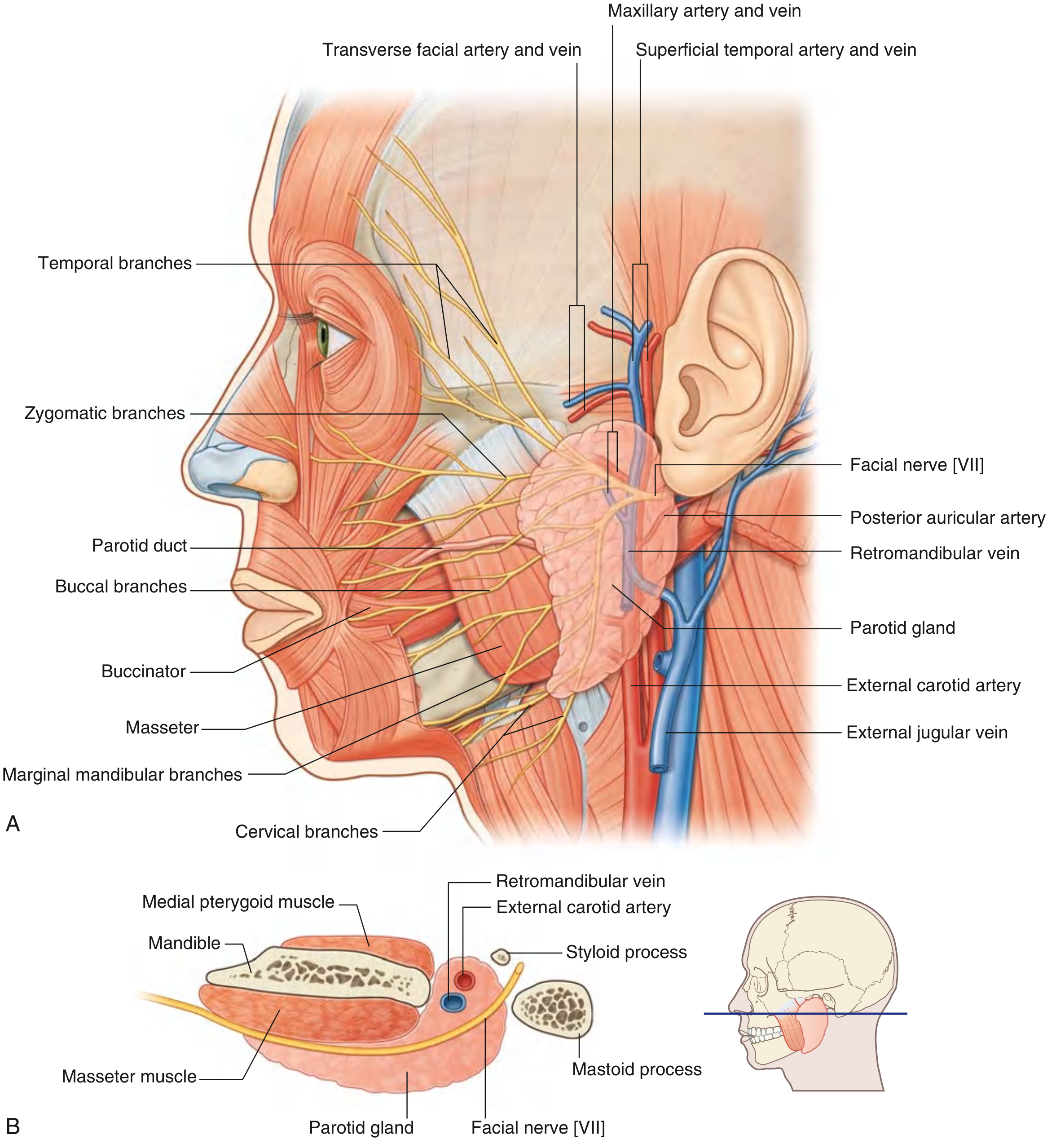
4. Structures Within the Parotid Gland
The following structures are embedded within or pass through the gland (remembered by the mnemonic - from superficial to deep: Facial nerve, Retromandibular vein, External carotid artery):
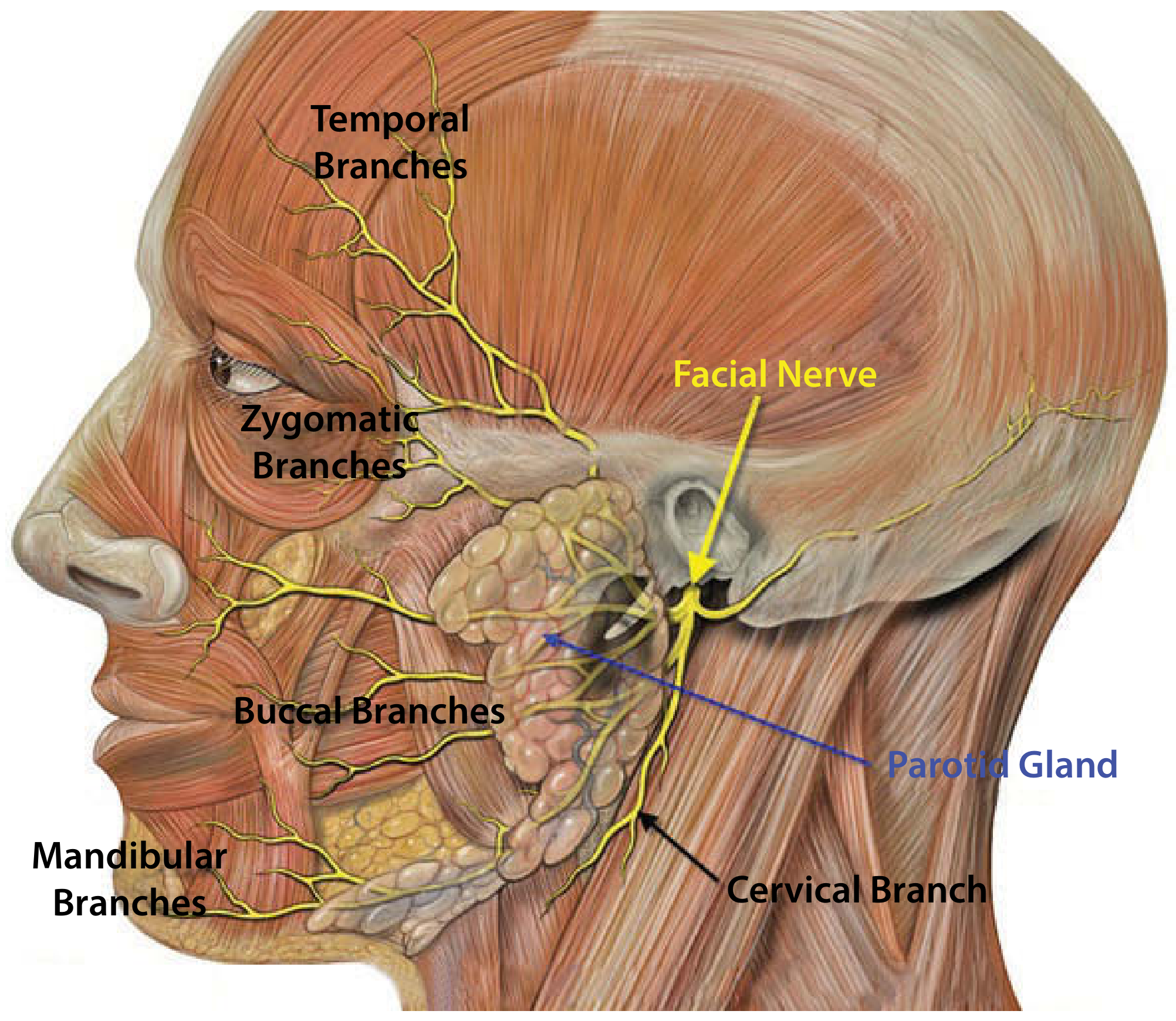
A. Facial Nerve (CN VII)
- Exits the skull base via the stylomastoid foramen (posterolateral to styloid process, anteromedial to mastoid process)
- Enters the posteromedial aspect of the parotid and divides into the pes anserinus (upper temporofacial + lower cervicofacial divisions)
- Five terminal branch groups emerge from the parotid borders:
- Temporal - upper border
- Zygomatic - upper border
- Buccal - anterior border
- Marginal mandibular - inferior border
- Cervical - inferior border
- The facial nerve is more superficial in children under 2 years
B. External Carotid Artery (deepest)
- Courses medial to the parotid, dividing into its two terminal branches:
- Maxillary artery - passes deep to mandible
- Superficial temporal artery - emerges from upper border after giving off the transverse facial artery
- Also gives the posterior auricular artery before dividing
- Frequently encountered during total parotidectomy
C. Retromandibular Vein
- Formed by union of the maxillary + superficial temporal veins within the parotid
- Joins the external jugular vein via the posterior facial vein
- An anterior division joins the internal jugular vein (lies just deep to the marginal mandibular branch)
(Gray's Anatomy for Students; K.J. Lee's Essential Otolaryngology)
5. Nerve Supply
| Type | Nerve | Pathway |
|---|---|---|
| Parasympathetic (secretomotor) | CN IX (Glossopharyngeal) via the lesser petrosal nerve → otic ganglion → auriculotemporal nerve | Preganglionic fibers from inferior salivatory nucleus → tympanic nerve → tympanic plexus → lesser petrosal nerve → otic ganglion → postganglionic fibers join auriculotemporal nerve |
| Sympathetic (vasoconstriction) | Superior cervical ganglion | Postganglionic fibers travel along external carotid artery branches |
| Sensory | Great auricular nerve (C2, C3) + Auriculotemporal nerve (V3) | Great auricular divides into anterior and posterior branches |
6. Lymphatic Drainage
The parotid is unique in having intraglandular (preauricular) lymph nodes - predominantly in the superficial lobe. Drainage follows:
- Intraglandular nodes → Parotid nodes (superficial and deep) → Upper deep cervical nodes (Level II)
7. Histology
Pure serous acini with serous demilunes. Striated ducts are prominent (for fluid reabsorption). The gland produces about 25% of total daily saliva (predominantly watery, enzyme-rich).
PART II: APPLIED ANATOMY (8 marks)
1. Parotidectomy and the Facial Nerve
The intimate relationship of CN VII with the parotid gland makes parotid surgery technically demanding. Surgical landmarks used to identify the facial nerve trunk:
- Tragal pointer - the nerve lies 1 cm deep and inferior to the tip of the tragal cartilage
- Tympanomastoid suture line - nerve lies ~6-8 mm deep at this point
- Posterior belly of digastric - marks the depth of the nerve
- Retrograde dissection - tracing a peripheral branch back to the trunk
Types of parotidectomy:
- Superficial parotidectomy - for most benign tumors (80-90% of tumors are in superficial lobe)
- Total conservative parotidectomy - for deep lobe tumors, with facial nerve preservation
- Radical parotidectomy - for malignancy invading the nerve
Complications:
- Temporary/permanent facial palsy: Neuropraxia usually resolves in 4-6 weeks; permanent palsy risk ~1-2%
- Sensory loss: In distribution of great auricular nerve (angle of mandible, lower 2/3 of pinna) - unavoidable
- Frey's syndrome (gustatory sweating)
- Cosmetic defect - hollowing behind the mandible
(Scott-Brown's Otorhinolaryngology)
2. Frey's Syndrome (Auriculotemporal Syndrome)
- Most disturbing late complication after parotidectomy
- Mechanism: Aberrant reinnervation - divided parasympathetic secretomotor fibers (from auriculotemporal nerve destined for parotid) regenerate along the divided sympathetic fibers that supply sweat glands of the overlying skin
- Result: Stimulation of salivation during eating triggers gustatory sweating and flushing in the pre-auricular skin
- Prevention: Interposing a fascial/SMAS flap between the parotid bed and skin
- Treatment: Intradermal botulinum toxin injection (most effective)
(Scott-Brown's; Goldman-Cecil Medicine; Bailey & Love)
3. Deep Lobe Tumors and Parapharyngeal Extension
The deep lobe extends into the pretyloid compartment of the parapharyngeal space. Deep lobe tumors may present as:
- Soft palate/lateral oropharyngeal swelling ("dumbbell tumor") with little external swelling
- The parapharyngeal space is an inverted pyramid: base at petrous bone, medial wall = lateral pharyngeal wall, lateral wall = medial pterygoid, posterior = carotid sheath
(K.J. Lee's Essential Otolaryngology; Cummings Otolaryngology)
4. Parotid Swellings - Clinical Significance
Because 80-90% of parotid tissue is superficial, a similar proportion of tumors arise there. Key clinical points:
| Feature | Suggests Benign | Suggests Malignant |
|---|---|---|
| Growth | Slow, years | Rapid |
| Pain | Absent | Present (44% of malignant cases) |
| Facial nerve | Intact | Paresis/paralysis (25% of malignant cases) |
| Mobility | Mobile | Fixed to skin/deep structures |
| Nodes | Absent | Cervical lymphadenopathy |
Most common benign tumor: Pleomorphic adenoma
Most common malignant: Mucoepidermoid carcinoma
(Cummings Otolaryngology; Scott-Brown's)
5. Parotid and Facial Palsy
- Parotid carcinoma accounts for up to 6% of cases of lower motor neuron facial palsy when no cause is found on initial MRI
- Suspect malignancy if: slow onset, progressive, no recovery, isolated branch involvement, facial tics
6. Parotid Lymph Nodes - Clinical Importance
- The parotid is the only salivary gland with intraglandular lymph nodes
- These drain the scalp, pinna, external auditory canal, middle ear, eyelids, and lacrimal gland
- Clinically: metastatic disease from skin malignancies (melanoma, SCC of scalp/ear) can present as a parotid mass
- Lymphoma can also involve these nodes
7. Stensen's Duct - Applied
- Injury to the duct during facial trauma or surgery can cause a salivary fistula or parotid pseudocyst
- The duct runs along a line from the tragus to the midpoint of the upper lip - used surgically
- Calculi in Stensen's duct present as painful swelling on eating (mealtime syndrome)
8. Accessory Parotid Gland
- Lies along Stensen's duct on the masseter surface
- Site of 1% of parotid tumors - presents as a cheek mass rather than pre-auricular swelling
SUMMARY TABLE FOR QUICK REVISION
| Feature | Detail |
|---|---|
| Type | Serous gland |
| Largest salivary gland | Yes |
| Unique feature | Contains intraglandular lymph nodes |
| Duct opening | Opposite upper 2nd molar |
| Key nerve traversing it | Facial nerve (CN VII) |
| Lobe division | By facial nerve plane; 80% is superficial |
| Parasympathetic supply | CN IX → lesser petrosal → otic ganglion → auriculotemporal |
| Most common benign tumor | Pleomorphic adenoma |
| Most common malignant | Mucoepidermoid carcinoma |
| Post-parotidectomy complication | Frey's syndrome (auriculotemporal nerve misdirection) |
Sources: K.J. Lee's Essential Otolaryngology, 11th ed. | Gray's Anatomy for Students, 4th ed. | Scott-Brown's Otorhinolaryngology Head & Neck Surgery | Cummings Otolaryngology Head & Neck Surgery, 7th ed. | Bailey & Love's Short Practice of Surgery, 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.