Elbow dislocation types mechanism of injury associated injury methods to reduce signs and symptoms investigation and treatment explain in detail with appropriate illustrative diagrams and images
Reading File
Finding Sources
Searching the Web
elbow dislocation types mechanism associated injuries reduction techniques management
Searching PubMed
"elbow dislocation"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks (Tintinalli's Emergency Medicine, Rockwood & Green's Fractures in Adults 2025, Roberts & Hedges, Campbell's Operative Orthopaedics, Pye's Surgical Handicraft) plus excellent images. Let me compose the full detailed answer.
Elbow Dislocation: A Comprehensive Review
1. Anatomy and Stability
The elbow is one of the most stable joints in the body, relying on three interconnected articulations: humeroulnar, humeroradial, and proximal radioulnar. Stability is provided by:
- Bony anatomy: the hinge-like trochlear notch of the ulna wrapping around the trochlea
- Medial (ulnar) collateral ligament (MCL): primary restraint to valgus stress
- Lateral collateral ligament complex (LCL): primary restraint to varus/rotatory stress
- Capsule, flexor/extensor muscle origins
Despite this stability, elbow dislocations rank third among large-joint dislocations, after the glenohumeral and patellofemoral joints, with an incidence of ~5.2 per 100,000 person-years.
2. Classification / Types
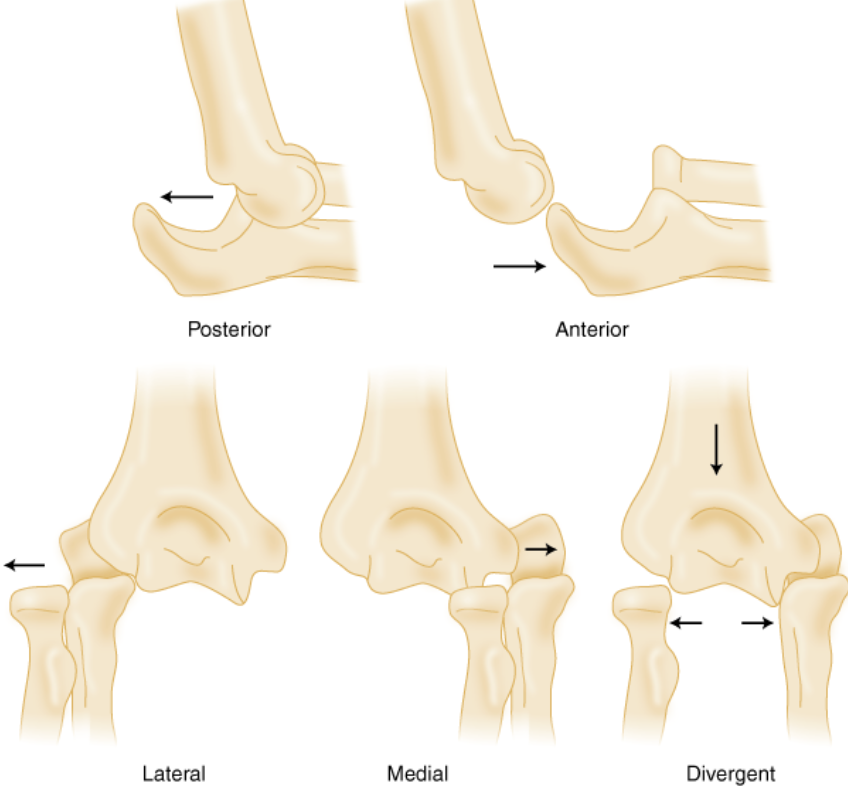
Elbow dislocations are classified by the direction of forearm displacement relative to the humerus:
| Type | Frequency | Description |
|---|---|---|
| Posterior / Posterolateral | ~90% | Radius & ulna displace posteriorly; most common |
| Posterior-medial | Uncommon | Associated with anteromedial coronoid fracture |
| Anterior | Rare | Forearm displaced anterior to humerus |
| Lateral | Rare | Forearm displaces laterally |
| Medial | Rare | Forearm displaces medially |
| Divergent | Very rare | Radius and ulna separate - disruption of proximal radioulnar joint |
Simple vs. Complex
- Simple: No associated fractures (ligamentous injuries only)
- Complex: Associated fractures (radial head, coronoid, olecranon). The "Terrible Triad" - elbow dislocation + radial head fracture + coronoid fracture - is the most unstable combination and requires emergent orthopaedic consultation.
3. Mechanism of Injury
The classic mechanism is a fall on an outstretched hand (FOOSH) with the elbow in extension or slight flexion. The typical force combination described by O'Driscoll is:
Valgus + Axial compression + Supination/Posterolateral rotation
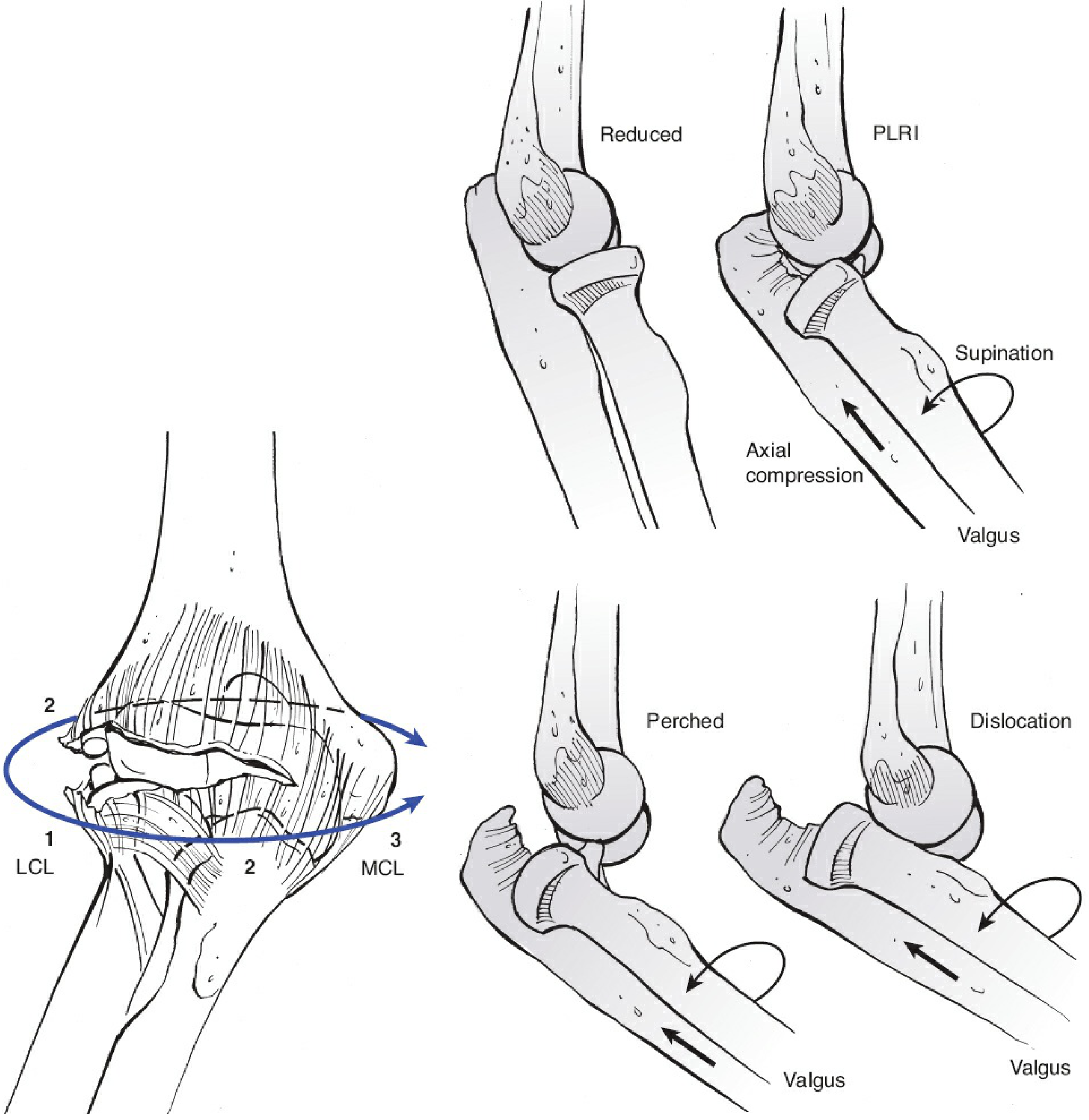
Figure: O'Driscoll's circle of soft tissue disruption. Injury begins at the LCL (1), proceeds through the posterior and anterior capsule (2), and can extend to the MCL (3). The stages are: Reduced → PLRI (posterolateral rotatory instability) → Perched → Full dislocation.
Sequence of soft tissue failure:
- LCL complex tears first (lateral side)
- Posterior and anterior capsule disrupts
- MCL may tear last (or remain intact in some cases)
Note: More recent MRI/video studies have challenged the classic lateral-first model, showing that medial ligament tears may sometimes predominate, explaining why some elbows are highly stable after reduction when the LCL is preserved.
Other mechanisms:
- Direct blow to the flexed elbow (posterior dislocation)
- High-energy trauma (MVA, sports contact) - associated with complex fracture-dislocations
- "Side-swipe" injury: violent blow to an elbow protruding from a vehicle window - typically causes fracture-dislocation with comminution
Epidemiology:
- Nearly 50% occur in sports (males in football; females in gymnastics and skating)
- Adolescent males are the highest-risk group
- ~5.2 per 100,000 person-years in the US
4. Signs and Symptoms
History:
- FOOSH or direct trauma
- Immediate pain and inability to move elbow
- Some patients self-reduce (then present with pain, swelling, ecchymosis only)
Examination findings:
Posterior dislocation (most common):
- Elbow held in ~45° of flexion - the patient refuses to extend
- Prominent olecranon posteriorly - "step deformity"
- Fullness in the antecubital fossa (displaced coronoid process)
- Disruption of the equilateral triangle formed by the olecranon and both epicondyles (normally equilateral in flexion - disturbed in dislocation, intact in supracondylar fracture)
- Marked swelling and ecchymosis - may obscure bony landmarks if seen late
- Restricted and painful ROM in all directions
Neurovascular assessment (mandatory before and after reduction):
| Structure | Finding to check |
|---|---|
| Ulnar nerve (most common, up to 20%) | Sensation little finger, intrinsic weakness |
| Median nerve | Sensation index fingertip, wrist flexion |
| Brachial artery (5-13% of cases) | Radial pulse, capillary refill |
| Anterior interosseous nerve | Thumb and index FDP (OK sign) |
Red flags for arterial injury: absent radial pulse before reduction, open dislocation, systemic injuries.
5. Investigations
Plain Radiography (first-line)
AP and lateral elbow X-rays are mandatory:

Figure: Posterior elbow dislocation on X-ray. Lateral view (left) shows radius and ulna displaced posteriorly relative to the distal humerus. AP view (right) shows the medial or lateral displacement component.
- Lateral view: Both radius and ulna displaced posteriorly
- AP view: May show medial or lateral displacement; ulna and radius maintain their normal relationship to each other
- Assess for coronoid process fracture, radial head fracture, medial epicondyle avulsion
Post-reduction X-rays:
- Confirm concentric reduction of ulnohumeral joint
- If concentric reduction is unclear, CT scan is required
Advanced imaging:
| Modality | Indication |
|---|---|
| CT scan | Confirm concentric reduction; characterise fracture patterns; CT angiography if vascular injury suspected |
| MRI | Assess ligamentous injury extent (MCL, LCL); plan operative treatment |
| Ultrasound/Angiography | Suspected brachial artery injury |
6. Methods of Reduction
Principles:
- Adequate analgesia/sedation is essential before any attempt
- Options: IV analgesia, intra-articular lidocaine (helpful and often underused), procedural sedation, or general anaesthesia for resistant cases
- Two providers are usually needed; single-person techniques exist
Posterior Dislocation Reduction Methods
Method 1: Prone Hanging Arm Technique (Recommended first)
Patient prone, affected arm hanging over edge of bed with elbow flexed 90°. Assistant grasps humerus with both hands, applies thumbs to posterior olecranon. Apply longitudinal traction distally (white arrow). If resistance, further flex elbow or lift humerus. Reduction confirmed by a definitive "clunk."
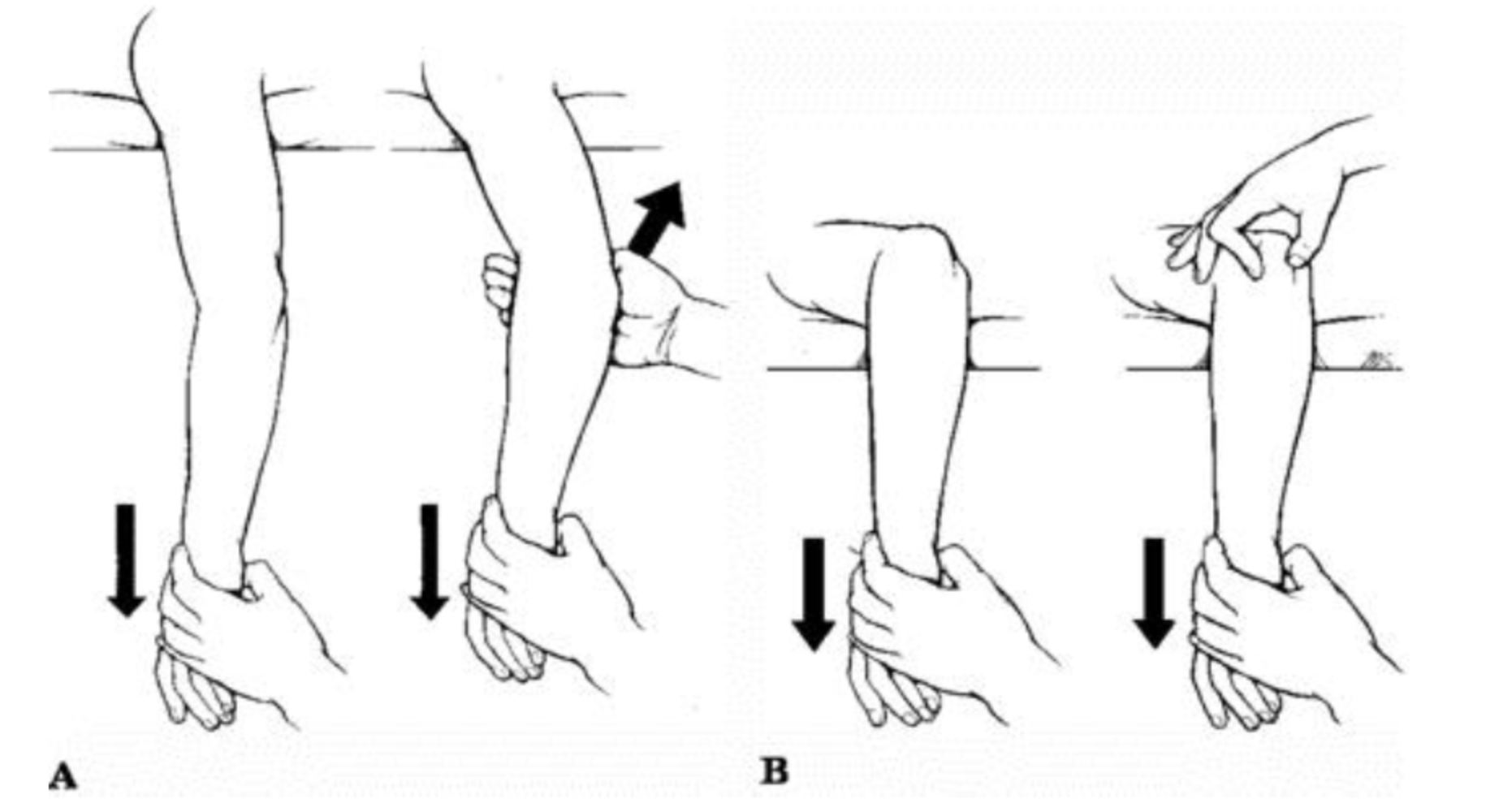
Figure: (A) Two-person prone technique - downward traction at wrist, upward pressure on olecranon. (B) Single-person variant.
Method 2: Supine Traction-Countertraction
Patient supine. Assistant stabilizes humerus at proximal arm. Clinician:
- Grasps wrist, applies slow steady in-line longitudinal traction
- Slightly flexes the elbow (to relax triceps)
- Holds wrist supinated
- If unsuccessful, applies downward pressure on proximal volar surface of forearm to free the coronoid process, then flexes elbow
Method 3: Chair/Back of Bed (Stimson-type)
Arm hung over padded back of chair or bed edge. Gravity provides traction. Apply posterior pressure on olecranon to guide reduction. Takes 1-10 minutes.
Method 4: Single-Person "Leverage" Technique
Clinician places their own elbow into patient's antecubital fossa, grasps patient's hand/wrist, flexes patient's forearm using leverage force into the antecubital fossa to push coronoid back into joint.
Technique to correct medial/lateral displacement:
Before applying traction/flexion, manually correct any side-to-side displacement.
Anterior Dislocation Reduction
Requires multiple providers. One applies inline traction to disengage the olecranon from anterior humerus; the second applies posterior traction to the proximal forearm to guide the olecranon posteriorly back into place.
Post-Reduction Assessment (critical):
- Confirm reduction by palpating the equilateral triangle and checking X-ray
- Stability testing: Varus and valgus stress at 20° of flexion with humerus externally rotated
- Valgus laxity = MCL injury → splint in supination
- Varus laxity = LCL injury → splint in pronation
- Neurovascular recheck - repeat pulse and nerve exam
- Check for entrapped medial epicondyle fracture on post-reduction X-ray
7. Treatment
Management Algorithm
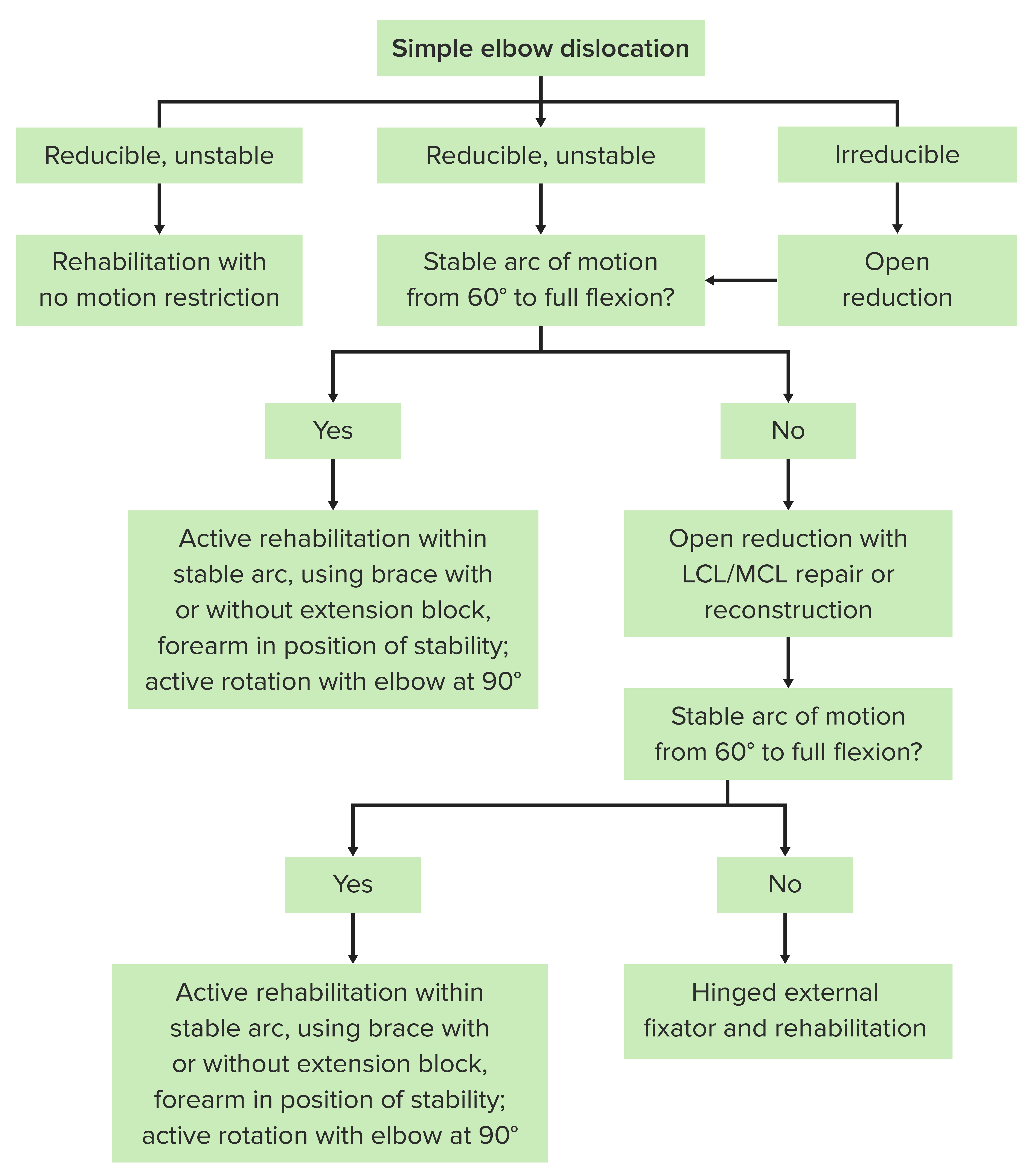
Figure: Simple elbow dislocation management algorithm based on stability after reduction.
Non-Operative (Simple Dislocations)
Immediate:
- Closed reduction as above
- Posterior long arm backslab/splint at ~90° flexion for 1-3 weeks (avoid prolonged immobilisation >3 weeks - stiffness risk)
- Ice, elevation
Immobilisation position:
- Elbow at 90° flexion
- Supination if MCL disruption (valgus instability)
- Pronation if LCL disruption (varus instability)
Rehabilitation (early mobilisation preferred):
- Active ROM exercises within a stable arc (typically 60° to full flexion)
- Brace with extension block if needed
- Active forearm rotation with elbow at 90°
- Physiotherapy is recommended; stiffness (especially loss of terminal extension) is the most common long-term complaint
Discharge and follow-up:
- Observe for 2-3 hours post-reduction for vascular compromise
- Orthopaedic follow-up within 24-48 hours
- Adequate analgesia, ice, elevation instructions
Operative Treatment
Indications:
- Irreducible dislocation (interposed tissue/entrapped fragment)
- Open dislocation (requires debridement + ORIF)
- Associated fracture with instability (radial head, coronoid - complex/terrible triad)
- Persistent instability after closed reduction
- Vascular injury (brachial artery - needs vascular repair)
- Entrapped medial epicondyle in joint
Operative options:
| Procedure | Indication |
|---|---|
| Open reduction | Irreducible, soft tissue interposition |
| ORIF of radial head/coronoid | Associated fractures causing instability |
| LCL/MCL repair or reconstruction | Persistent instability after reduction |
| Hinged external fixator | Unstable after ligament repair; protects vascular repair |
| Internal joint stabilizer | Compliance issues or severe instability |
| Cross-pinning | Selected complex cases |
For ORIF, the patient is positioned supine with arm table, fluoroscopy from the head, and equipment including suture anchors, heavy non-absorbable suture, and large fragment locking set.
8. Complications
| Complication | Notes |
|---|---|
| Elbow stiffness / loss of extension | Most common; up to 15° extension loss is common; worse with prolonged immobilisation |
| Ulnar nerve palsy | Up to 20% incidence; most recover post-reduction |
| Median nerve injury | Less common; median nerve entrapment in joint post-reduction is a specific risk |
| Brachial artery injury | 5-13%; absent radial pulse is a red flag; angiography/vascular repair required |
| Recurrent instability | <10% of simple dislocations; more common with extensive MCL+LCL injury |
| Myositis ossificans | Heterotopic ossification around elbow, often following delayed treatment or forceful manipulation |
| Avascular necrosis | Rare |
| Post-traumatic arthritis | Long-term, especially after complex fracture-dislocation |
9. Special Variants
Terrible Triad of the Elbow
- Elbow dislocation + radial head fracture + coronoid fracture
- Highly unstable; requires operative stabilisation (ORIF of coronoid and radial head + LCL repair)
- MCL repair added if still unstable
- High complication rate
Monteggia Fracture-Dislocation
- Proximal ulna fracture + radial head dislocation
- Peak in children aged 4-10 years
- Radial nerve injury in 10-20% (especially anterior/lateral dislocations)
- A line through the radial neck should always pass through the capitellum (Radiocapitellar line) - loss of this relationship is diagnostic
Divergent Dislocation
- Very rare; radius and ulna separate (disruption of proximal radioulnar joint)
- Results from severe axial force driving the humerus between the two bones
- Generally requires open reduction
10. Key Clinical Pearls
- Elbow dislocation vs. supracondylar fracture: Palpate the equilateral triangle (olecranon + two epicondyles) - intact in supracondylar fractures, disrupted in dislocation
- Always check neurovascular status before AND after reduction - median nerve can become entrapped post-reduction
- Always check post-reduction X-ray for concentric joint reduction and for a trapped medial epicondyle fragment
- Intra-articular lidocaine is an underused but effective adjunct for procedural pain management
- Early mobilisation gives better outcomes than prolonged casting - immobilise for maximum 3 weeks
- 98.5% of dislocations are posterior - anterior reduction techniques are rarely needed
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide (9th ed.)
- Rockwood and Green's Fractures in Adults (10th ed., 2025)
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
- Campbell's Operative Orthopaedics (15th ed., 2026)
- Pye's Surgical Handicraft (22nd ed.)
- StatPearls: Posterior Elbow Dislocation | LITFL Elbow Dislocation
This is a shared conversation. Sign in to Orris to start your own chat.