Hernia repair
Reading File
Finding Sources
Searching PubMed
"hernia repair"[MeSH Terms] AND "mesh"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to write a thorough response. Let me compile everything.
Hernia Repair - Comprehensive Overview
Anatomy of the Inguinal Region
Understanding the anatomy is the foundation of any hernia repair:
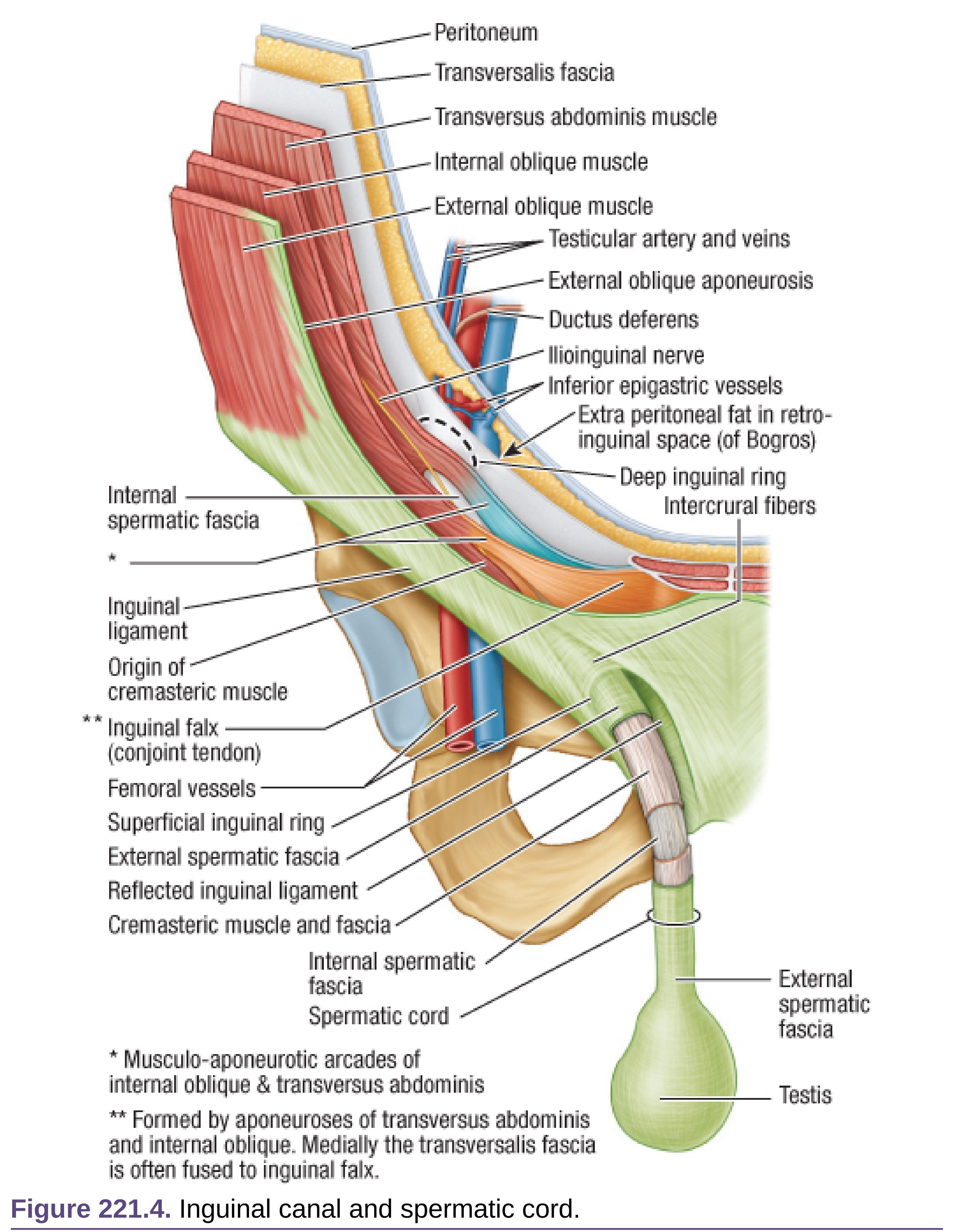
Hesselbach's (inguinal) triangle is the key anatomical landmark, bounded by:
- Lateral border of the rectus sheath (medially)
- Inferior epigastric vessels (superolaterally)
- Inguinal ligament (inferiorly)
The transversus abdominis and transversalis fascia normally prevent inguinal and femoral hernias - variations or defects in these layers allow groin hernias to occur. - Fischer's Mastery of Surgery, 8th ed.
Types of Inguinal Hernia
| Type | Location | Key Feature |
|---|---|---|
| Direct | Medial to inferior epigastric vessels - through Hesselbach's triangle | Covered by attenuated transversalis fascia; lies adjacent to but outside the spermatic cord |
| Indirect | Lateral to inferior epigastric vessels - through the deep inguinal ring | Follows the route of testicular descent; hernia sac becomes part of the spermatic cord |
| Femoral | Inferior to the inguinal ligament - through the femoral canal | Higher risk of strangulation |
Indirect hernias represent persistence of a patent processus vaginalis. In children, 99% of inguinal hernias are congenital indirect; direct and femoral types are rare. - Fischer's Mastery of Surgery, Mulholland & Greenfield's Surgery
Surgical Options for Inguinal Hernia Repair
Summary of Operations
(Bailey & Love's Surgery, 28th ed.)
Herniotomy - sac ligation only (used in children)
Open suture repairs (tissue repairs):
- Bassini
- Shouldice
- Desarda
- Maloney darn
Open flat mesh repair:
- Lichtenstein - the standard tension-free open mesh repair
Open preperitoneal repair:
- Stoppa repair
Laparoscopic/robot-assisted:
- TEP (Totally Extraperitoneal)
- TAPP (Transabdominal Preperitoneal)
Open Repair (Lichtenstein Technique)
The open repair involves an incision over the inguinal canal, incising Scarpa's fascia and the external oblique aponeurosis to expose the inguinal canal. The cremaster is opened to identify and mobilise the sac from the testicular vessels and vas deferens. The sac is divided, twisted to reduce any contents, and transfixed/ligated at the internal ring. A flat mesh is placed in a tension-free fashion over the posterior wall of the inguinal canal and fixed to the inguinal ligament and conjoint tendon. - Bailey & Love's Surgery, 28th ed.
Laparoscopic Repair (TEP and TAPP)
Both techniques aim to reduce the hernia sac from within and place a 10 x 15 cm mesh (or larger) in the preperitoneal plane, covering:
- Hesselbach's triangle
- The deep inguinal ring
- The femoral canal
TEP: Surgeon develops the extraperitoneal plane directly, without entering the peritoneal cavity.
TAPP: Surgeon enters the peritoneal cavity first, then incises the peritoneum above the defect to access the extraperitoneal space.
Advantages of laparoscopic over open approach:
- Reduced pain - both immediately and up to 5 years postoperatively
- Faster return to full activity
- Fewer wound complications (infection, bleeding, seroma)
- Particular benefit for bilateral hernias and recurrent hernias after open surgery
- Chronic pain is less common and less severe
The increasing use of robot-assisted laparoscopic repair is evident, though little additional patient benefit has been demonstrated. The cost of using a robot for simple inguinal repair remains hard to justify. - Bailey & Love's Surgery, 28th ed.
Mesh in Hernia Repair
Mesh (prosthetic material as a net or flat sheet) can be used to:
- Bridge a defect - fixed over the defect as a tension-free patch (requires generous overlap onto strong tissue)
- Plug a defect - a plug of mesh pushed into the defect (largely abandoned due to "meshoma" formation causing chronic pain, migration, and fistula)
- Augment a repair - defect closed with sutures, mesh added for reinforcement
Current standard: Primary closure of the defect with mesh reinforcement placed tension-free is optimal. Inlay mesh (sutured edge-to-edge with no overlap) is NOT recommended. - Bailey & Love's Surgery, 28th ed.
Mesh Materials
| Material | Properties |
|---|---|
| Polypropylene | Inert, hydrophobic monofilament; resists bacterial ingrowth; most commonly used |
| Polyester | Hydrophilic; encourages microvascular ingrowth |
| PTFE | Flat sheet; highly inert; resistant to both tissue ingrowth and adhesion formation |
Net meshes allow tissue ingrowth between strands and become integrated into host tissue within months. In extraperitoneal inguinal repair, mesh fixation may not be required at all. - Bailey & Love's Surgery, 28th ed.
Emergency Hernia Surgery
About 5% of inguinal hernias present as an irreducible, painful lump that may progress to strangulation and bowel infarction. Key points:
- ~20% of emergency cases require bowel resection
- Bowel resection may require conversion to midline laparotomy, significantly increasing morbidity and mortality
- Synthetic mesh is acceptable even in emergency cases as long as appropriate antibiotic cover is given (unless significant infection/contamination is present)
Complications
Early
- Bleeding / haematoma (subcutaneous vessels; rarely inferior epigastric or iliac vessels)
- Urinary retention
- Femoral nerve blockade (from local anaesthetic infiltration - resolves over hours)
Medium-term (within the first week)
- Pain, bruising, swelling
- Seroma formation (inflammatory response to dissection, sutures, or mesh; more common if peritoneal sac left in situ; usually resolves spontaneously)
- Wound infection
Late
- Hernia recurrence - good centres aim for <5% at 5 years. Mesh repairs have lower recurrence than suture repairs. Tension on the repair is the primary driver of recurrence
- Chronic pain (>3 months) - possibly affects up to 20% of patients after groin hernia repair. Neuralgic pain from nerve irritation is the most severe type. Risk factors include: female sex, young age, painful hernia, pre-existing chronic pain syndrome
- Testicular atrophy - damage to testicular artery can lead to testicular infarction (most serious complication in young men)
Key principle: there is very strong evidence that specialist hernia surgeons have lower recurrence and chronic pain rates regardless of technique used. - Bailey & Love's Surgery, 28th ed.; Maingot's Abdominal Operations
Tailored Approach
No single operation suits all hernias. The choice depends on:
- Surgeon's skills and equipment available
- Patient factors (age, BMI, fitness, comorbidities, bilateral vs. unilateral)
- Hernia characteristics (size, reducibility, recurrent vs. primary)
- Whether no operation at all is the best management (e.g., asymptomatic hernia in elderly high-risk patients)
Laparoscopic repair is preferred for: bilateral hernias, recurrent hernias after prior open repair, patients who require early return to activity.
Open Lichtenstein remains the gold standard open approach for primary unilateral inguinal hernia when laparoscopic expertise is unavailable.
Sources: Bailey & Love's Short Practice of Surgery 28th Ed. | Fischer's Mastery of Surgery 8th Ed. | Maingot's Abdominal Operations | Mulholland & Greenfield's Surgery 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.