Difference between organo axial and mesentero axial volvulus
Reading File
Finding Sources
Finding Sources
Searching the Web
organoaxial vs mesenteroaxial volvulus difference stomach
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough comparison of the two types of gastric volvulus.
Organoaxial vs. Mesenteroaxial Gastric Volvulus
Gastric volvulus is an abnormal rotation of the stomach >180° on its own axis, first described by Berti in 1866. Singleton's classification (the most widely used) divides it into three types based on the axis of rotation: organoaxial (Type I), mesenteroaxial (Type II), and combined/unclassified (Type III).
Schematic Diagrams
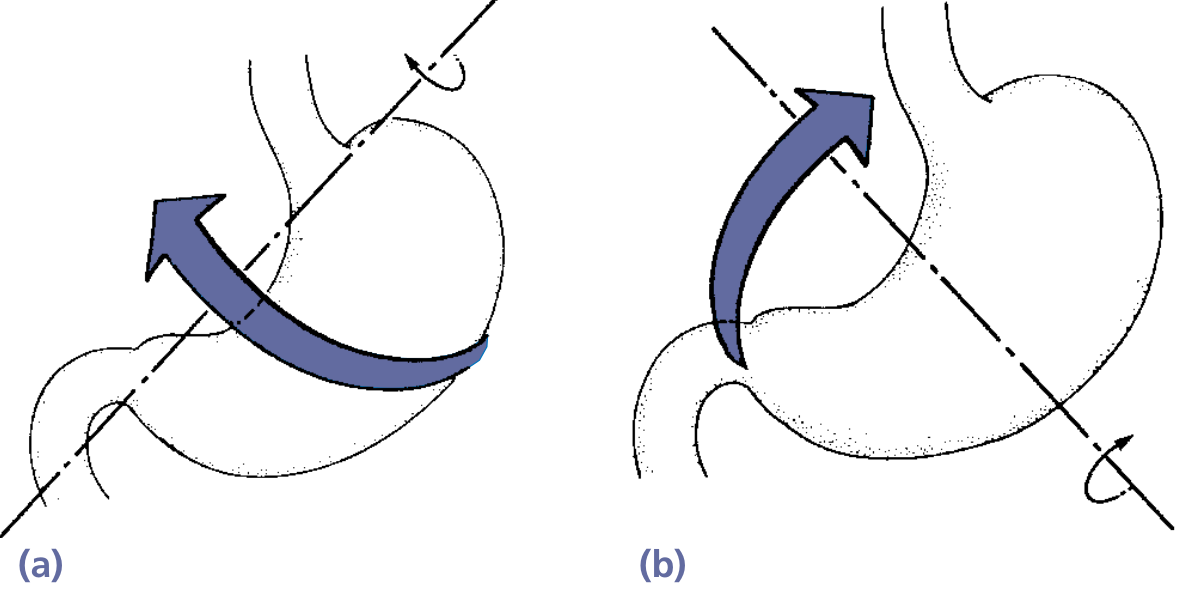
Fig. 53.8 - (a) Organoaxial, (b) Mesenteroaxial volvulus (Yamada's Textbook of Gastroenterology)
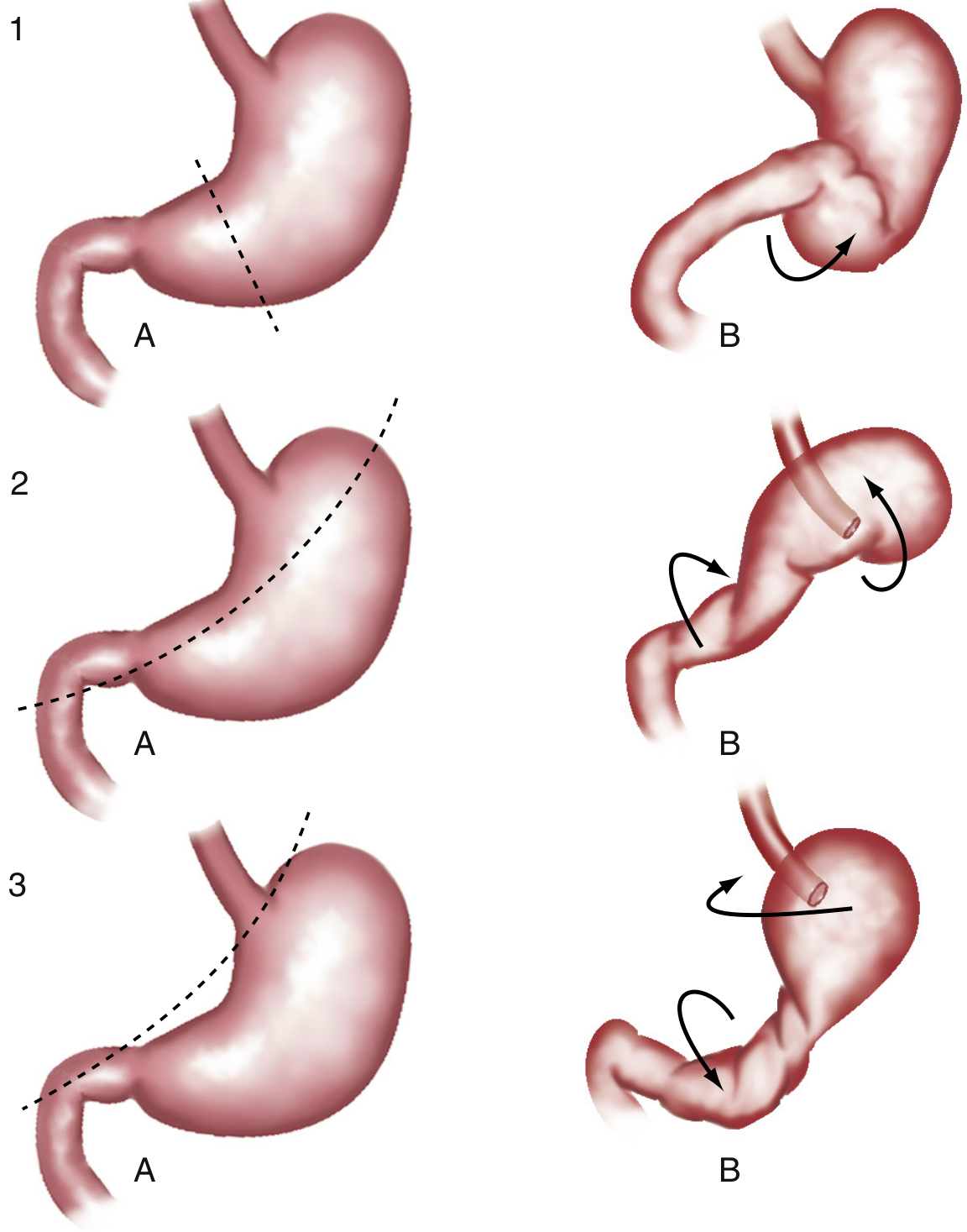
Fig. 27.5 - Pathogenesis of gastric volvulus: rows 1 = mesenteroaxial; rows 2-3 = organoaxial variants (Sleisenger & Fordtran's GI and Liver Disease)
Side-by-Side Comparison
| Feature | Organoaxial (Type I) | Mesenteroaxial (Type II) |
|---|---|---|
| Frequency | ~59-67% of cases (most common) | ~29-33% of cases |
| Axis of rotation | Long axis of stomach (longitudinal axis from GEJ to pylorus) | Short axis (transverse axis bisecting lesser and greater curvatures) |
| Direction of rotation | Stomach rotates along its length - antrum rotates anteriorly/superiorly, fundus posteriorly/inferiorly | Stomach folds on itself - antrum rotates anteriorly and superiorly; posterior surface faces anteriorly |
| GEJ and pylorus position | Both remain in their normal anatomical positions (not in close proximity to each other) | GEJ and pyloric/gastroduodenal junction come close together - "upside-down stomach" |
| Completeness | Usually complete (>180° twist) | Usually incomplete and intermittent |
| Presentation | Typically acute | Typically chronic/recurrent |
| Borchardt's triad | Classic - severe epigastric pain, retching without vomiting, inability to pass NG tube (occurs in ~70% of acute cases) | Less classical - NG tube passes more easily (lower esophageal sphincter remains open) |
| Vascular compromise/ischemia | High risk - strangulation and necrosis reported in 5-28% of cases | Uncommon - because rotation is usually incomplete |
| Obstruction type | Closed-loop obstruction | Obstruction less complete |
| Associated pathology | Strongly associated with paraesophageal/diaphragmatic hernia and diaphragmatic defects | Less associated with diaphragmatic defects; may occur without them |
| Radiologic appearance | Greater curvature displaced superiorly; lesser curvature more caudal | "Upside-down stomach" - distal antrum/pylorus positioned cranially to fundus (horizontal flip) |
| Surgical urgency | Usually emergency surgery required | May be managed on a non-emergency basis |
Key Points to Remember
Organoaxial - think "spinning a rolling pin" - the long axis is the pivot. The antrum and fundus rotate in opposite directions, creating a tight closed-loop. This is the dangerous type with high risk of ischemia and necrosis.
Mesenteroaxial - think "flipping a pancake" - the stomach folds over its midpoint. Because it's usually incomplete and intermittent, it tends to cause recurrent subacute symptoms rather than a surgical emergency.
Borchardt's triad (acute epigastric pain + retching without vomiting + inability to pass NG tube) is most characteristic of organoaxial volvulus. In mesenteroaxial, the NG tube passes relatively easily because the GEJ is not obstructed.
Combined type (Type III) - the stomach twists along both axes simultaneously; accounts for about 12% of cases and is most often seen in chronic volvulus.
Sources: Yamada's Textbook of Gastroenterology 7th ed., p. 1127-1128 | Sleisenger & Fordtran's GI and Liver Disease, p. 407 | Grainger & Allison's Diagnostic Radiology, p. 513 | Rosen's Emergency Medicine | Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.