Viva questions regarding laryngoscope with answers
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks to compile detailed viva questions and answers on the laryngoscope. Let me present the full response.
Viva Questions on the Laryngoscope - With Answers

Q1. What is a laryngoscope? What are its basic components?
A: A laryngoscope is a handheld instrument used to examine the larynx and facilitate intubation of the trachea. Its basic components are:
- Handle - contains batteries for the light source; held in the left hand
- Blade - the working part inserted into the mouth; attached to the handle
- Bulb - at the tip of the blade (or illuminates a fiberoptic bundle)
- Flange - on the left side of the blade, used to retract the tongue laterally
- Electrical contact - connects handle to blade to complete the circuit
(Morgan & Mikhail's Clinical Anesthesiology, 7e; Miller's Anesthesia, 10e)
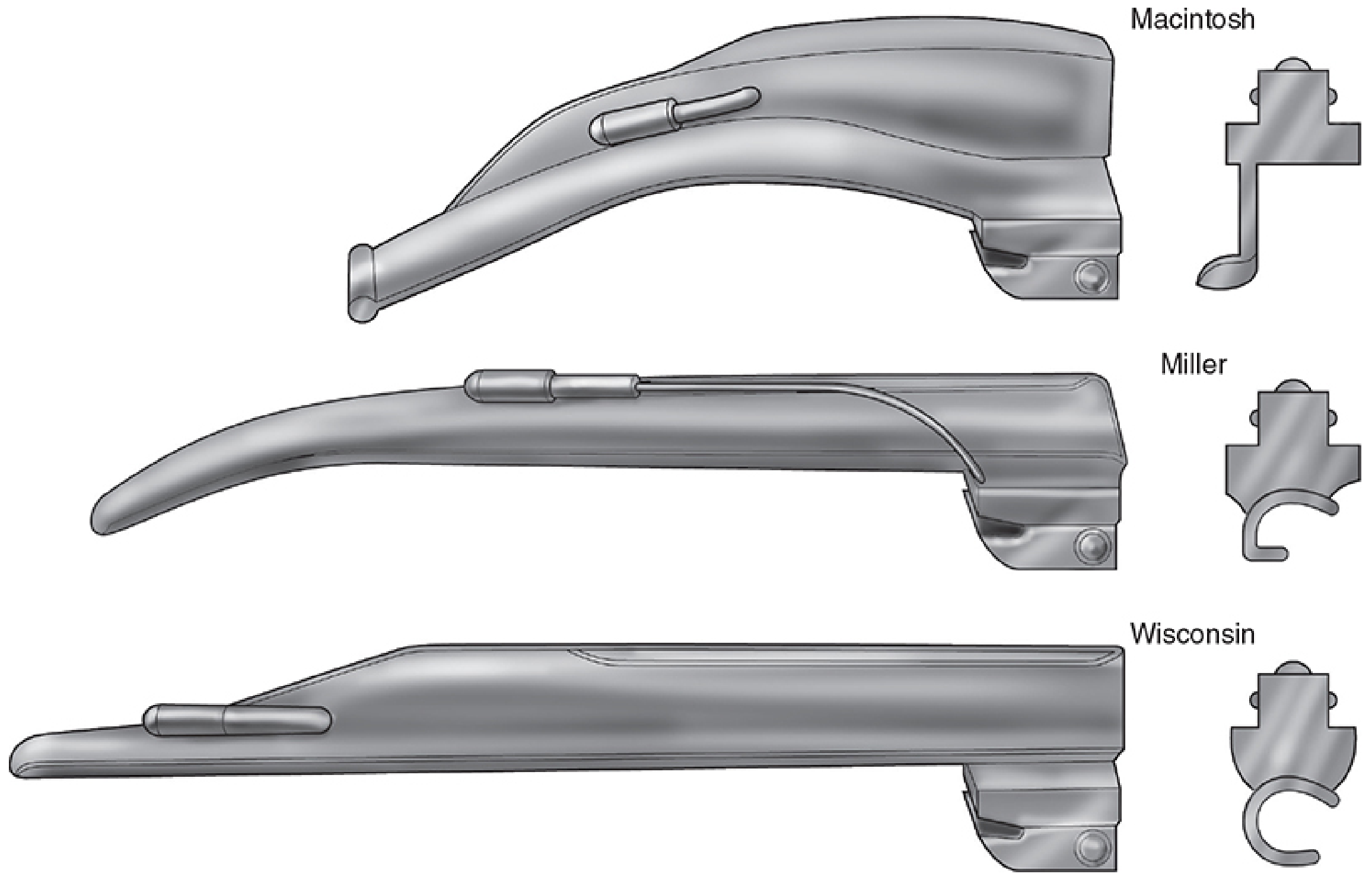
Q2. What are the two basic types of laryngoscope blades? Name the most common examples of each.
A:
| Type | Shape | Most Common Example |
|---|---|---|
| Curved blade | Curved/C-shaped | Macintosh blade |
| Straight blade | Straight | Miller blade |
Other straight blades include the Wisconsin and Flagg blades. Both are designed to be held in the left hand, and both have a flange on the left side to retract the tongue laterally.
(Miller's Anesthesia, 10e; Roberts & Hedges' Clinical Procedures in Emergency Medicine)
Q3. What is the mechanism of action of the Macintosh (curved) blade?
A: The tip of the Macintosh blade is placed in the vallecula (the space between the base of the tongue and the epiglottis). A lifting force directed at a 45-degree angle up and away from the laryngoscopist indirectly lifts the epiglottis by placing tension on the hyoepiglottic ligament, thereby exposing the glottic structures.
- The blade should NOT be used as a lever rocking back on the upper incisors - this damages the teeth and gives an inferior view.
- Force is generated using the anterior deltoid and triceps (wrist should not flex radially).
(Miller's Anesthesia, 10e; Roberts & Hedges')
Q4. What is the mechanism of action of the Miller (straight) blade?
A: The tip of the straight blade is passed posterior to the epiglottis (beneath it) and lifts it directly. The Miller blade is inserted using the paraglossal technique (described by Henderson):
- Insert lateral to the tongue along the paraglossal gutter (between tongue and tonsil)
- Apply continued moderate lifting force to maintain lateral tongue displacement
- As the blade is advanced, the epiglottis comes into view
- Tip is positioned in the midline of the posterior surface of the epiglottis, close to the anterior commissure of the vocal cords
- This achieves good epiglottis control and facilitates tube passage
This method avoids contact of the laryngoscope with the maxillary incisors.
(Miller's Anesthesia, 10e)
Q5. Compare the Macintosh and Miller blades - advantages and disadvantages.
A:
| Feature | Macintosh (Curved) | Miller (Straight) |
|---|---|---|
| Tip position | Vallecula (indirect lift) | Posterior to epiglottis (direct lift) |
| Tongue retraction | Better - wider flange keeps tongue away | Less effective |
| Room for tube passage | More - larger flange | Less |
| Risk of dental damage | Lower | Higher |
| Preferred age group | Adults | Paediatrics |
| Long, floppy epiglottis | Less effective | Better |
| Anterior larynx | Less effective | Better |
| Prominent incisors | Preferred | Less suitable |
| Short thyromental distance | Less suitable | Preferred |
| Laryngospasm risk | Lower | Higher (stimulates superior laryngeal nerve on undersurface of epiglottis) |
| Inadvertent oesophageal passage | Less likely | Can occur - reveals unfamiliar anatomy until withdrawn |
| Blade sizes for adult | Usually size 3 | Usually size 2 |
(Roberts & Hedges'; Miller's Anesthesia, 10e; Morgan & Mikhail's)
Q6. In which hand is the laryngoscope held, and why?
A: The laryngoscope is always held in the left hand. This frees the right hand to:
- Open the mouth (using the scissors technique)
- Guide the endotracheal tube (ETT) through the vocal cords
- Apply external laryngeal manipulation (ELM/BURP)
- Ensure the upper lip is not impinged between the laryngoscope and upper incisors
(Miller's Anesthesia, 10e)
Q7. What is the Cormack-Lehane grading system? Why is it important?
A: Developed by Cormack and Lehane in 1984, this grading scale describes the laryngoscopic view obtained during direct laryngoscopy:
| Grade | View |
|---|---|
| Grade I | Full view of the glottis (epiglottis and vocal cords completely visible) |
| Grade II | Partial view of the glottis |
| Grade III | Only epiglottis visible, no part of glottis seen |
| Grade IV | Neither epiglottis nor glottis visible |
Yentis modification further splits Grade II:
- Grade IIA - partial view of the glottis
- Grade IIB - only arytenoids or posterior vocal cords visible
Clinical significance: Grade I and IIA - intubation rarely difficult; Grades IIB and III - significantly higher incidence of failed intubation; Grade IV - requires an alternate method.
An alternative rating tool is the POGO scale (Percentage of Glottic Opening), which measures what percent of the vocal cords from anterior commissure to arytenoid notch is visible. It has higher interobserver reliability and is useful in research.
(Miller's Anesthesia, 10e)
Q8. What is the BURP manoeuvre? How is it different from cricoid pressure?
A:
-
BURP = Backward, Upward, Rightward Pressure applied on the thyroid cartilage during laryngoscopy to improve glottic visualisation. It is a type of external laryngeal manipulation (ELM). Optimal BURP is achieved when the laryngoscopist guides position with their right hand and an assistant exerts the pressure.
-
Cricoid pressure (Sellick's manoeuvre) = Pressure applied on the anterior cricoid ring to displace it posteriorly, aiming to occlude the oesophagus and prevent regurgitation/aspiration. It is not intended to improve glottic view.
-
Bimanual laryngoscopy = The laryngoscopist uses their own right hand to apply ELM, then an assistant takes over once the optimal position is found.
(Roberts & Hedges')
Q9. What are the blade sizes used in adults and paediatric patients?
A:
- Adults: Macintosh size 3 (most common), Macintosh size 4 for larger patients or long thyromental distance; Miller size 2
- Paediatrics: Straight blades (Miller) are typically preferred; smaller sizes (0, 1, 1.5) are used
- In patients with a very long thyromental distance, a larger blade may be more appropriate
(Miller's Anesthesia, 10e; Roberts & Hedges')
Q10. What are the types of light sources used in laryngoscopes?
A:
- Bulb-at-tip - a bulb illuminates the tip of the blade directly; batteries in the handle power it
- Fiberoptic - a bulb in the handle illuminates a fiberoptic bundle that terminates at the blade tip
- Fiberoptic bundle laryngoscopes can be made MRI-compatible (no ferromagnetic components)
- LED light - modern laryngoscopes increasingly use LED for better brightness and longer life
The Macintosh blade variant with superior brightness was demonstrated in a Philadelphia survey: only 24% of blades in EDs provided adequate brightness. The G-Mac (German) offered clearly superior brightness vs. the A-Mac (American) or intermediate E-Mac (English).
(Morgan & Mikhail's; Roberts & Hedges')
Q11. What is a video laryngoscope (VL)? Name common examples.
A: Video laryngoscopes have a video chip or lens/mirror at the tip of the blade to transmit a view of the glottis to the operator on a screen, without requiring direct line-of-sight alignment.
Three categories:
-
Macintosh-style VLs (can be used for both DL and video-assisted laryngoscopy):
- C-MAC (Karl Storz) - most extensively studied; shorter intubation times; technique identical to DL
- McGrath MAC (Aircraft Medical)
- GlideScope Titanium MAC (Verathon)
-
Hyperangulated/distally angulated VLs ("look around the corner"):
- GlideScope Titanium LoPro (Verathon) - 60-degree angulation
- D-Blade (Karl Storz, for C-MAC system)
- X-Blade (for McGrath MAC)
- Almost always require an ETT stylet (malleable with 60-90 degree bend)
-
Channeled VLs (have a built-in guide channel for the ETT):
- Airtraq
- King Vision
Advantages of VLs (Cochrane 2022 meta-analysis, 222 studies, 26,149 participants):
- Increased first-attempt intubation success
- Reduced rate of failed intubation
- Hyperangulated VLs: reduced esophageal intubation
- Channeled and Macintosh-style VLs: reduced peri-intubation hypoxaemia
- Useful in teaching (instructor sees same view as learner)
- Less cervical spine displacement than DL
(Miller's Anesthesia, 10e; Morgan & Mikhail's; Tintinalli's Emergency Medicine)
Q12. When is a straight blade preferred over a curved blade?
A: The straight (Miller) blade is preferred in:
- Paediatric patients (due to the relatively large, floppy epiglottis and more cephalad larynx)
- Patients with a long, floppy epiglottis (direct lifting is more effective)
- Anterior larynx (short thyromental distance)
- Larynx fixed by scar tissue
- When curved blade has failed to give an adequate view
The straight blade is less effective in patients with prominent upper teeth and is more likely to cause dental damage.
(Roberts & Hedges'; Miller's Anesthesia, 10e)
Q13. What are the complications associated with laryngoscopy?
A:
- Dental damage - particularly with straight blade or incorrect levering technique
- Laryngospasm - more common with straight blade (stimulates superior laryngeal nerve on epiglottis undersurface)
- Soft tissue trauma - lips, tongue, pharynx
- Oesophageal intubation - can occur, especially if straight blade advanced too far (reveals unfamiliar anatomy)
- Cervical spine injury - especially in trauma patients; video laryngoscopes cause less cervical spine displacement
- Hypertension/tachycardia - sympathetic response to laryngoscopy
- Hypoxaemia - if intubation is prolonged
Q14. What is the "sniffing position" and why is it important for laryngoscopy?
A: The sniffing position is achieved by:
- Flexion of the lower cervical spine (neck flexion - usually a pillow under the head)
- Extension of the atlanto-occipital joint (head extension/tilt back)
This aligns the oral, pharyngeal, and laryngeal axes to create a straight line of sight from the lips to the glottis, facilitating direct laryngoscopy. It is sometimes described as the position adopted when sniffing a flower or morning air.
Video laryngoscopes reduce dependence on this positioning, as they can achieve glottic visualisation without requiring full axial alignment.
(Morgan & Mikhail's; Miller's Anesthesia, 10e)
Q15. What is the technique for opening the mouth before laryngoscope insertion?
A: The scissors technique is used:
- The right thumb presses caudally (downward) on the right lower molars
- The index or third finger of the right hand presses cephalad (upward) on the right upper molars
- This crosses the fingers like scissors to open the mouth
After insertion of the laryngoscope, the right hand can be used to ensure the upper lip is not caught between the blade and the upper incisors.
(Miller's Anesthesia, 10e)
Q16. What is the direction of force applied while using the laryngoscope?
A: Force should be directed upward and forward at a 45-degree angle (toward the junction of the opposite wall and ceiling), using the anterior deltoid and triceps muscles. This is the same direction for both Macintosh and Miller blades.
Common mistake to avoid: Do not lever/rock back on the upper incisors to lift the blade tip. This:
- Damages the teeth
- Provides an inferior glottic view
(Roberts & Hedges'; Miller's Anesthesia, 10e)
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7e, pp. 591-593
- Miller's Anesthesia, 10e, pp. 5908-5935
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, pp. 118-123
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide
This is a shared conversation. Sign in to Orris to start your own chat.