Hypersensitivity
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I have rich, comprehensive content across all four types. I now have enough to write a thorough, well-structured answer. Let me compile everything.
Hypersensitivity
Hypersensitivity refers to immune responses that are excessive, misdirected, or occur at inappropriate locations - causing tissue damage (immunopathology) rather than protection. The underlying effector mechanisms are the same ones used in normal host defense; the problem is that they are overactivated against antigens that pose no real threat, such as innocuous environmental antigens, self-antigens, or antigens from another species.
The classification system introduced by Gell and Coombs (1963) divides hypersensitivity into four types (I-IV). Subsequent work has added a Type V and recognition of innate hypersensitivity reactions.
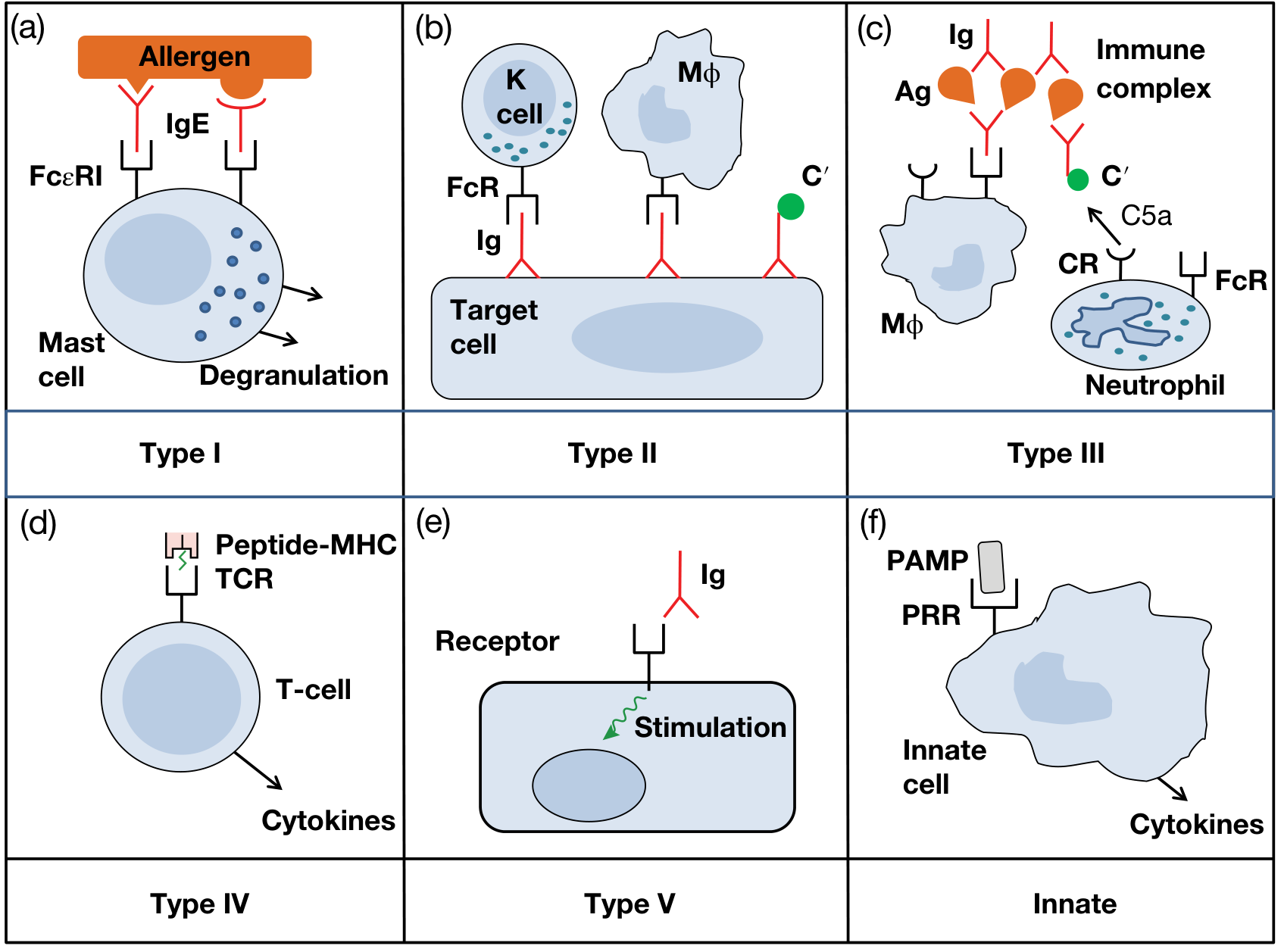
Figure 14.1 - Six categories of hypersensitivity (Roitt's Essential Immunology, 13th Ed.)
Summary Table (Gell and Coombs Classification)
| Feature | Type I | Type II | Type III | Type IV |
|---|---|---|---|---|
| Name | Immediate / Anaphylactic | Cytotoxic | Immune Complex | Cell-Mediated / Delayed |
| Immune reactant | IgE | IgG | IgG | T cells |
| Effector cells | Mast cells, basophils, eosinophils | Complement, phagocytes | Complement, phagocytes, neutrophils | Macrophages, cytotoxic T cells |
| Onset | Minutes | Minutes-hours | Hours | 48-72 hours |
| Disease examples | Allergic rhinitis, anaphylaxis, asthma | Haemolytic anaemia, Goodpasture's | Serum sickness, SLE, post-streptococcal GN | Contact dermatitis, tuberculin reaction, graft rejection |
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Table 14.1
Type I - Immediate (IgE-Mediated) Hypersensitivity
Mechanism: Allergen exposure in a sensitized individual cross-links IgE molecules already bound to the high-affinity FcεRI receptors on mast cells and basophils. This triggers explosive degranulation, releasing preformed mediators (histamine, tryptase, heparin) and prompting synthesis of lipid mediators (prostaglandins, leukotrienes) and cytokines.
Two phases:
- Early phase (within minutes): Histamine-mediated vasodilation, bronchoconstriction, increased vascular permeability, and mucus secretion.
- Late phase (4-12 hours): Eosinophil-dominated inflammation driven by Th2 cytokines (IL-4, IL-5, IL-13), causing prolonged tissue damage.
Sensitization: Initial antigen exposure drives Th2 differentiation, IL-4/IL-13 production, and B-cell class switching to IgE production. IgE then coats mast cells throughout the body, "priming" for future exposure.
Clinical examples:
- Anaphylaxis (penicillin, bee sting, peanuts)
- Allergic rhinitis (hayfever)
- Atopic asthma
- Urticaria and atopic eczema
- Food allergy (cow's milk, eggs, nuts, shellfish)
Treatment principles: Epinephrine (reverses bronchospasm and vasodilation - the cornerstone of anaphylaxis treatment), antihistamines (H1 blockers), corticosteroids, mast cell stabilizers (sodium cromoglycate), leukotriene antagonists (montelukast), and anti-IgE biologics (omalizumab).
- Roitt's Essential Immunology, 13th Ed., Chapter 14
Type II - Cytotoxic (Antibody-Dependent) Hypersensitivity
Mechanism: IgG (or IgM) antibodies bind directly to antigens on cell surfaces or extracellular matrix. This triggers cell destruction via three pathways:
- Complement activation - classical pathway generates MAC (C5b-C9), causing direct cell lysis
- Opsonization and phagocytosis - C3b and Fc receptors on phagocytes mediate cell engulfment
- Antibody-Dependent Cellular Cytotoxicity (ADCC) - NK cells, monocytes, and eosinophils bind antibody-coated targets via FcγR and kill them without phagocytosis
Clinical examples:
- ABO transfusion reactions - pre-existing antibodies against ABO antigens lyse incompatible red cells
- Haemolytic disease of the newborn (Rh incompatibility) - maternal anti-D IgG crosses placenta
- Goodpasture's syndrome - anti-GBM antibodies destroy glomerular and alveolar basement membranes
- Autoimmune haemolytic anaemia and immune thrombocytopenia (ITP)
- Bullous pemphigoid - IgG against hemidesmosomal proteins (BP180/BP230), causing subepidermal blisters with eosinophilic infiltrate
- Roitt's Essential Immunology, 13th Ed.; Goldman-Cecil Medicine
Type III - Immune Complex-Mediated Hypersensitivity
Mechanism: Soluble antigen-antibody (IgG) complexes form in the circulation or in tissues. Normally these are cleared by the mononuclear phagocyte system (MPS). When complexes are produced in excess or not cleared efficiently, they deposit in vessel walls, glomeruli, and synovium. Deposited complexes activate complement, generating C3a and C5a (anaphylatoxins), which attract neutrophils. Neutrophil degranulation releases proteases and reactive oxygen species, causing local tissue injury.
Types I, II, and III are all antibody-mediated. Type III is distinguished by the fact that the antigen is soluble (not on a cell surface).
Clinical examples:
- Serum sickness - systemic reaction 1-2 weeks after injection of foreign protein (horse antitoxin); fever, arthralgia, urticaria, lymphadenopathy
- Systemic lupus erythematosus (SLE) - anti-dsDNA immune complexes deposit in kidneys, skin, and joints
- Post-streptococcal glomerulonephritis - streptococcal antigen-antibody complexes deposit in glomeruli
- Hypersensitivity pneumonitis (Farmer's lung) - inhaled fungal spores form immune complexes in lung parenchyma
- Arthus reaction - local tissue necrosis from intradermal antigen injection in a pre-immunized individual
- Roitt's Essential Immunology, 13th Ed.; Goldman-Cecil Medicine
Type IV - Delayed-Type (Cell-Mediated) Hypersensitivity
Mechanism: Unlike Types I-III, Type IV does not involve antibodies. It is entirely T cell-mediated. Sensitized CD4+ Th1 cells recognize antigen (presented on MHC II by antigen-presenting cells) and release cytokines - particularly IFN-γ, which activates macrophages, causing inflammation and tissue destruction. CD8+ cytotoxic T cells are also involved in some forms (e.g., contact dermatitis).
Onset is delayed (48-72 hours) because it takes time to recruit and activate sufficient effector T cells and macrophages at the site of antigen deposition.
Subtypes (Cher classification):
- IVa - Th1-mediated, macrophage activation (tuberculin test, Crohn's disease)
- IVb - Th2-mediated, eosinophilic inflammation (contact dermatitis to nickel)
- IVc - Cytotoxic T cell-mediated (Stevens-Johnson syndrome)
- IVd - Neutrophil-mediated, T cell-dependent (AGEP)
Clinical examples:
- Tuberculin (Mantoux) test - induration at 48-72 h is classic delayed hypersensitivity
- Contact dermatitis - nickel, poison ivy, latex
- Granulomatous diseases - tuberculosis, sarcoidosis (macrophages fail to clear persistent antigen, forming granulomas)
- Graft rejection - T cell-mediated destruction of allogeneic tissue
- Type 1 diabetes mellitus (CD8+ T cell destruction of pancreatic beta cells)
- Roitt's Essential Immunology, 13th Ed.; Goldman-Cecil Medicine
Type V - Stimulatory Hypersensitivity (Addition to Classic Classification)
Mechanism: Antibodies bind to cell surface receptors and act as agonists, mimicking the normal ligand and stimulating the cell rather than destroying it. This is distinct from Type II because the outcome is cell overstimulation, not cytotoxicity.
Clinical example:
- Graves' disease - TSI (thyroid-stimulating immunoglobulin) antibodies bind TSH receptor on thyroid follicular cells, mimicking TSH and causing unregulated hyperthyroidism
- Roitt's Essential Immunology, 13th Ed.
Innate Hypersensitivity
Excessive or inappropriately activated pattern recognition receptors (PRRs) - such as Toll-like receptors (TLRs) - can trigger cytokine storms and inflammatory tissue damage without involving adaptive immunity. This is increasingly recognized in conditions like sepsis and cytokine release syndrome.
Key Points to Remember
| Point | Detail |
|---|---|
| Types I, II, III = antibody-mediated | Type IV = cell-mediated |
| Type I antigen = soluble; extracellular | Type II antigen = cell surface or matrix-bound |
| Type III antigen = soluble (circulating) | Type IV antigen = intracellular or cell-surface (presented by MHC) |
| Most allergies (hayfever, asthma, eczema, food) | Type I (IgE); some eczema is Type IV |
| Serum sickness prototype | Type III |
| Tuberculin test prototype | Type IV |
| A single disease can involve multiple types | e.g., SLE involves Types II, III, and IV |
Sources:
- Roitt's Essential Immunology, 13th Edition, Chapter 14 (Allergy and Other Hypersensitivities)
- Goldman-Cecil Medicine, International Edition, Chapter on Hypersensitivity
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1, Table 14.1
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th Edition, Chapter on Immune Function
This is a shared conversation. Sign in to Orris to start your own chat.