Guideline on how and when to start insulin in diabetes mellitus
Reading File
Finding Sources
Finding Sources
Searching PubMed
"insulin initiation" AND "type 2 diabetes"
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete guideline answer.
Insulin in Diabetes Mellitus: When and How to Start
Overview
Insulin is the most potent glucose-lowering agent available and is the treatment of choice for type 1 diabetes mellitus (T1DM) and an important option at multiple stages of type 2 diabetes mellitus (T2DM). Its timely initiation reduces insulin resistance, induces beta-cell rest, and minimizes both micro- and macrovascular complications through a mechanism called "metabolic memory."
- Textbook of Family Medicine 9e, p. 978
PART 1 - TYPE 1 DIABETES
When to Start
Insulin is mandatory from diagnosis in T1DM - there are no alternatives because absolute insulin deficiency is the fundamental defect.
What Regimen to Use
A physiological (basal-bolus) regimen is the standard of care:
| Component | Insulin Type | Timing |
|---|---|---|
| Basal | Glargine, detemir, or degludec | Once daily (bedtime or morning) |
| Bolus (prandial) | Lispro, aspart, or glulisine | 15 min before each meal |
| Correction | Same rapid-acting analog | Added to bolus as needed |
An alternative is continuous subcutaneous insulin infusion (CSII/insulin pump) using rapid-acting analogs - preferred for patients with hypoglycemia unawareness, highly variable glucose, or who require tight control (e.g., pregnancy).
HbA1c target: <7% for most patients; <6.5% if achievable without hypoglycemia in young, newly diagnosed individuals.
PART 2 - TYPE 2 DIABETES
When to Start Insulin
T2DM is a progressive disease with gradual beta-cell failure. Insulin is typically introduced at several decision points:
1. At Diagnosis (Early/Intensive Initiation)
Consider immediate insulin therapy when:
- HbA1c >9.0% with symptomatic hyperglycemia (polyuria, polydipsia, weight loss)
- HbA1c >8.5% with symptoms
- Fasting glucose consistently >200 mg/dL
Short-term (2 weeks to 3 months) intensive insulin in newly diagnosed T2DM with high HbA1c can induce beta-cell rest and may improve long-term outcomes. - Goldman-Cecil Medicine, p. 1056
2. Oral Agent Failure (Most Common Scenario)
Start insulin when:
- Adequate trial of 2-3 oral/non-insulin injectable agents fails to achieve target HbA1c
- HbA1c remains >7-8% despite maximally tolerated oral agents
- Progressive beta-cell failure (common after 10-15 years of T2DM)
3. Special Circumstances
- Hospitalization / critical illness: Initiate insulin for blood glucose >180 mg/dL (target 140-180 mg/dL); 80-110 mg/dL may be targeted in select ICU settings
- Pregnancy (gestational diabetes / pre-existing DM): Insulin is the preferred agent; initiate before pregnancy in those with pre-existing DM, targeting HbA1c <6%
- Renal/hepatic failure: When oral agents are contraindicated
- Steroid-induced hyperglycemia
- DKA or hyperosmolar state (even in T2DM)
How to Start Insulin in T2DM: Step-by-Step
Step 1 - Choose the Starting Regimen
Basal insulin first is the preferred approach for most outpatients:
- Start with glargine, detemir, or degludec (long-acting analogs preferred over NPH to minimize hypoglycemia risk)
- Starting dose: 10 units once daily (bedtime or morning), OR 0.1-0.2 units/kg/day
- Can be combined safely with metformin, SGLT-2 inhibitors, DPP-4 inhibitors, and GLP-1 receptor agonists
- Approximately 60% of T2DM patients achieve HbA1c ≤7% with basal insulin + oral agents - Textbook of Family Medicine 9e, p. 1591
Step 2 - Titrate the Dose
A common self-titration protocol (the "2-2-2 rule" or similar):
- Increase basal dose by 2 units every 3 days if fasting glucose is 130-180 mg/dL
- Increase by 4 units if fasting glucose >180 mg/dL
- Reduce dose if any fasting glucose reading is <80 mg/dL
Target fasting glucose: 80-130 mg/dL
Step 3 - Add Prandial Insulin When Needed
Consider adding rapid-acting prandial insulin when:
- HbA1c remains >7% despite fasting glucose <100 mg/dL on optimized basal insulin
- Basal insulin dose has exceeded 60 units/day
- Patient has not met HbA1c goal within 1 year of starting basal insulin
- "BeAM factor" (bedtime glucose minus morning glucose) is >55 mg/dL - this indicates uncontrolled postprandial glucose
- Repeated nocturnal hypoglycemia on basal titration
Starting prandial dose: 4-6 units with the largest meal, titrated up by 1-2 units every 3 days based on 2-hour postprandial glucose target (<180 mg/dL).
Inpatient Dosing (Hospitalized T2DM Patients)
- Starting dose: 8-16 units long-acting insulin + 3-5 units rapid-acting before each meal
- Add a correction dose of 1-2 units per 50 mg/dL above target
- Target glucose: 140-180 mg/dL in non-critical care settings
Insulin Pharmacokinetic Profile
The figure below shows the onset and duration of action for all major insulin types:
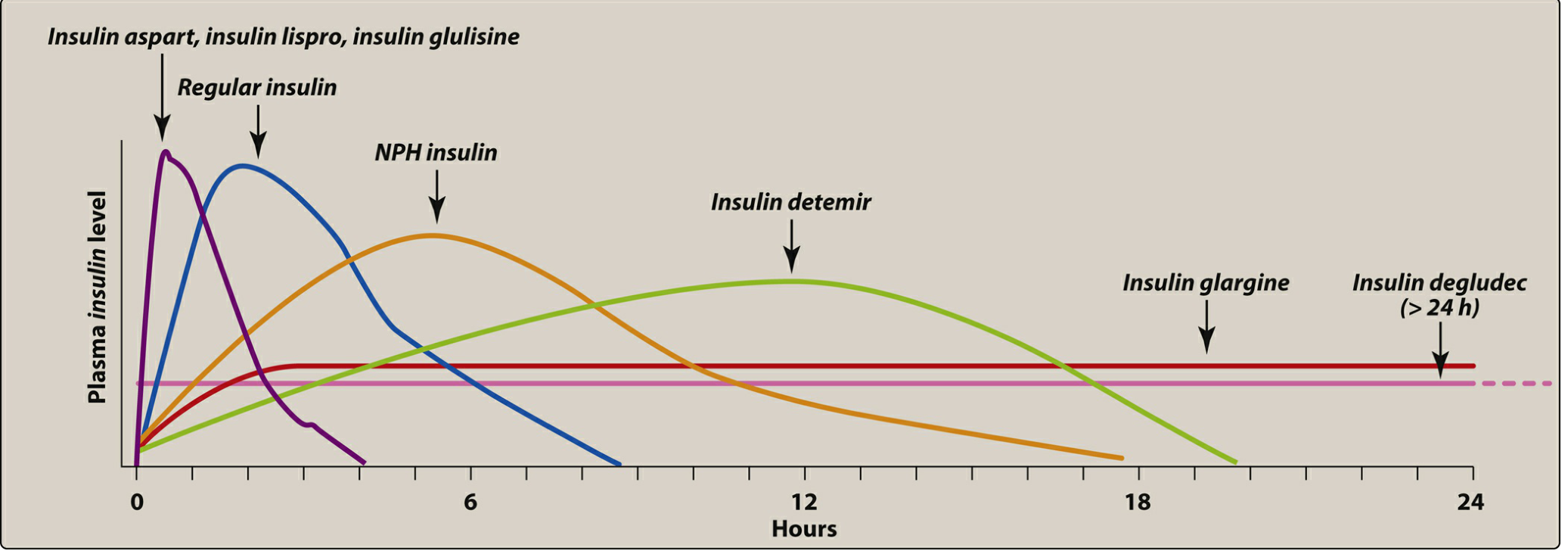
| Type | Examples | Onset | Peak | Duration |
|---|---|---|---|---|
| Rapid-acting | Lispro, Aspart, Glulisine | 15 min | 1-2 h | 3-5 h |
| Short-acting | Regular human | 30-60 min | 2-4 h | 6-8 h |
| Intermediate | NPH | 1-2 h | 4-10 h | 12-18 h |
| Long-acting | Glargine, Detemir | 1-2 h | Peakless | 20-24 h |
| Ultra-long | Degludec | 1-2 h | Flat | >24 h |
Common Insulin Regimens
The diagram below illustrates three standard insulin regimens:
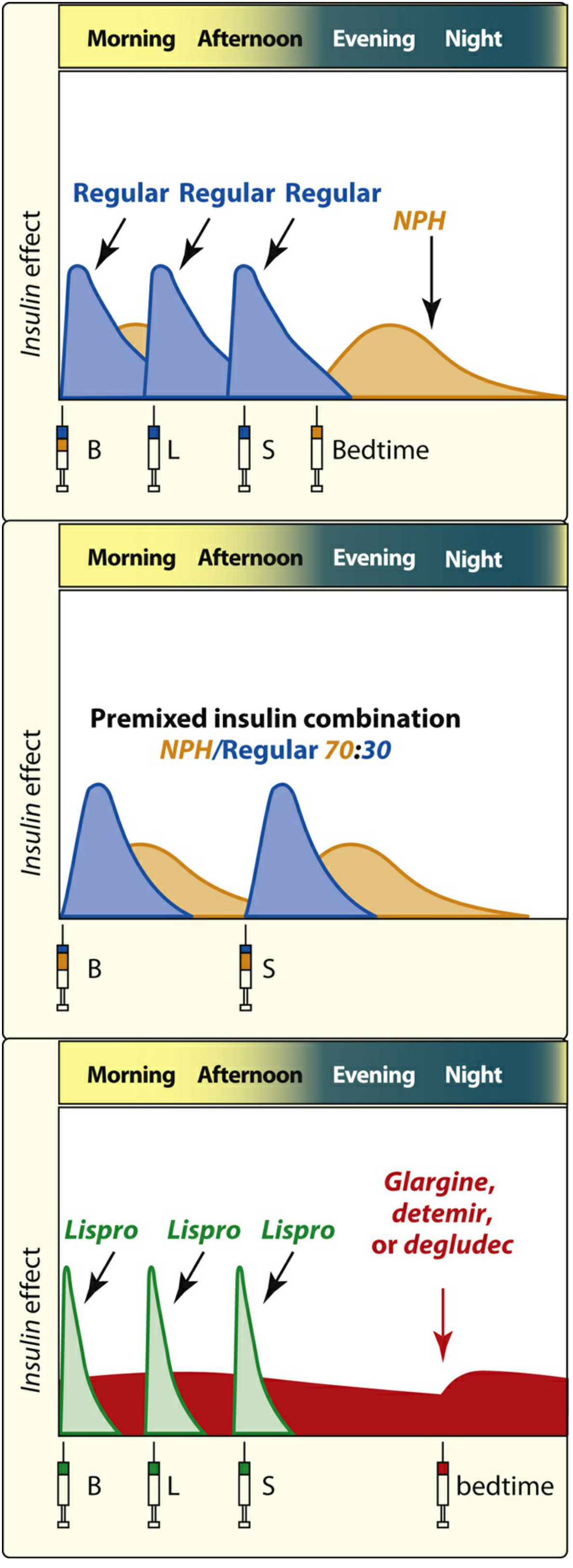
- Conventional: Regular insulin at each meal + NPH at bedtime
- Premixed (70:30 NPH/Regular): Twice daily injections - simpler, for patients with regular meal schedules and HbA1c 8.5-10%
- Basal-Bolus (preferred): Long-acting at bedtime + rapid-acting analog at each meal - most physiological, best glycemic control
Practical Keys to Successful Insulin Initiation
The following points are evidence-based recommendations from the Textbook of Family Medicine 9e (Table 34-20):
- Explain the difference between "basal" and "bolus" insulin to minimize dosing errors
- Use insulin pens or disposable pumps rather than syringes - improves accuracy and adherence
- Inject rapid-acting analogs 15 minutes before meals (unless pre-meal glucose <80 mg/dL)
- Use analog insulins rather than regular human insulin to reduce hypoglycemia risk
- When adding a GLP-1 receptor agonist to basal insulin, reduce the basal dose by 20%
- Teach patients structured self-monitoring of blood glucose (SMBG) to detect impending hypoglycemia
- Patients with renal insufficiency should reduce insulin doses by 10% and monitor carefully (reduced renal insulin clearance increases hypoglycemia risk)
- To reduce weight gain: consider discontinuing sulfonylureas, thiazolidinediones, or glinides when insulin is started
- Agents safely continued alongside insulin: metformin, bromocriptine, SGLT-2 inhibitors, alpha-glucosidase inhibitors, DPP-4 inhibitors (not with GLP-1 agonists)
- Always provide patients with a written, individualized titration plan
Glycemic Targets Summary
| Setting | Target |
|---|---|
| HbA1c (most adults) | <7% |
| HbA1c (young, no hypoglycemia risk) | <6.5% |
| HbA1c (elderly, comorbidities, hypoglycemia unawareness) | 7-8% |
| Fasting glucose | 80-130 mg/dL |
| 2-hour postprandial glucose | <180 mg/dL |
| Inpatient (non-ICU) | 140-180 mg/dL |
Recent evidence note: A 2026 systematic review and network meta-analysis (PMID: 41436667) in Diabetologia compared insulin regimens in T2DM, confirming that basal-bolus regimens provide the greatest HbA1c reduction but with higher hypoglycemia rates. Basal insulin alone remains the preferred starting point due to its simplicity and safety.
This is a shared conversation. Sign in to Orris to start your own chat.