Types of Pulmonary hypetension
Reading File
Finding Sources
Searching PubMed
"pulmonary hypertension" classification
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have all the key information needed. Let me compile the comprehensive answer.
Types of Pulmonary Hypertension
Definition
Pulmonary hypertension (PH) is defined hemodynamically as a mean pulmonary artery pressure (mPAP) > 20 mmHg at rest on right heart catheterization (RHC), updated from the older threshold of >25 mmHg at the 6th World Symposium on Pulmonary Hypertension (WSPH, 2018). - Harrison's Principles of Internal Medicine, 22nd Ed.
WHO/WSPH Clinical Classification (6th WSPH, 2018)
The current classification divides PH into 5 groups based on underlying etiology and pathophysiological mechanism. Assignment to the correct group is essential because only Groups 1 and 4 have specific, proven targeted therapies. - Murray & Nadel's Textbook of Respiratory Medicine
Group 1 - Pulmonary Arterial Hypertension (PAH)
Mechanism: Precapillary - characterized by marked pulmonary arterial remodeling (intimal fibrosis, medial hypertrophy, plexiform lesions). Hemodynamic criteria: mPAP >20 mmHg + PVR >2.0 Wood Units + PAWP ≤15 mmHg. - Harrison's 22E
| Sub-type | Notes |
|---|---|
| 1.1 Idiopathic PAH (IPAH) | Most common; mean age at diagnosis now 54-68 years; female predominance (~3:1) |
| 1.2 Heritable PAH | Most commonly BMPR2 mutation; younger at diagnosis, more severe |
| 1.3 Drug- and toxin-induced | Anorexigens (fenfluramine), methamphetamine, dasatinib |
| 1.4 Associated PAH | Connective tissue disease, HIV, portal hypertension (portopulmonary), congenital heart disease, schistosomiasis |
| 1.5 PAH long-term responders to CCBs | Acute vasoreactivity test positive subset |
| 1.6 PAH with PVOD/PCH features | Pulmonary veno-occlusive disease / pulmonary capillary hemangiomatosis overlap |
| 1.7 Persistent PH of the newborn |
Epidemiology: PAH is rare (~15 cases per million adults) but disproportionately affects young, otherwise healthy women. In resource-rich countries, PAH accounts for only ~3% of pulmonary vascular disease.
Group 2 - PH Due to Left Heart Disease (Most Common Overall)
Mechanism: Postcapillary - elevated pulmonary venous pressure transmitted backward from the left heart. Left heart disease and lung disease are the most common causes of PH in developed countries. In one large RHC cohort, 46% of patients had Group 2 vs. only 16% with precapillary PAH. - Fuster & Hurst's The Heart, 15th Ed.
| Sub-type |
|---|
| 2.1 HF with preserved ejection fraction (HFpEF) - increasingly the leading cause |
| 2.2 HF with reduced/mildly reduced ejection fraction (HFrEF) |
| 2.3 Valvular heart disease |
| 2.4 Congenital/acquired cardiovascular conditions causing postcapillary PH |
Group 3 - PH Due to Lung Disease and/or Hypoxia
Mechanism: Precapillary - hypoxic pulmonary vasoconstriction + parenchymal/vascular remodeling. Second most common cause of PH in developed countries.
| Sub-type |
|---|
| 3.1 Obstructive lung disease (COPD) - ~1/3 of end-stage COPD patients referred for transplant have PH |
| 3.2 Restrictive lung disease (ILD, pulmonary fibrosis) |
| 3.3 Mixed obstructive/restrictive pattern |
| 3.4 Hypoventilation syndromes (OSA, obesity-hypoventilation/Pickwickian) - usually mild PH |
| 3.5 Hypoxia without lung disease (e.g. high altitude) |
| 3.6 Developmental lung disorders |
Group 4 - PH Due to Pulmonary Artery Obstructions (CTEPH)
Mechanism: Mechanical obstruction + secondary vascular remodeling. Occurs in ~3-4% of all patients after acute pulmonary embolism. Uniquely potentially curable with pulmonary thromboendarterectomy (PTE). About 25% of CTEPH patients have no documented prior PE. - Murray & Nadel's, Fuster & Hurst's
| Sub-type |
|---|
| 4.1 Chronic thromboembolic PH (CTEPH) |
| 4.2 Other pulmonary artery obstructions (sarcomas, other malignant/non-malignant tumors, hydatid cysts) |
CTEPH can be clinically identical to IPAH - distinguishing them is essential because treatment differs fundamentally.
Group 5 - PH with Unclear and/or Multifactorial Mechanisms
A heterogeneous group where the mechanism causing PH is not clearly established or involves multiple contributing pathways. - Harrison's 22E
| Sub-type | Examples |
|---|---|
| 5.1 Hematological disorders | Chronic hemolytic anemia, myeloproliferative disorders |
| 5.2 Systemic disorders | Sarcoidosis, pulmonary Langerhans cell histiocytosis, neurofibromatosis type 1 |
| 5.3 Metabolic disorders | Glycogen storage disease, Gaucher disease, thyroid disorders |
| 5.4 Chronic renal failure (with or without hemodialysis) | |
| 5.5 Pulmonary tumor thrombotic microangiopathy | |
| 5.6 Fibrosing mediastinitis |
Global Epidemiology by Group
The chart below (from Fuster & Hurst's The Heart, 15th Ed.) illustrates the striking difference in cause distribution between resource-rich and resource-limited settings:
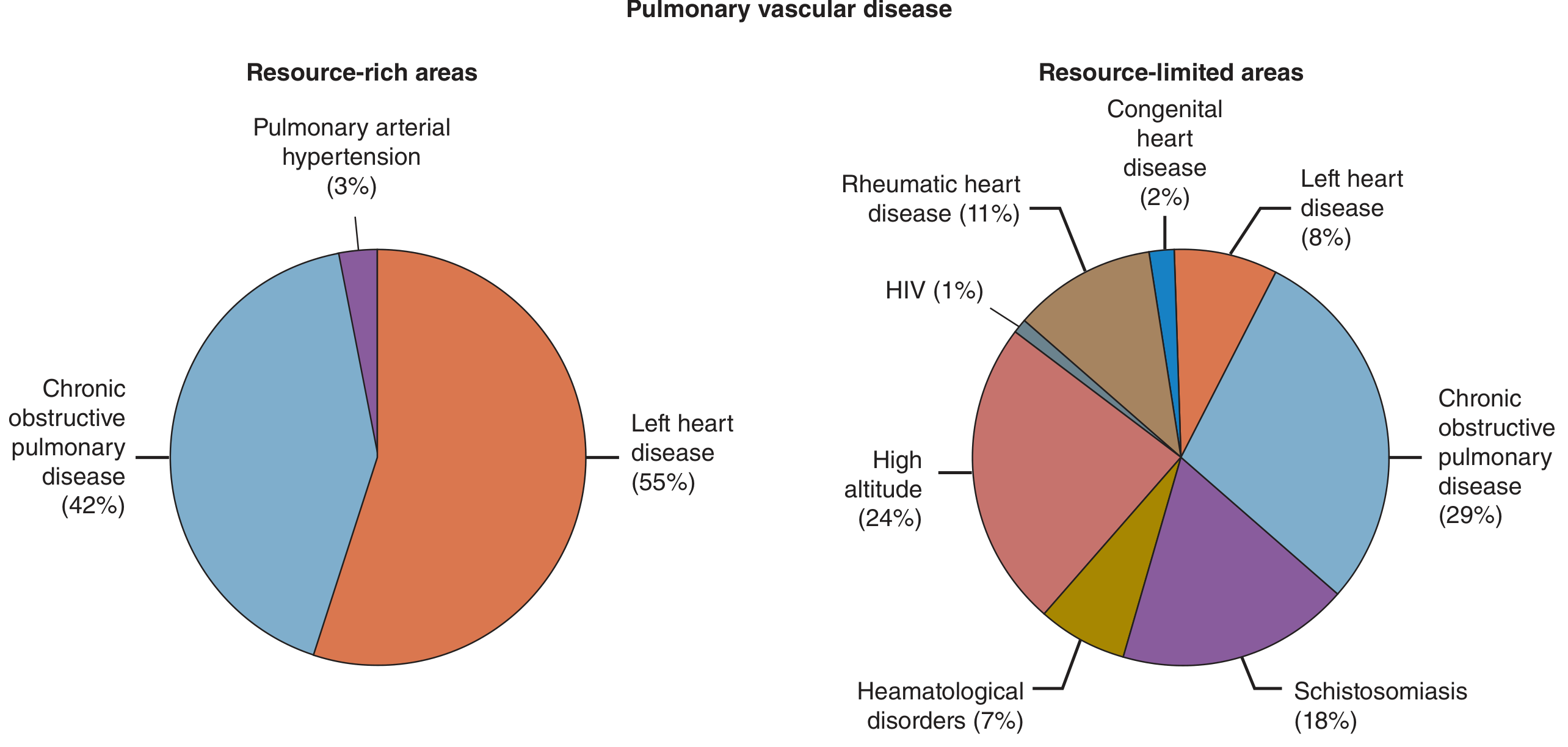
In resource-rich areas: left heart disease (55%) and COPD (42%) dominate; PAH is only 3%.
In resource-limited areas: high altitude (24%), schistosomiasis (18%), and COPD (29%) are prominent; infectious/inflammatory disorders play a much larger role.
Key Hemodynamic Classification Points
| Hemodynamic Type | mPAP | PAWP | PVR | Associated Groups |
|---|---|---|---|---|
| Precapillary PH | >20 mmHg | ≤15 mmHg | >2 WU | Groups 1, 3, 4, 5 |
| Postcapillary PH | >20 mmHg | >15 mmHg | - | Group 2 |
| Combined pre+postcapillary | >20 mmHg | >15 mmHg | >2 WU | Group 2 (severe) |
Clinical Importance of Classification
- Groups 1 & 4 are the only groups with approved targeted therapies (prostacyclins, endothelin antagonists, PDE-5 inhibitors for Group 1; PTE surgery + riociguat for Group 4)
- Groups 2 & 3 are treated by managing the underlying left heart or lung disease; PAH-specific drugs are generally not indicated and may be harmful
- Group 5 has no specific treatments; management targets the underlying systemic condition
Sources: Harrison's Principles of Internal Medicine 22E; Fuster & Hurst's The Heart 15th Ed.; Murray & Nadel's Textbook of Respiratory Medicine
1 day itinerary for travel near Ahmedabad
Asking for Preferences
Searching the Web
nature outdoor day trip within 50 km Ahmedabad 2025
Searching the Web
Thol Lake Bird Sanctuary Indroda Nature Park Ahmedabad visit timings entry fee 2025
I have all the details I need. Note that today is Sunday, July 12, 2026 - currently monsoon season in Gujarat, and Indroda Nature Park is closed on Mondays (relevant for tomorrow planning). Here's your itinerary:
1-Day Nature Itinerary Near Ahmedabad (Within 50 km)
Today is Sunday - perfect timing. It's also monsoon season (July), so the landscape is lush green, lakes are full, and birds are active.
Route Overview
Ahmedabad → Thol Lake Bird Sanctuary → Indroda Nature Park (Gandhinagar) → Back to Ahmedabad
Total driving: ~80 km round trip | Total drive time: ~2 hours combined
Morning: Thol Lake Bird Sanctuary
Distance from Ahmedabad: ~25 km (~45 min drive, via SH 41)
Timings: 6:00 AM - 6:30 PM
Entry fee: ₹50/person | Parking: ₹200-300 extra
Arrive at 6:00–6:30 AM - the golden hour. The lake is especially beautiful in monsoon with overflowing banks and green surroundings.
What to do:
- Walk the bund (embankment trail) around the lake - roughly 3-4 km, flat and easy
- Spot flamingos, painted storks, spoonbills, purple moorhens, jacanas, herons and 150+ species
- Photography is the main draw - bring binoculars if you have them
- The monsoon brings good numbers of resident breeding birds even outside peak winter migration season
Spend: ~2.5 to 3 hours (depart by ~9:30 AM)
Breakfast: Carry packed snacks/tea from Ahmedabad - there are minimal food stalls near the sanctuary. Alternatively, stop at a dhaba on the highway back toward Gandhinagar.
Mid-Morning to Afternoon: Indroda Nature Park, Gandhinagar
Distance from Thol: ~35 km (~40 min) | From Ahmedabad: 25 km
Timings: 8:30 AM - 5:30 PM (Tue-Sun) | Closed Mondays
Entry fee: Free for under-5 | ₹15 (children 5-12) | Adults: nominal fee (₹30-50)
Arrive around 10:30 AM
Often called "India's Jurassic Park", Indroda spreads over 400 hectares along the Sabarmati river in Gandhinagar. In monsoon, it turns strikingly green.
What to do:
- Dinosaur & Fossil Park - one of the largest dinosaur fossil collections in Asia, open-air displays
- Zoo - crocodiles, deer, birds, reptiles in naturalistic enclosures
- Botanical Garden - herbs, shrubs, and climbers native to Gujarat
- Wilderness Park (east of Sabarmati) - light walking trails through scrub forest
Spend: 2.5 to 3 hours
Lunch: Gandhinagar
After Indroda, head into central Gandhinagar for lunch. Try:
- Sector 21 area - several Gujarati thali restaurants
- Swati Snacks or any local joint for authentic Gujarati fare (dal dhokli, fafda, thepla)
Late Afternoon: Sabarmati Riverfront / Adalaj Stepwell (on the way back)
Adalaj Vav (Stepwell) - ~18 km from Gandhinagar, directly on the route back to Ahmedabad
Timings: Open all day | Entry: Free
Not purely outdoors, but Adalaj is a stunning 15th-century stepwell surrounded by gardens - a 30-minute stop worth making. In monsoon, the stone is cool and the light is gorgeous.
Evening: Back to Ahmedabad
Reach Ahmedabad by 5:30 - 6:00 PM. If you want to close the day outdoors, the Sabarmati Riverfront in Ahmedabad is a pleasant evening walk with street food stalls.
Summary Table
| Time | Place | Distance from AMD | Entry |
|---|---|---|---|
| 6:00 - 9:30 AM | Thol Lake Bird Sanctuary | 25 km | ₹50 |
| 10:30 AM - 1:30 PM | Indroda Nature Park, Gandhinagar | 25 km | ~₹50 |
| 1:30 - 2:30 PM | Lunch in Gandhinagar | - | - |
| 3:00 - 3:30 PM | Adalaj Stepwell (optional) | 18 km | Free |
| 5:30 PM | Back in Ahmedabad | - | - |
Monsoon Tips (July)
- Carry a light rain poncho - not a heavy umbrella (you'll be walking trails)
- Wear closed shoes with grip - the Thol bund can get muddy
- Start early at Thol - birds are most active at dawn, and it gets humid by 9 AM
- Mosquito repellent is a must, especially near the lake
- Road to Thol via Kalol highway is smooth; Gandhinagar roads are excellent
How much is the total population if ahmedabad
Searching the Web
Ahmedabad total population 2024 2025
Here's a clear breakdown of Ahmedabad's population figures from multiple sources:
Ahmedabad Population (2026)
| Scope | Population | Source |
|---|---|---|
| City proper (municipal limits) | ~7.7 million | Wikipedia / 2023 estimate |
| Urban agglomeration | ~8.77 million | Wikipedia / 2023 estimate |
| Metro area projection (2026) | ~10.59 million | World Population Review |
| Last official census (2011) | 5.57 million (city) | Census of India |
Key Context
- The 2011 Census recorded the city population at 5,570,585, making it India's 5th most populous city at the time.
- India's 2021 Census has been delayed and is still pending as of 2026, so all current figures are projections/estimates.
- The metro area is growing at roughly 3.46% per year, one of the faster growth rates among major Indian cities.
- Ahmedabad ranks 7th among Indian urban agglomerations (after Delhi, Kolkata, Mumbai, Bengaluru, Chennai, and Hyderabad).
Bottom line: The most commonly cited current population for Ahmedabad city is approximately 7.5 - 8 million, with the broader metro region crossing 10 million in 2025-26 projections.
This is a shared conversation. Sign in to Orris to start your own chat.