Explain mechanism of gastric secretion and its regulation with peptic ulcer reference taken from ganong
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have all the content needed from Ganong's. Let me compose the comprehensive answer.
Gastric Secretion: Mechanism and Regulation
Source: Ganong's Review of Medical Physiology, 26th Edition
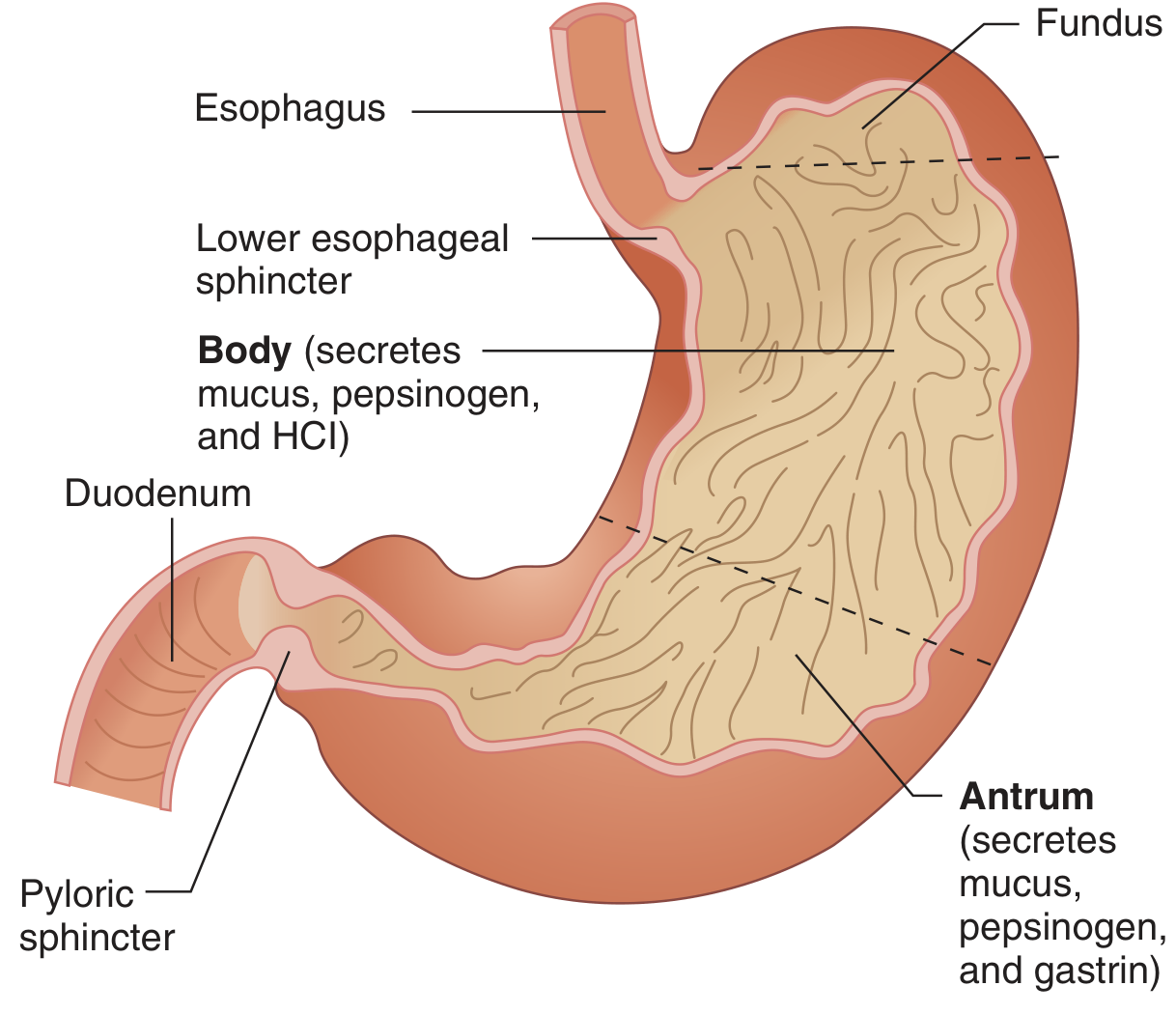
1. Anatomic Basis
The stomach stores food, mixes it with acid, mucus, and pepsin, then releases it at a controlled rate into the duodenum. The gastric mucosa contains deep glands whose secretory product depends on the region:
- Cardia and pyloric (antral) glands - secrete mucus and gastrin (G cells)
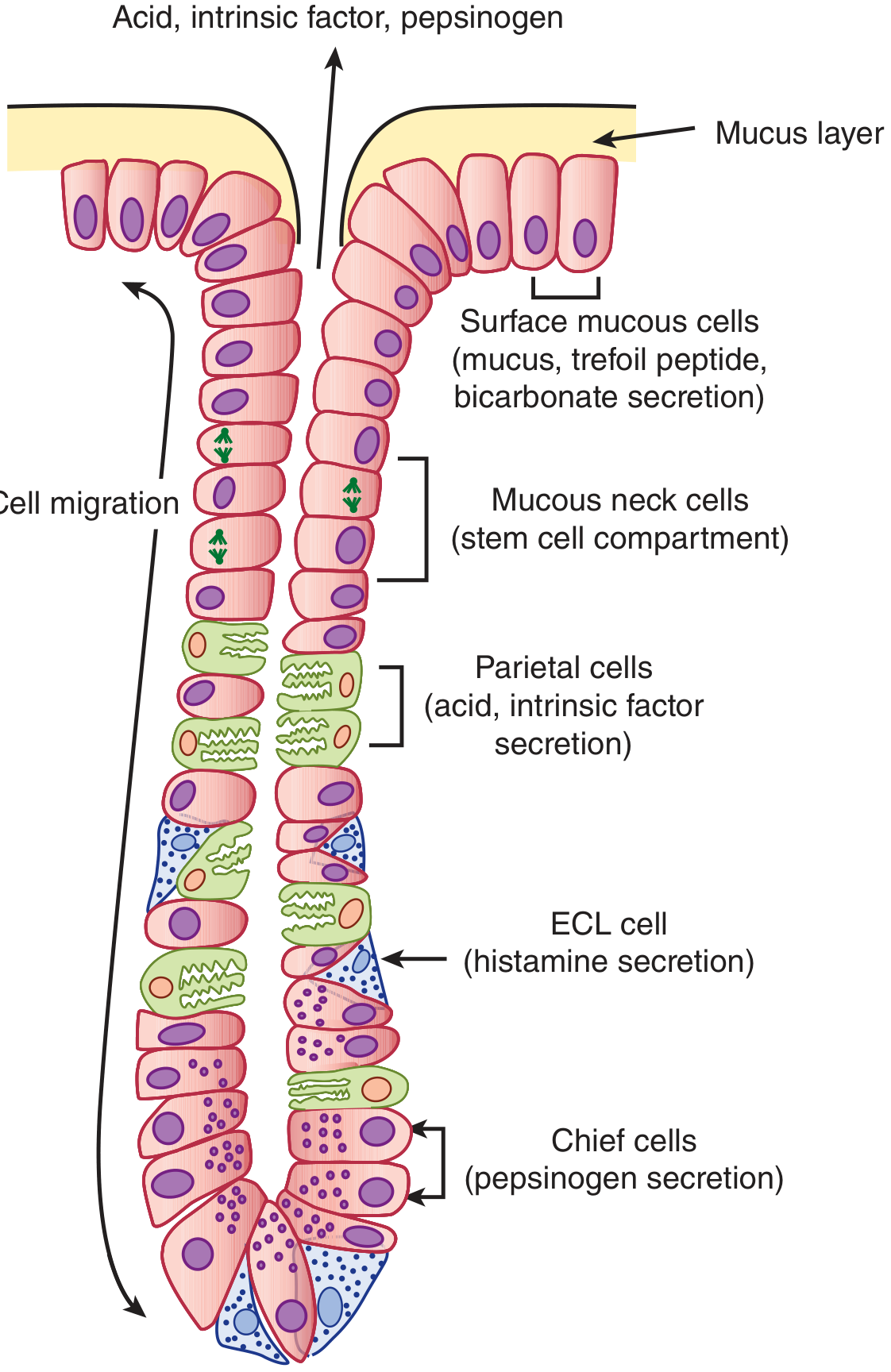
- Body/fundus glands (oxyntic glands) - contain the key secretory cells:
- Parietal cells - secrete HCl and intrinsic factor
- Chief cells - secrete pepsinogens and gastric lipase
- ECL cells - secrete histamine
- Surface mucous cells - secrete mucus, HCO3-, and trefoil peptides
Several glands drain into a common gastric pit that opens onto the mucosal surface.
2. Composition of Gastric Juice (Fasting State)
| Component | Details |
|---|---|
| Cations | Na+, K+, Mg2+, H+ (pH ~3.0) |
| Anions | Cl-, HPO42-, SO42- |
| Enzymes | Pepsins, Lipase |
| Protective | Mucus, Bicarbonate, Trefoil peptides |
| Absorption factor | Intrinsic factor (for vitamin B12) |
3. Three Primary Stimuli of Gastric Secretion
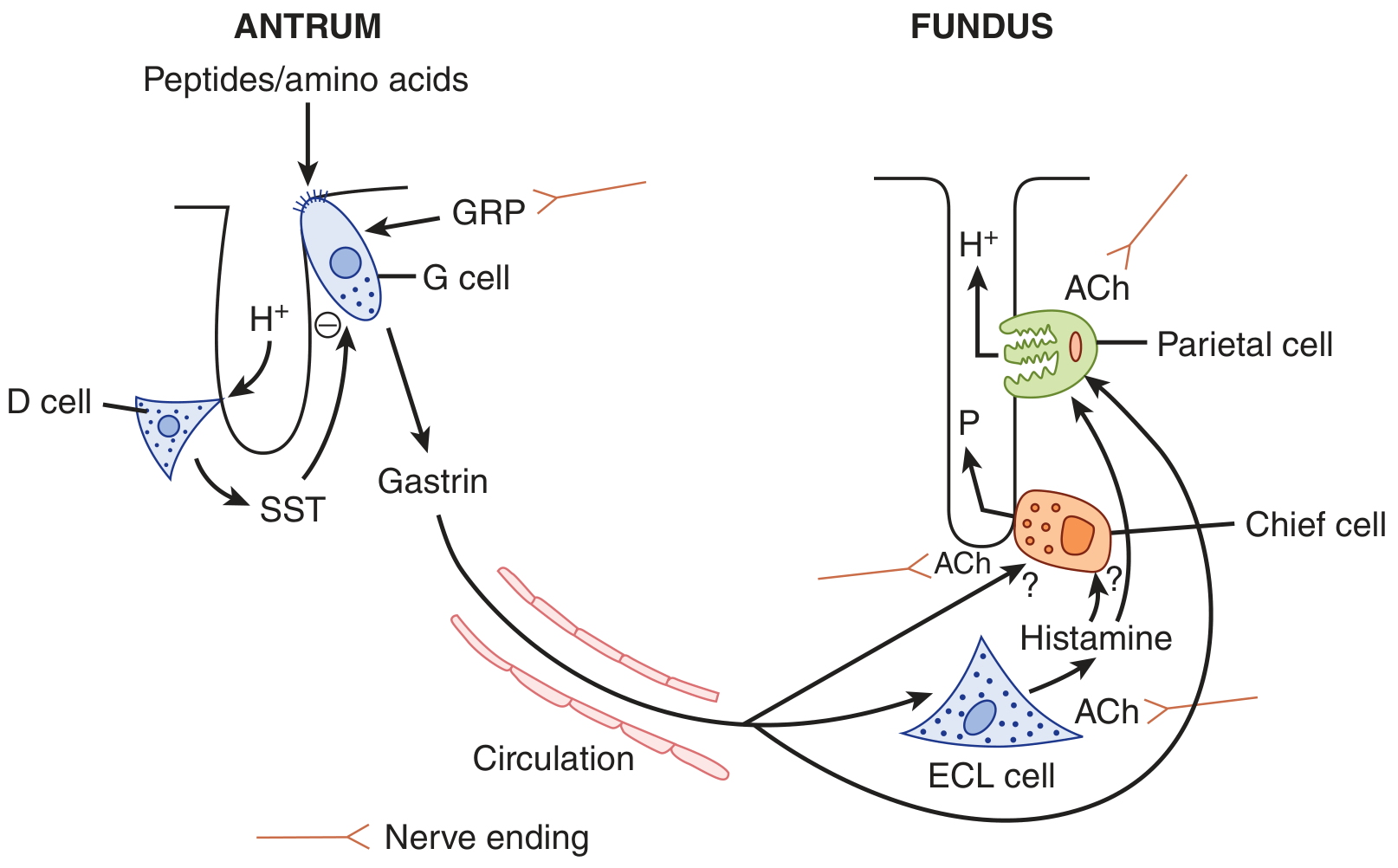
Ganong identifies three main chemical mediators, each acting via distinct receptors on parietal cells:
a) Gastrin
- Released by G cells in the antrum in response to:
- Gastrin-releasing peptide (GRP) from enteric nerve endings
- Oligopeptides/amino acids in the gastric lumen
- Travels via the bloodstream (endocrine pathway) to the fundic glands
- Acts on CCK-B receptors on parietal cells and chief cells
- Also acts on ECL cells to stimulate histamine release
b) Histamine
- Released by ECL cells in the fundic glands
- Acts via H2 receptors on parietal cells
- Second messenger: cAMP (cyclic AMP pathway)
- The most pharmacologically important stimulus - blocking H2 alone markedly suppresses secretion
c) Acetylcholine (ACh)
- Released from enteric nerve endings in the fundus
- Acts via M3 (muscarinic) receptors on parietal cells, chief cells, and ECL cells
- Second messenger: elevated cytosolic Ca2+
4. Mechanism of HCl Secretion by Parietal Cells
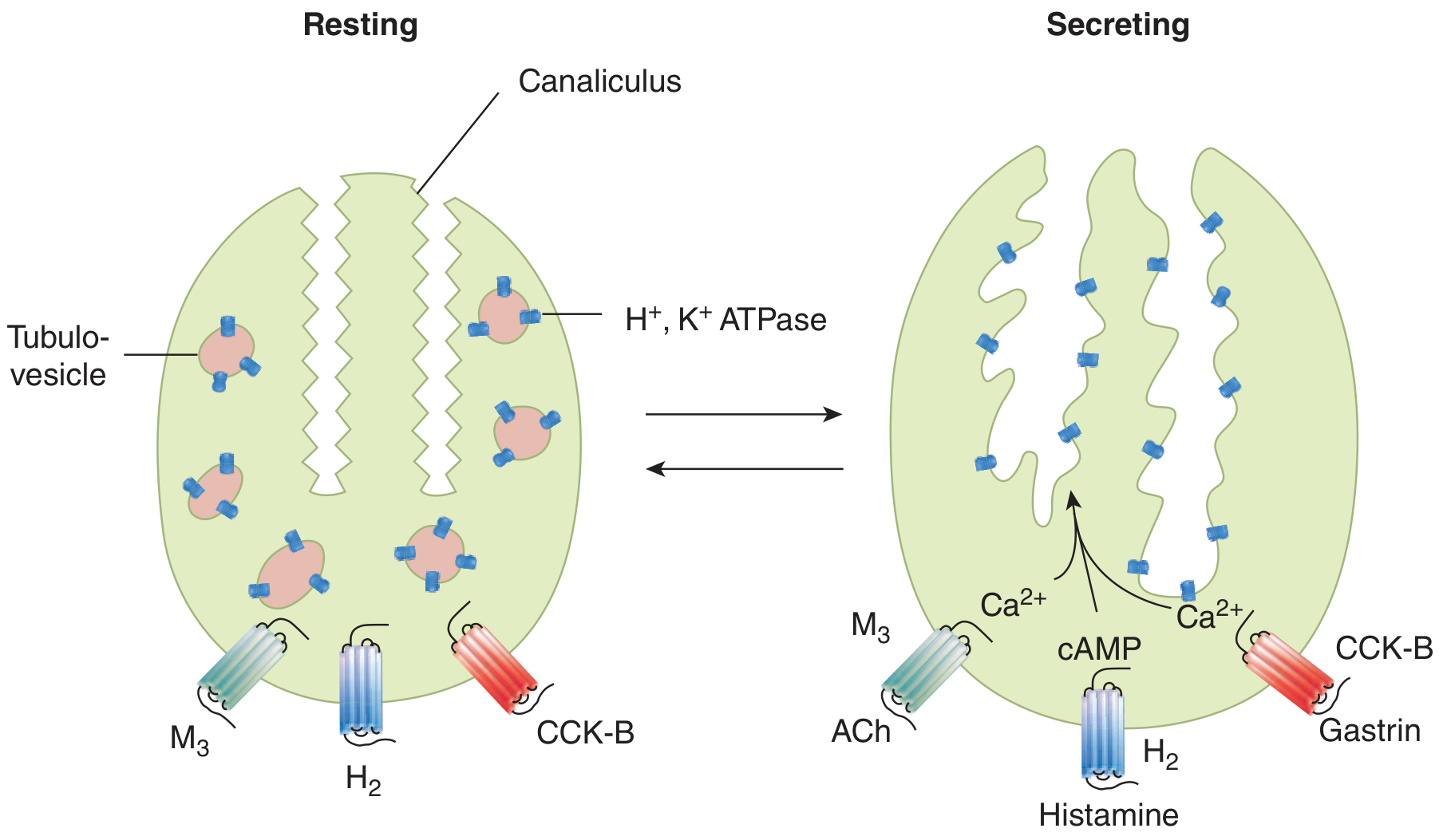
Morphologic Changes on Activation
At rest, H+K+-ATPase (proton pumps) are sequestered in intracellular membrane compartments called tubulovesicles. On stimulation:
- Tubulovesicles fuse with invaginations of the apical membrane (canaliculi)
- The apical surface area is greatly amplified
- H+K+-ATPase molecules are repositioned onto the apical membrane to begin pumping acid
Ion Transport Mechanism
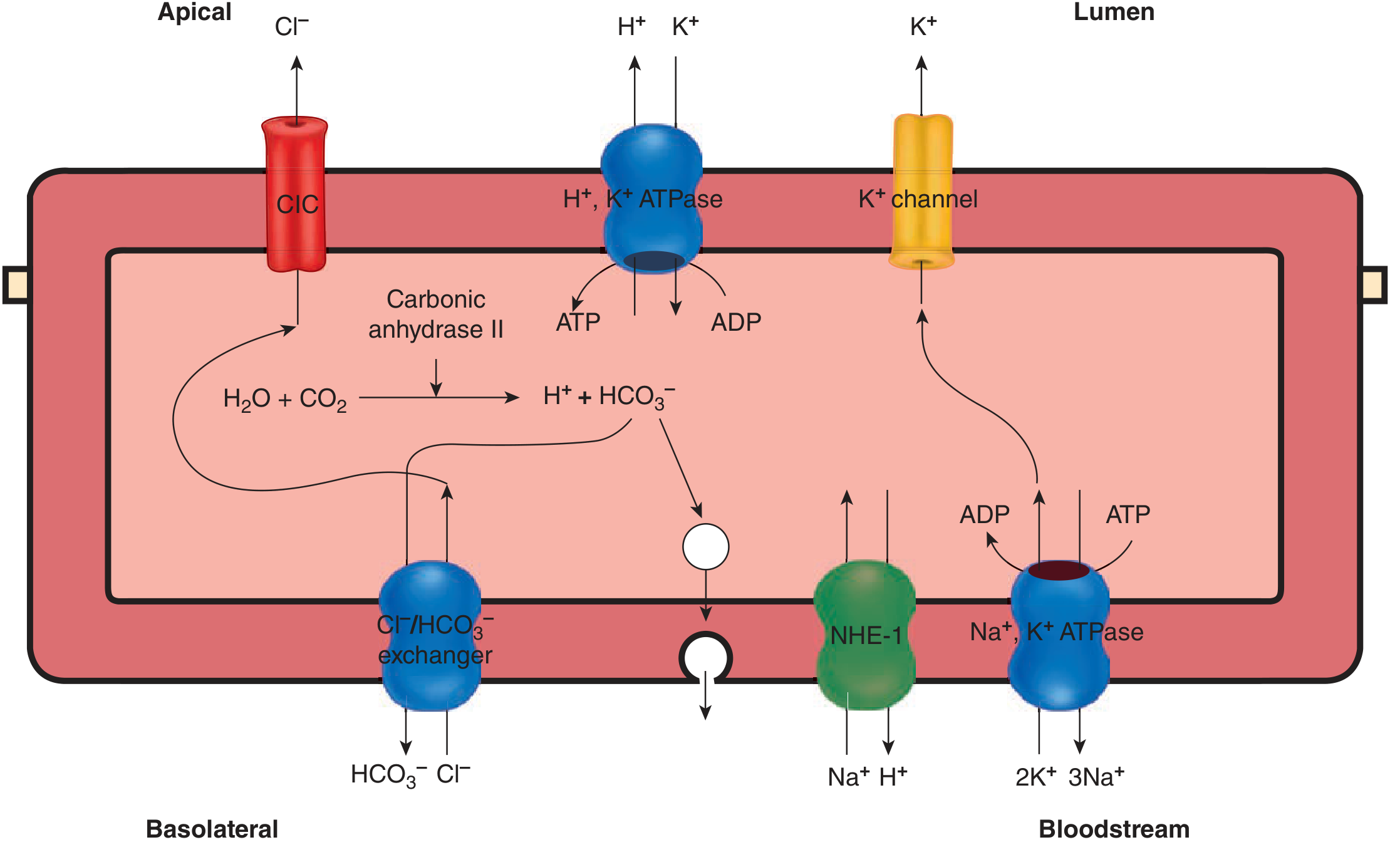
The steps are:
- H+ generation: CO2 + H2O → H+ + HCO3- (catalyzed by carbonic anhydrase II)
- H+ secretion: The H+,K+-ATPase (proton pump) on the apical membrane actively pumps H+ out into the lumen in exchange for K+ - against a concentration gradient of over 1,000,000-fold
- K+ recycling: Apical K+ channels supply K+ for the proton pump exchange
- Cl- secretion: Apical ClC chloride channels secrete Cl- into the lumen - combines with H+ to form HCl
- HCO3- handling: HCO3- is exported across the basolateral membrane via a Cl-/HCO3- exchanger into the bloodstream (the "alkaline tide") - this HCO3- later neutralizes gastric acid after it enters the duodenum
- Na+ homeostasis: Basolateral Na+,K+-ATPase and NHE-1 maintain intracellular ion balance
Intracellular Signal Transduction
| Agonist | Receptor | Second messenger | Effect |
|---|---|---|---|
| Gastrin | CCK-B | ↑ Ca2+ | Activate proton pump |
| ACh | M3 | ↑ Ca2+ | Activate proton pump |
| Histamine | H2 | ↑ cAMP | Activate proton pump |
The two signaling pathways (Ca2+ and cAMP) are synergistic - together they produce a greater-than-additive increase in secretion. This synergism means high secretion rates can be achieved with small changes in each stimulus. Therapeutically, blocking just one pathway (e.g., H2 blockade) can markedly suppress secretion.
5. Phases of Gastric Secretion
Cephalic Phase
- Initiated before food enters the stomach - anticipation, smell, sight, taste of food
- Mediated via the vagus nerve (dorsal vagal complex coordinates input from higher brain centers)
- Vagal outflow releases GRP and ACh → stimulates G cells and parietal cells
- Quantitatively limited - few local triggers yet
Gastric Phase (most significant)
- Begins when food enters the stomach
- Oligopeptides/amino acids in the lumen directly stimulate G cells to release gastrin
- Gastric distension activates stretch receptors → vago-vagal and local reflexes amplify secretion
- The meal itself buffers gastric acidity, reducing the negative feedback that would otherwise inhibit secretion
- Quantitatively the largest phase
Intestinal Phase
- Once the meal passes into the duodenum
- Duodenal factors (secretin, CCK, acidity) begin to inhibit gastric secretion
6. Inhibition of Gastric Secretion
The key feedback brake is somatostatin (SST):
- When luminal pH falls (excess acid), D cells in the antrum release somatostatin
- Somatostatin inhibits:
- G cells (stops gastrin release)
- ECL cells (stops histamine release)
- Parietal cells directly
- This is the primary mechanism terminating secretion after the meal leaves the stomach
7. Pepsinogen / Pepsin Secretion
- Chief cells secrete pepsinogen (inactive precursor)
- Pepsinogen is activated to pepsin by HCl in the gastric lumen (autocatalytic below pH 5)
- Pepsin initiates protein digestion in the stomach
- Chief cells are stimulated by ACh and gastrin (direct pathways not fully elucidated per Ganong)
8. Gastric Mucosal Defense
The stomach is protected from autodigestion by:
- Mucus-bicarbonate barrier secreted by surface mucous cells - creates an alkaline microenvironment adjacent to the epithelium
- Trefoil peptides - stabilize the mucus-bicarbonate layer
- Prostaglandins - stimulate mucus and HCO3- secretion, maintain mucosal blood flow
- Tight junctions between epithelial cells - gastric mucosal barrier preventing back-diffusion of H+
- Rapid cell turnover - damaged cells are quickly replaced
9. Peptic Ulcer Disease (PUD)
Ganong explains PUD as a breakdown of the mucosal barrier that normally prevents autodigestion:
Causes
1. Helicobacter pylori infection
- The most common cause
- H. pylori disrupts the mucus-bicarbonate barrier
- Creates a local environment favoring acid injury
2. NSAIDs (aspirin and other non-steroidal anti-inflammatory drugs)
- Inhibit cyclooxygenase (COX) enzymes
- Reduce prostaglandin synthesis
- Consequently decrease mucus and HCO3- secretion
- Impair mucosal defense without necessarily increasing acid output
3. Prolonged hypersecretion of acid
- Example: Zollinger-Ellison syndrome
- Caused by gastrinomas (gastrin-secreting tumors)
- Most gastrinomas are found in the pancreas, though some occur in the stomach and duodenum
- Gastrin causes prolonged, massive acid hypersecretion
- Results in severe, treatment-resistant peptic ulcers
10. Treatment of Peptic Ulcer (Therapeutic Highlights from Ganong)
| Drug/Approach | Mechanism |
|---|---|
| Proton pump inhibitors (PPIs) e.g. omeprazole | Irreversibly inhibit H+,K+-ATPase on parietal cells - block the final common pathway of acid secretion |
| H2-receptor antagonists | Block histamine H2 receptors on parietal cells - reduce cAMP-mediated acid secretion |
| Antibiotics | Eradicate H. pylori if present |
| Misoprostol | Prostaglandin E1 agonist - used for NSAID-induced ulcers (when NSAID cannot be stopped) - restores mucus and HCO3- secretion |
| Surgical removal | Gastrinomas in Zollinger-Ellison syndrome can sometimes be removed |
Summary Diagram of Regulation
The regulation of gastric secretion is best summarized as a 3-phase, 3-agonist system with negative feedback:
- Three phases: cephalic (vagal/neural) → gastric (hormonal + neural) → intestinal (inhibitory)
- Three agonists converge on parietal cells: gastrin (via CCK-B, Ca2+), histamine (via H2, cAMP), ACh (via M3, Ca2+)
- Synergism between pathways enables high secretion at low individual stimulus concentrations
- Somatostatin from D cells provides the critical acid-feedback brake
- The mucosal barrier (mucus, HCO3-, prostaglandins) protects the stomach from its own acid
All content from: Ganong's Review of Medical Physiology, 26th Edition, Chapter 25 (Digestion, Absorption, & Nutritional Principles), pp. 459-462.
This is a shared conversation. Sign in to Orris to start your own chat.