Cerebellum and cerebellar disorder physiology mbbs 1st year
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have all the material needed for a comprehensive MBBS 1st year answer. Let me compose the full response.
Cerebellum and Cerebellar Disorders - Physiology (MBBS 1st Year)
1. Introduction
The cerebellum ("little brain") is a foliated structure lying in the posterior fossa, dorsal to the pons and medulla. It weighs only ~10% of the cerebral cortex but its surface area is about 75% of it. The cerebellum does not initiate movement - instead, it acts as a comparator and error-correcting organ that regulates the rate, range, force, and direction of movements (collectively called synergy).
Key functions:
- Coordination of voluntary movement
- Planning and execution of movement
- Maintenance of posture and balance
- Coordination of head and eye movements
- Motor learning
Costanzo Physiology 7th Ed., p. 113-115
2. Gross Anatomy and Divisions
The cerebellum is divided into three functional divisions based on dominant input:
| Division | Dominant Input | Function |
|---|---|---|
| Vestibulocerebellum (flocculonodular lobe) | Vestibular organs | Balance and eye movements |
| Spinocerebellum (vermis + intermediate hemisphere) | Spinal cord | Synergy (coordination) of movement |
| Pontocerebellum (lateral hemispheres) | Cerebral cortex via pontine nuclei | Planning and initiation of movements |
Three pairs of peduncles connect the cerebellum to the brainstem:
- Superior cerebellar peduncle - mainly EFFERENT; projects to red nucleus and thalamus
- Middle cerebellar peduncle - entirely AFFERENT; from contralateral pontine nuclei
- Inferior cerebellar peduncle - mixed; afferents from brainstem/spinal cord + efferents to vestibular nuclei
Four deep cerebellar nuclei (from medial to lateral): Fastigial, Globose, Emboliform, Dentate. The globose and emboliform are sometimes grouped as the interpositus nucleus.
Ganong's Review of Medical Physiology, 26th Ed., p. 253-254
3. Layers of the Cerebellar Cortex
The cerebellar cortex has three layers and five cell types:
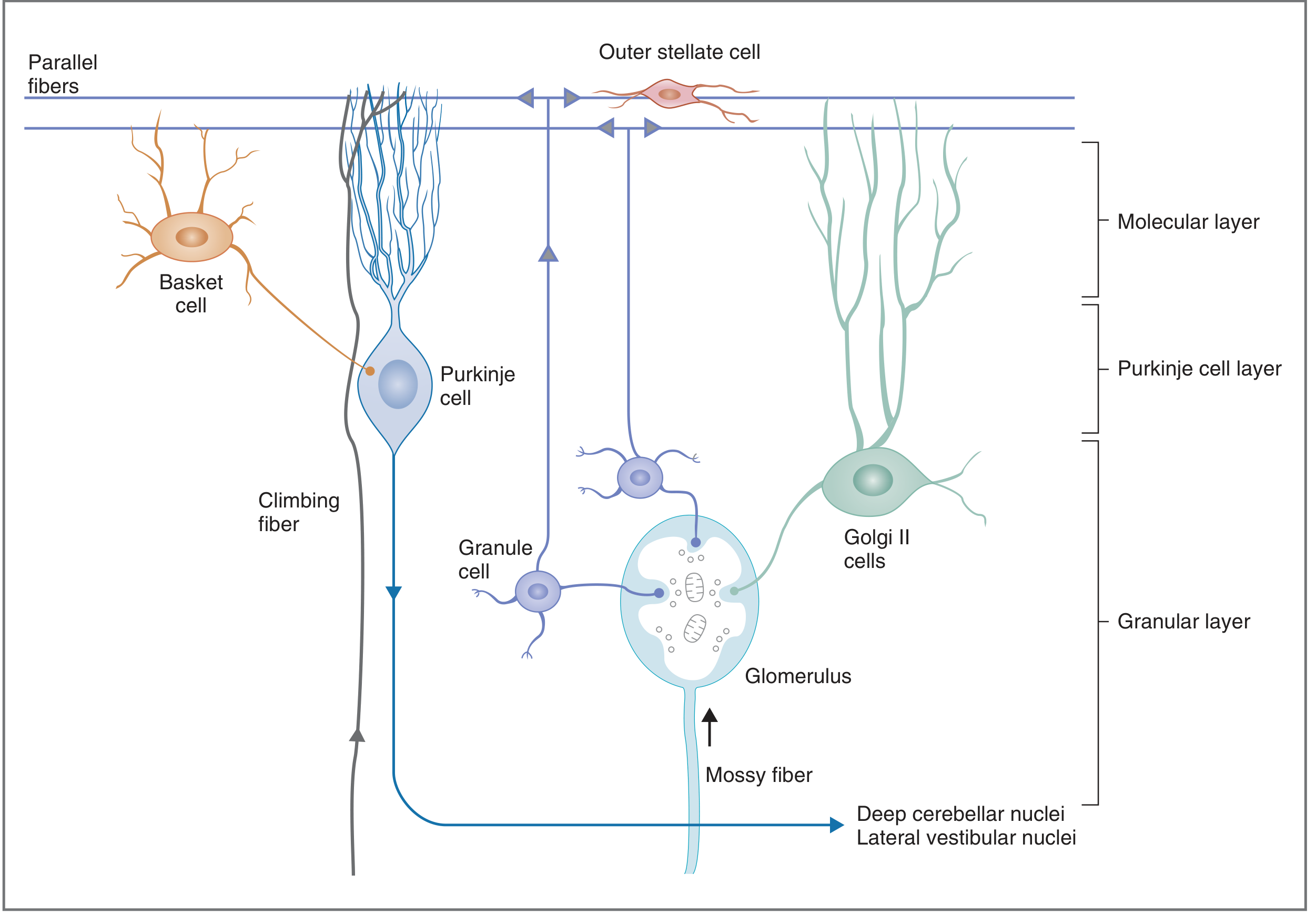
Fig. Cross-section of cerebellar cortex showing cell types and connections - Costanzo Physiology
Layers (outer to inner):
1. Molecular Layer (outermost)
- Contains: outer stellate cells, basket cells, dendrites of Purkinje and Golgi II cells, and parallel fibers (axons of granule cells)
- Parallel fibers run perpendicular to the flattened Purkinje dendrites
2. Purkinje Cell Layer (middle)
- Contains only Purkinje cells - the largest neurons in the CNS
- Purkinje cells are the sole output of the cerebellar cortex
- Their output is always inhibitory (neurotransmitter = GABA)
3. Granular Layer (innermost)
- Contains: granule cells, Golgi II cells, and glomeruli
- Mossy fibers synapse on granule cell dendrites at glomeruli
Costanzo Physiology 7th Ed., p. 114
4. Input to the Cerebellar Cortex
Two excitatory input systems reach the cerebellar cortex:
A. Mossy Fiber System (majority of input)
- Sources: vestibulocerebellar, spinocerebellar, and pontocerebellar afferents
- Synapse on granule cells at glomeruli
- Granule cells send axons up → bifurcate in molecular layer → become parallel fibers
- Parallel fibers synapse on Purkinje cells (up to 250,000 parallel fiber inputs per Purkinje cell!)
- Produce simple, single-action-potential spikes (simple spikes)
B. Climbing Fiber System
- Origin: inferior olive of the medulla
- Project DIRECTLY onto Purkinje cell dendrites (each Purkinje cell receives only ONE climbing fiber, but that fiber makes 2000-3000 synapses on it)
- Single action potential produces multiple excitatory bursts = complex spikes
- Play a role in cerebellar learning - climbing fiber activity increases when a new movement is being learned
Costanzo Physiology 7th Ed., p. 114-115; Ganong's 26th Ed., p. 257-258
5. Cerebellar Interneurons
All interneurons except granule cells are inhibitory:
| Cell | Effect on Purkinje Cell |
|---|---|
| Granule cells | Excitatory (via parallel fibers) |
| Basket cells | Inhibitory |
| Stellate cells | Inhibitory |
| Golgi II cells | Inhibit granule cells → reduce excitatory drive to Purkinje cells |
6. Output Circuit
Cerebellar cortex → Purkinje cells (inhibitory, GABA)
↓
Deep cerebellar nuclei (mainly dentate)
↓
Superior cerebellar peduncle → crosses → Red nucleus / Thalamus (VL)
↓
Motor cortex → Corticospinal tract → crosses → contralateral spinal cord
The double-crossing explains why cerebellar lesions produce IPSILATERAL signs - the cerebellar output crosses once going up, and the corticospinal tract crosses again going down. Net result: right cerebellar lesion → right-sided (ipsilateral) ataxia.
7. The Cerebellum as an Error-Corrector
The cerebellum receives:
- Sensory feedback (proprioception from spinal cord via spinocerebellar tracts)
- Motor commands (from cerebral cortex via cortico-ponto-cerebellar pathway)
- Vestibular information (balance/position from inner ear)
It compares the "intended" movement (motor command) with the "actual" movement (sensory feedback) and sends corrective signals to adjust timing and amplitude. This is the basis of cerebellar motor learning.
8. Disorders of the Cerebellum
Cerebellar lesions produce a clinical syndrome characterized by errors in rate, range, force, and direction of movement. Signs are ipsilateral to the lesion.
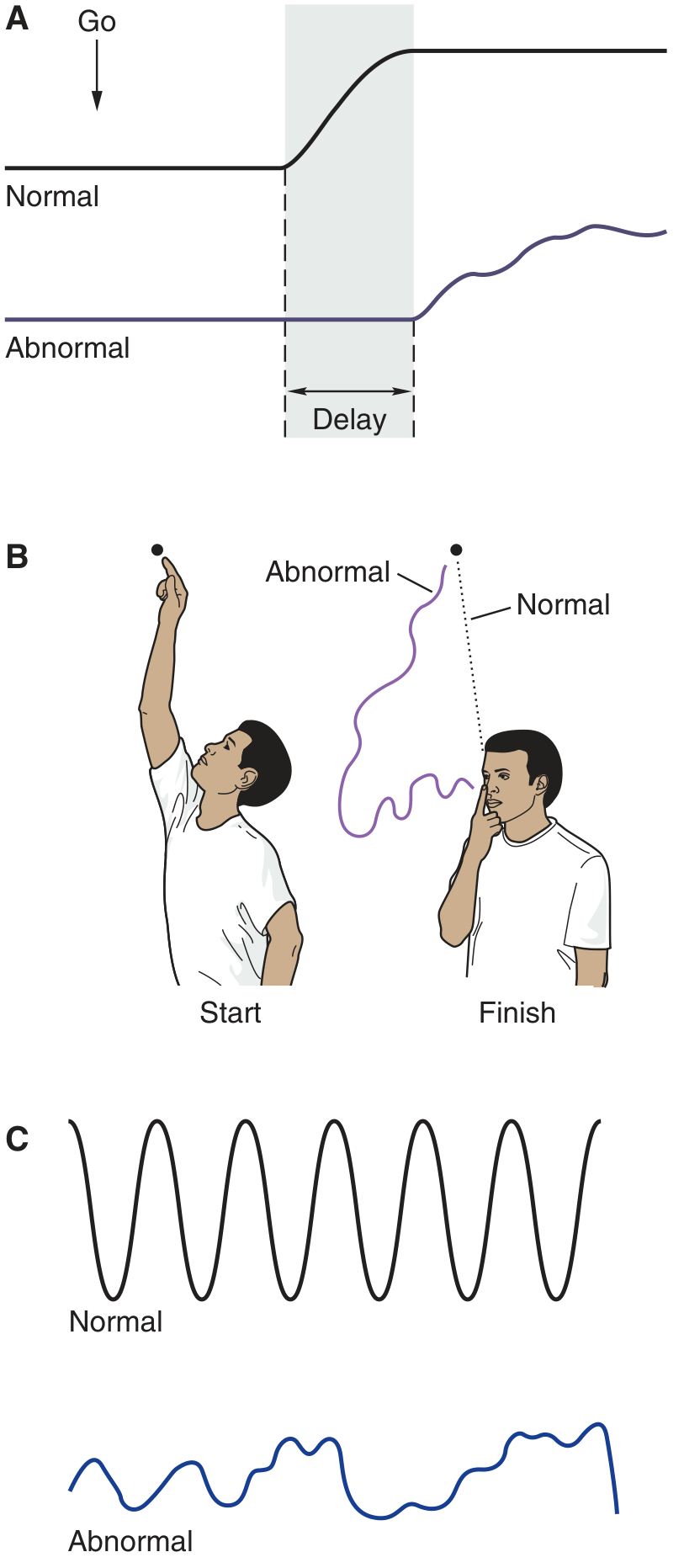
Fig. Typical defects associated with cerebellar disease - Ganong's Review of Medical Physiology
A. ATAXIA (Most Prominent Feature)
- Incoordination due to errors in rate, range, force, and direction of movement
- Gait ataxia: wide-based, unsteady, "drunken" gait
- Limb ataxia: clumsy, poorly coordinated limb movements
B. DYSMETRIA
- Inability to judge distance accurately
- Limb overshoots (hypermetria) or undershoots (hypometria) the target
- Tested by: finger-nose test, heel-shin test
C. INTENTION TREMOR (Kinetic/Ataxic Tremor)
- Tremor that appears during voluntary movement and worsens as the limb approaches its target
- Perpendicular oscillation around the direction of movement
- Absent at rest (unlike the resting tremor of Parkinson disease)
- Mechanism: dysmetria initiates corrective action, which overshoots → oscillates back and forth
D. DYSDIADOCHOKINESIA
- Inability to perform rapid, alternating movements (e.g., pronation-supination of the forearm)
- Reflects the failure of normal agonist-antagonist reciprocal inhibition
E. HYPOTONIA
- Decreased muscle tone, especially prominent with acute cerebellar lesions
- Loss of cerebellar facilitation of alpha motor neurons reduces resting tone
F. DYSARTHRIA (Scanning Speech)
- Slurred, irregular, slow speech
- Results from incoordination of the muscles of articulation (same principle as limb ataxia)
G. NYSTAGMUS
- Involuntary rhythmic eye movements
- Caused by involvement of the vestibulocerebellum (flocculonodular lobe) and its connections with vestibular nuclei
H. REBOUND PHENOMENON (Holmes Test)
- If a person with cerebellar disease flexes the forearm against resistance and the resistance is suddenly removed, they cannot stop the arm from flying upward (hitting themselves)
- Normally, the antagonist muscles check the movement; cerebellar damage impairs this braking
I. DECOMPOSITION OF MOVEMENT
- A smooth multi-joint movement is broken into jerky, sequential components
- E.g., reaching for a glass appears as shoulder movement, then elbow, then wrist - one at a time instead of fluid
J. DELAYED INITIATION
- There is a prolonged interval between the commanded act and actual movement onset
9. Summary of Signs by Region Affected
| Cerebellar Region | Clinical Feature |
|---|---|
| Vestibulocerebellum (flocculonodular lobe) | Truncal ataxia, gait ataxia, nystagmus, vertigo |
| Spinocerebellum (vermis/intermediate) | Gait ataxia, truncal instability |
| Pontocerebellum (lateral hemispheres) | Ipsilateral limb ataxia, dysmetria, intention tremor, dysdiadochokinesia |
10. Comparison: Cerebellar vs. Basal Ganglia Disorders
| Feature | Cerebellar Disease | Parkinson Disease (Basal Ganglia) |
|---|---|---|
| Tremor | Intention tremor (during movement) | Resting tremor (at rest, "pill-rolling") |
| Tone | Hypotonia | Rigidity |
| Gait | Wide-based, ataxic, "drunken" | Shuffling, festinant, stooped |
| Initiation | Delayed | Slow (bradykinesia) |
| Speech | Scanning (cerebellar dysarthria) | Soft, monotone (hypokinetic dysarthria) |
| Coordination | Severely impaired | Relatively preserved |
Key Mnemonics
DANISH - signs of cerebellar disease:
- Dysdiadochokinesia
- Ataxia
- Nystagmus
- Intention tremor
- Scanning speech (dysarthria)
- Hypotonia
Sources: Costanzo Physiology 7th Ed., pp. 113-115; Ganong's Review of Medical Physiology 26th Ed., pp. 253-258; Adams and Victor's Principles of Neurology 12th Ed., pp. 127-130; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.