Development of lung for md exams 10 marks answer from fishman only
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed. Let me compose the full 10-mark exam answer.
Development of the Lung
Source: Fishman's Pulmonary Diseases and Disorders (Chapter 105)
Introduction
Lung development begins at 4 weeks of gestation and continues through young adulthood. It involves a complex series of reciprocal interactions between mesoderm-derived mesenchyme and endoderm-derived epithelium. Any disruption at any stage leads to anatomic and physiologic abnormalities ranging from asymptomatic incidental findings to severe postnatal respiratory distress.
Embryological Origin
- The lung originates from the laryngotracheal groove of the endoderm, located at the fourth pharyngeal arch.
- The splanchnic mesoderm provides muscular and cartilaginous covering to the lung and forms the visceral pleura.
- The somatic mesoderm forms the parietal pleura.
- The laryngotracheal groove outpouches from the foregut, forming the respiratory diverticulum (tracheal bud), which separates from the esophagus.
- The tracheal bud branches into two primary bronchi (left and right), then into secondary (lobar) bronchi: three on the right (for 3 lobes) and two on the left (for 2 lobes) by 5 weeks of gestation.
Five Stages of Lung Development
Lung development is divided into five stages:
| Stage | Gestational Age | Key Events |
|---|---|---|
| Embryonic | 4–5 weeks | Tracheal bud, primary/secondary bronchi |
| Pseudoglandular | 5–16 weeks | Conducting airways to terminal bronchioles; mesenchymal differentiation |
| Canalicular | 16–26 weeks | Type I pneumocytes; surfactant lamellar bodies; angiogenesis |
| Saccular | 26 weeks to term | Primary sacculi; double-capillary septa; smooth muscle differentiation |
| Alveolar | Postnatal | Secondary septation; alveolar maturation |
1. Embryonic Stage (4–5 weeks)
- Laryngotracheal groove outpouches to form the respiratory diverticulum.
- Tracheal bud separates from the esophagus.
- Primary bronchi form; secondary (lobar) bronchi develop by 5 weeks.
2. Pseudoglandular Stage (5–16 weeks)
- The lung grows laterally and caudally on exposure to splanchnic mesoderm.
- Conducting airways branch progressively until terminal bronchioles (16th to 25th generation) are formed by 16 weeks.
- The mesenchymal tissue begins to differentiate into:
- Ciliated columnar epithelial cells
- Goblet cells
- Type II pneumocytes (precursors)
- This stage marks the transition between conducting and respiratory airways.
- Alveolar myofibroblasts surround distal lung epithelial tubules and buds during this stage; they are essential for later secondary septation.
3. Canalicular Stage (16–26 weeks)
- The epithelium differentiates into type I pneumocytes (alveolar cells) - the primary structural cells responsible for gas exchange.
- Extensive angiogenesis occurs, forming the capillary network surrounding alveolar cells.
- Lamellar bodies (inclusion bodies) form within type II pneumocytes - the primary sites for surfactant storage.
- Conducting airways continue to elongate and widen, giving a canalicular appearance.
- A fetus born at this stage may survive with intensive respiratory support, as minimal gas exchange surface is present.
4. Saccular Stage (26 weeks to term)
- Progressive maturation of type I and type II pneumocytes.
- Decrease in interstitial tissue leads to the formation of air spaces (primary sacculi) - the location of future gas exchange.
- Exponential growth in primary sacculi with formation of the primary septum between each saccular unit.
- Primary septa contain a double-layered capillary network.
- Mesenchymal tissue differentiates into:
- Smooth muscle cells
- A fibroelastic network of collagen fibrils - the foundation for alveolarization.
5. Alveolar (Alveolarization) Stage (Postnatal)
- Secondary septation begins: secondary septa arise from primary septa, subdividing the primary sacculi into alveoli.
- The double capillary loops fuse into a single capillary loop in the definitive alveolar wall.
- Alveolar myofibroblasts play a key role - their absence results in deficient secondary septation and failure of alveolar development.
- The alveolar surface area increases dramatically postnatally.
- Alveolarization continues until approximately 8 years of age in humans.
Role of Fetal Lung Fluid
- Fetal lung fluid is secreted by the lung epithelium and plays a mechanical role in maintaining lung expansion.
- Adequate fetal lung fluid volume is critical for normal lung growth.
- Oligohydramnios (reduced amniotic fluid, e.g., from renal agenesis) causes pulmonary hypoplasia due to reduced mechanical stretch stimulus on the developing lung.
Molecular Mechanisms
- Lung morphogenesis depends on reciprocal signaling between mesenchyme and epithelium.
- Key molecular regulators include:
- FGF (Fibroblast Growth Factor) signaling - branching morphogenesis
- Wnt signaling - epithelial-mesenchymal crosstalk
- Shh (Sonic Hedgehog) - separation of trachea from esophagus and airway patterning
- TGF-beta - mesenchymal differentiation and myofibroblast activation
- Disruption of these pathways leads to congenital anomalies such as tracheo-esophageal fistula, bronchial atresia, and CPAM.
Classification of Developmental Disorders
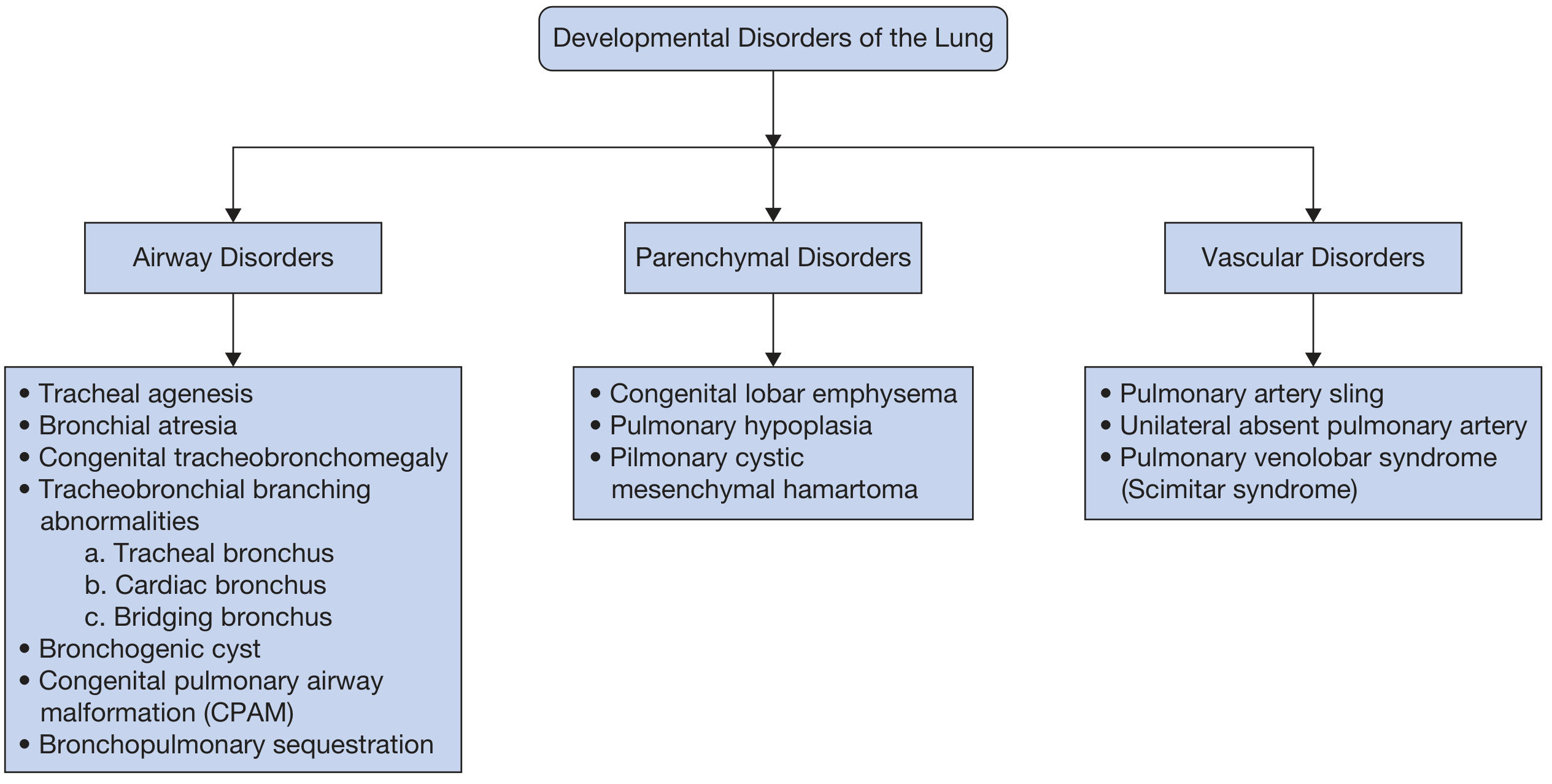
Developmental disorders are classified as:
- Airway disorders: Tracheal agenesis, bronchial atresia, congenital tracheobronchomegaly (Mounier-Kuhn), bronchogenic cyst, CPAM, bronchopulmonary sequestration
- Parenchymal disorders: Congenital lobar emphysema, pulmonary hypoplasia, pulmonary cystic mesenchymal hamartoma
- Vascular disorders: Pulmonary artery sling, unilateral absent pulmonary artery, Scimitar syndrome
Clinical Relevance
- Prenatal ultrasonography and Doppler are first-line screening tools.
- Some anomalies resolve spontaneously before birth; others persist with a spectrum of severity.
- Asymptomatic anomalies often discovered incidentally in adults may be misidentified as malignant or infectious lesions on chest imaging.
- A clinico-radiologic approach is needed for accurate identification and management.
Reference: Fishman's Pulmonary Diseases and Disorders, 5th Edition - Chapter 105 (Deshwal & Ghosh), "Development of the Lung" and associated sections on Myofibroblasts in Lung Development and Molecular Mechanisms.
Give combined answer from murray
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I have very comprehensive content from Murray. Let me now compile the full combined answer integrating both Fishman's and Murray & Nadel's.
Development of the Lung
Combined Answer - Fishman's Pulmonary Diseases & Disorders (Ch. 105) + Murray & Nadel's Textbook of Respiratory Medicine (Ch. 2)
Introduction
The human lung has an estimated surface area of approximately 130 m² and contains approximately 480 million alveoli for gas exchange. Gas reaches these alveoli through an elaborate branched network of conducting airways, running in parallel with the pulmonary vasculature. Because gas exchange must begin immediately at first breath, the developmental program leading to a functional lung is critical to neonatal survival.
Human lung development begins at approximately 4 weeks of gestation and continues well into young adulthood - with newer evidence showing alveolar addition continues into the third decade of life. Any disruption leads to a spectrum of disease: from neonatal respiratory distress to increased susceptibility to chronic respiratory conditions in adulthood.
Embryological Origin
- The lung arises from the laryngotracheal groove of the endoderm at the fourth pharyngeal arch (Fishman).
- Epithelial cells arise from the endoderm; mesenchymal and endothelial cells arise from the mesoderm (Murray).
- The splanchnic mesoderm provides muscular and cartilaginous covering and forms the visceral pleura.
- The somatic mesoderm forms the parietal pleura.
- The laryngotracheal groove outpouches from the foregut as the respiratory diverticulum (tracheal bud), which separates from the esophagus.
- The tracheal bud divides into two primary bronchi, then secondary (lobar) bronchi (3 right, 2 left) by 5 weeks of gestation.
Five Stages of Lung Development
| Stage | Timing | Key Events |
|---|---|---|
| Embryonic | 4–5 weeks | Tracheal bud; primary and secondary bronchi |
| Pseudoglandular | 5–16 weeks | Branching to terminal bronchioles; early cell differentiation |
| Canalicular | 16–26 weeks | Type I pneumocytes; angiogenesis; surfactant lamellar bodies |
| Saccular | 26 weeks to term | Primary sacculi; double-capillary septa; smooth muscle differentiation |
| Alveolar | Postnatal (to ~20s) | Secondary septation; alveologenesis; single capillary loop maturation |
Stage 1: Embryonic Stage (4–5 weeks gestation)
- The laryngotracheal groove outpouches from the foregut to form the respiratory diverticulum.
- Tracheal bud elongates and separates from the esophagus - disruption of Sonic Hedgehog (Shh) signaling at this step leads to tracheo-esophageal fistula.
- The bud branches into left and right primary bronchi, then into secondary (lobar) bronchi by 5 weeks.
- The primary lung field is specified by NKX2.1 (TTF-1) transcription factor - the master regulator of lung identity (Murray).
Stage 2: Pseudoglandular Stage (5–16 weeks)
- The lung grows laterally and caudally under the influence of the splanchnic mesoderm.
- Conducting airways branch progressively until terminal bronchioles (16th to 25th generation) are formed by 16 weeks.
- The lung at this stage histologically resembles a gland - hence "pseudoglandular."
- Mesenchymal tissue differentiates into:
- Ciliated columnar epithelial cells
- Goblet cells (secretory)
- Club cells (formerly Clara cells)
- Precursors of type II pneumocytes
- Submucosal glands are prevalent in the human conducting airways and are lined by serous and goblet cells, with myoepithelial cells in the basal layer (Murray).
- Alveolar myofibroblasts surround distal epithelial tubules and buds during this stage; they are essential for later secondary septation. Their absence causes deficient alveolar development (Fishman).
- Key signaling: FGF10-FGFR2 axis drives branching morphogenesis; Wnt signaling regulates epithelial-mesenchymal crosstalk.
Stage 3: Canalicular Stage (16–26 weeks)
- Epithelium differentiates into type I pneumocytes (AT1 cells) - the primary structural cells for gas exchange, covering ~95% of alveolar surface area.
- Type II pneumocytes (AT2 cells) develop and form lamellar bodies - organelles that store and secrete pulmonary surfactant (Murray).
- Extensive angiogenesis produces the capillary network surrounding alveolar cells - driven by VEGF signaling.
- Conducting airways elongate and widen, giving the canalicular appearance on histology.
- Airway epithelial cells begin to differentiate at midgestation, while alveolar epithelial cells differentiate near the end of gestation - in time to support gas exchange at birth (Murray).
- A fetus born at 24–25 weeks may survive with respiratory support as minimal gas exchange surface exists.
Stage 4: Saccular Stage (26 weeks to term)
- Progressive maturation of type I and type II pneumocytes with decreasing interstitial tissue.
- Primary sacculi form - the precursors of future alveoli; these are the sites of gas exchange.
- Exponential growth in primary sacculi with primary septa forming between each unit.
- Primary septa at this stage contain a double-layered capillary network (characteristic feature).
- Mesenchymal tissue further differentiates into:
- Smooth muscle cells
- Fibroelastic network of collagen fibrils - the structural foundation for alveolarization.
- Surfactant production increases, becoming sufficient for postnatal respiration around 35 weeks (clinical relevance for RDS in prematurity).
Stage 5: Alveolar Stage (Postnatal)
- Secondary septation: secondary septa arise from primary septa, subdividing primary sacculi into true alveoli.
- The double capillary loops of the primary septa fuse into a single capillary loop in the mature alveolar wall - increasing gas exchange efficiency.
- AT2 cells serve as progenitors and can give rise to AT1 cells that cover the alveolar surface (Murray).
- Alveolar myofibroblasts (present during alveologenesis) are absent in the adult lung - their clearance after septation is an active process (Fishman).
- Murray notes: the conventional view suggests alveolar formation is complete by 6–7 years of age, but recent studies show new alveoli continue to be added into the 20s in humans.
- 95% of the total alveolar surface area is added after birth (Murray).
Cell Types of the Mature Lung (Murray)
There are more than 40 resident cell types in the mature lung:
Airway epithelium:
- Goblet cells and Club cells - secretory
- Ciliated cells - mucociliary clearance
- Basal cells - progenitors that replace damaged luminal cells after injury
- Rare cells: pulmonary neuroendocrine cells, ionocytes, tuft cells
Alveolar epithelium:
- AT2 cells - produce surfactant; serve as progenitors for AT1 cells
- AT1 cells - cover 95% of alveolar surface; primary gas exchange interface
Mesenchyme:
- Myofibroblasts, matrix fibroblasts, lipofibroblasts, pericytes (distinguished by single-cell RNA sequencing)
Molecular Regulation of Lung Development
| Signal | Role |
|---|---|
| NKX2.1 / TTF-1 | Master transcription factor specifying lung identity |
| SOX2 | Proximal airway epithelial identity |
| SOX9 | Distal progenitor cell maintenance in branching tips |
| FGF10 / FGFR2 | Epithelial-mesenchymal signaling; branching morphogenesis |
| Shh (Sonic Hedgehog) | Tracheo-esophageal separation; airway patterning |
| Wnt signaling | Epithelial-mesenchymal crosstalk; cell fate decisions |
| VEGF | Pulmonary angiogenesis; capillary network formation |
| TGF-beta | Mesenchymal differentiation; myofibroblast activation |
Role of Fetal Lung Fluid
- Fetal lung fluid is secreted by the lung epithelium and fills the nascent airways.
- It exerts mechanical stretch on the developing epithelium, which is a key stimulus for normal lung growth.
- Oligohydramnios (e.g., from renal agenesis - Potter sequence) reduces amniotic fluid, limits fetal breathing movements, and causes pulmonary hypoplasia due to the loss of mechanical distension.
Pulmonary Vasculature Development (Murray)
- Pulmonary endothelial cells give rise to three distinct vascular networks:
- Pulmonary arteries (carrying deoxygenated blood to lungs)
- Pulmonary veins (carrying oxygenated blood from lungs)
- Bronchial circulation (systemic supply to airway walls)
- The pulmonary circulation is unique - opposite to all other tissues in the body in carrying deoxygenated blood to, and oxygenated blood from, the organ.
Developmental Disorders
Classified into three groups (Fishman):
Airway Disorders: Tracheal agenesis, bronchial atresia, congenital tracheobronchomegaly (Mounier-Kuhn syndrome), tracheo-esophageal fistula, bronchogenic cyst, CPAM, bronchopulmonary sequestration
Parenchymal Disorders: Congenital lobar emphysema, pulmonary hypoplasia, pulmonary cystic mesenchymal hamartoma
Vascular Disorders: Pulmonary artery sling, unilateral absent pulmonary artery, Scimitar syndrome (pulmonary venolobar syndrome)
Clinical Significance
- Preterm birth and BPD (Bronchopulmonary Dysplasia): disruption of the saccular/alveolar stages leads to arrested alveolar development, poor gas exchange in infancy persisting into adulthood.
- Surfactant deficiency: prematurity interrupts canalicular/saccular maturation - basis of Respiratory Distress Syndrome (RDS) in neonates.
- Reduced early lung capacity - from any cause - leads to premature decline of respiratory function during aging and increased susceptibility to COPD (Murray).
- Many congenital anomalies remain subclinical and are discovered incidentally in adulthood, where they are often misidentified as malignant or infectious lesions on chest imaging.
Emerging Technologies (Murray)
- iPSC-derived lung cells: patient-derived induced pluripotent stem cells differentiated into lung lineages for disease modeling and therapy.
- Lung Organoids: 3D miniature lung structures recapitulating key developmental steps.
- CRISPR/Cas9: disease mutation correction in iPSCs and in vivo editing of lung cells; in utero lung editing achieved in animal models - promising for cystic fibrosis.
- Single-cell RNA sequencing (scRNA-seq): revealed heterogeneity within morphologically similar cell types (e.g., AT2 subpopulations, multiple mesenchymal subtypes); identified rare ionocytes and tuft cells.
References:
- Fishman's Pulmonary Diseases and Disorders, 5th Ed., Chapter 105 - Deshwal & Ghosh
- Murray & Nadel's Textbook of Respiratory Medicine, Chapter 2 - Stages of Lung Development with Cellular and Molecular Mechanisms
This is a shared conversation. Sign in to Orris to start your own chat.