pediatric neuroogical examination in detail
pediatric neurological examination cranial nerves motor sensory reflexes
neurological assessment infants children developmental milestones primitive reflexes
pediatric neurological examination reflexes developmental assessment
Pediatric Neurological Examination
1. General Approach & Preparation
- Observe first: Watch the child enter the room, interact with caregivers, and play spontaneously.
- Age-appropriate engagement: Use toys, pictures, or games. In infants, examine on the parent's lap.
- Order flexibility: Perform the least distressing components first (e.g., observe, then elicit reflexes, save invasive/unpleasant parts for last).
- Developmental context: All findings must be interpreted against age-appropriate norms.
2. History (Pre-Examination)
- Birth history: Gestational age, perinatal complications, APGAR scores, neonatal ICU stay
- Developmental milestones: Gross motor, fine motor, speech/language, social
- Regression: Loss of previously acquired skills (red flag)
- Family history: Neurodegenerative diseases, epilepsy, neuromuscular disorders
- Seizures: Type, frequency, duration, post-ictal phase
- Behavioral/cognitive concerns
3. Mental Status
| Domain | Assessment Method |
|---|---|
| Level of consciousness | Alert, drowsy, stuporous, comatose |
| Orientation | Age-appropriate: name, age, place, date |
| Attention | Digit span, sustained play, counting backwards |
| Language | Vocabulary, fluency, comprehension, naming, repetition |
| Memory | 3-object recall (older children) |
| Behavior/affect | Observed during interaction |
| Cognitive level | Drawings (person, shapes), reading, reasoning |
In infants: assess alertness, social smile, visual fixation/tracking, and response to voice.
4. Cranial Nerve Examination
CN I – Olfactory
- Rarely tested routinely; use familiar scents (coffee, vanilla) in older children if anosmia is suspected.
CN II – Optic
- Visual acuity: Snellen chart (age ≥ 3), preferential looking or Cardiff cards (infants)
- Visual fields: Confrontation testing; in infants, watch for blink to threat from periphery
- Pupillary light reflex (afferent limb)
- Fundoscopy: Optic disc (papilledema, pallor), cup-to-disc ratio
CN III, IV, VI – Oculomotor, Trochlear, Abducens
- Extraocular movements: Pursuit (follow a target), saccades
- Ptosis, diplopia, nystagmus
- Pupil: Direct and consensual light reflex; accommodation
- In infants: use a moving light or bright toy
CN V – Trigeminal
- Sensory: Light touch to forehead, cheeks, chin (all 3 divisions)
- Motor: Jaw clench, lateral jaw movement (masseter, temporalis, pterygoids)
- Corneal reflex: Touch with cotton wisp → blink (CN V afferent, CN VII efferent)
CN VII – Facial
- Motor: Observe symmetry when smiling, crying, grimacing
- Upper vs. lower face: Upper motor neuron lesion spares the forehead (bilateral cortical input)
- Taste on anterior 2/3 tongue (rarely tested in routine exam)
CN VIII – Vestibulocochlear
- Hearing: Startle to sound (neonates), whisper test, tuning fork (Rinne/Weber) in older children
- Vestibular: Nystagmus, Dix-Hallpike maneuver (older children)
CN IX, X – Glossopharyngeal, Vagus
- Palatal elevation: Say "Ahh" — uvula should rise midline
- Gag reflex: Bilateral
- Voice quality: Hoarseness, nasal quality
- Swallowing
CN XI – Accessory
- Sternocleidomastoid: Head turn against resistance
- Trapezius: Shoulder shrug against resistance
CN XII – Hypoglossal
- Tongue: Protrusion (deviates toward lesion side), atrophy, fasciculations
5. Motor System
Inspection
- Muscle bulk: Wasting, pseudohypertrophy (calf — Duchenne MD)
- Fasciculations: Fine involuntary twitches (lower motor neuron)
- Abnormal movements: Tremor, chorea, athetosis, dystonia, myoclonus, tics
Tone
| Finding | Interpretation |
|---|---|
| Hypotonia ("floppy infant") | LMN lesion, metabolic, cerebellar, benign congenital |
| Hypertonia/spasticity | UMN lesion (velocity-dependent) |
| Rigidity (lead-pipe/cogwheel) | Extrapyramidal |
| Hypotonia with brisk reflexes | UMN lesion at cervical/thoracic level |
- Infants: Ventral suspension (Landau), pull-to-sit, traction response, passive limb movement
- Children: Passive range of motion at wrist, elbow, ankle; pendulum test
Power (MRC Scale, modified for children)
| Grade | Description |
|---|---|
| 0 | No contraction |
| 1 | Flicker only |
| 2 | Movement with gravity eliminated |
| 3 | Movement against gravity, not resistance |
| 4 | Movement against partial resistance |
| 5 | Normal power |
- In young children, assess by observing play: reach, grasp, crawl, stand, climb stairs.
Key Muscle Groups to Test
- Upper limbs: Shoulder abduction (C5), elbow flexion (C5–C6), wrist extension (C6–C7), finger extension (C7), grip (C8), intrinsics (T1)
- Lower limbs: Hip flexion (L1–L2), knee extension (L3–L4), dorsiflexion (L4–L5), plantar flexion (S1–S2)
6. Deep Tendon Reflexes (DTRs)
| Reflex | Nerve Root | Method |
|---|---|---|
| Biceps | C5–C6 | Tap biceps tendon |
| Triceps | C6–C7 | Tap triceps tendon |
| Brachioradialis | C5–C6 | Tap radius above wrist |
| Knee (patellar) | L3–L4 | Tap patellar tendon |
| Ankle (Achilles) | S1–S2 | Tap Achilles tendon |
- 0 = Absent; 1+ = Diminished; 2+ = Normal; 3+ = Brisk; 4+ = Clonus present
Plantar Response (Babinski Sign)
- Stroke lateral sole heel to toe → normal: plantar flexion of toes
- Positive Babinski: Extension of big toe + fanning of others (extensor plantar response)
- Normal up to 18–24 months of age due to immature corticospinal tract
Abdominal Reflexes
- Stroke abdomen in each quadrant → contraction toward stimulus
- Absence suggests UMN lesion (T7–T12)
Cremasteric Reflex (males)
- Stroke inner thigh → ipsilateral cremasteric contraction (L1–L2)
7. Primitive / Neonatal Reflexes
| Reflex | Elicitation | Normal Disappearance |
|---|---|---|
| Moro (startle) | Sudden head drop → symmetric arm abduction + extension, then flexion | 4–6 months |
| Rooting | Stroke corner of mouth → head turns toward stimulus | 3–4 months (awake) |
| Sucking | Touch center of lips | 3–4 months (awake) |
| Palmar grasp | Press palm between thumb and index finger → forced grasp | 5–6 months |
| Plantar grasp | Press plantar surface of toes → toe flexion | 9–12 months |
| Asymmetric tonic neck reflex (ATNR) | Turn head to one side → ipsilateral arm extends, contralateral flexes ("fencing posture") | 4–6 months |
| Symmetric tonic neck reflex (STNR) | Neck flexion → arm flexion, leg extension; neck extension → arm extension, leg flexion | 8–12 months |
| Tonic labyrinthine reflex (TLR) | Prone → increased flexor tone; supine → increased extensor tone | 6 months |
| Galant reflex | Stroke paravertebral back → lateral trunk flexion toward stimulus | 3–6 months |
| Stepping/walking reflex | Hold upright, sole touches surface → reciprocal stepping | 2 months |
| Placing reflex | Dorsum of foot touches table edge → leg lifts and places | 2 months |
| Landau reflex | Ventral suspension → spine/head extends; head flexed → hips flex | Integrates ~24 months |
| Parachute reflex | Lower head-first toward surface → arms extend protectively | Appears 6–9 months, persists lifelong |
Moro reflex assessment (illustrated below): The child is tilted backward, triggering arm abduction/extension followed by flexion. Persistence beyond 6 months or asymmetry warrants further evaluation.

8. Sensory Examination
| Modality | Test | Pathway |
|---|---|---|
| Light touch | Cotton wool | Dorsal column + spinothalamic |
| Pain | Pinprick (use disposable pin) | Spinothalamic (lateral) |
| Temperature | Cold tuning fork | Spinothalamic |
| Vibration | 128 Hz tuning fork on bony prominences | Dorsal column (posterior) |
| Proprioception (JPS) | Move digit up/down; patient reports direction | Dorsal column |
| Cortical sensation | 2-point discrimination, graphesthesia, stereognosis | Parietal cortex |
- In infants/toddlers: observe withdrawal from noxious stimuli; assess symmetry.
- Dermatomal distribution guides localization of lesions.
9. Cerebellar Examination
| Test | Technique | Finding in Cerebellar Disease |
|---|---|---|
| Finger-nose-finger | Touch examiner's finger, then own nose, repeatedly | Dysmetria, intention tremor |
| Heel-shin test | Run heel down contralateral shin | Dysmetria |
| Rapid alternating movements | Pronate/supinate hand rapidly | Dysdiadochokinesia |
| Rebound test | Flex arm against resistance, suddenly release | Overshoot |
| Romberg test | Stand feet together, eyes closed (age ≥ 5) | Positive = proprioceptive/vestibular (NOT cerebellar) |
| Tandem gait | Walk heel-to-toe | Ataxia, wide base |
- Cerebellar signs: DANISH — Dysdiadochokinesia, Ataxia, Nystagmus, Intention tremor, Slurred speech (dysarthria), Hypotonia
10. Gait Assessment
| Gait Type | Features | Causes |
|---|---|---|
| Hemiplegic | Circumduction, arm not swinging, foot drop | UMN lesion (stroke, CP) |
| Diplegic (scissor) | Legs crossed, toe-walking, hip adductor spasticity | Bilateral CP |
| Ataxic (cerebellar) | Wide-based, staggering, irregular cadence | Cerebellar lesion |
| Sensory ataxic | Stamp feet, worse with eyes closed | Dorsal column dysfunction |
| Steppage | High-stepping, foot slap, foot drop | LMN/peripheral nerve (peroneal) |
| Waddling (Trendelenburg) | Pelvis drops to swing side, trunk sway | Proximal myopathy, DMD |
| Toe-walking | Persistent bilateral | Spasticity, autism, idiopathic |
- Also assess: running, jumping, hopping (single leg by age 4), climbing stairs (alternate feet by age 3).
11. Higher Cortical Functions (Older Children)
| Function | Test |
|---|---|
| Dominant hemisphere | Language (aphasia assessment), calculation, reading, writing |
| Non-dominant hemisphere | Spatial tasks, copying figures, neglect |
| Frontal lobe | Abstract reasoning, Go-No-Go tasks, sequencing, primitive reflexes (grasp, suck, palmomental) |
| Parietal lobe | Graphesthesia, stereognosis, 2-point discrimination, body image |
12. Age-Specific Examination Considerations
| Age Group | Focus Areas |
|---|---|
| Neonate (0–1 mo) | Level of alertness, fontanelle, suck/rooting, Moro, tone, cry quality |
| Infant (1–12 mo) | Primitive reflex integration, emergence of postural reflexes, gross motor milestones |
| Toddler (1–3 yrs) | Gait, speech, fine motor (stacking blocks), behavior |
| Preschool (3–5 yrs) | Finger-nose, heel-shin, tandem gait, drawing skills |
| School-age (>5 yrs) | Full adult-equivalent examination possible; add cognitive/academic assessment |
13. Key Localizing Features
| Localization | Key Findings |
|---|---|
| Cortex/UMN | Spasticity, hyperreflexia, extensor plantar, no atrophy |
| Basal ganglia | Choreoathetosis, dystonia, rigidity, resting tremor |
| Cerebellum | Hypotonia, ataxia, dysmetria, nystagmus, no sensory loss |
| Brainstem | Crossed signs: cranial nerve deficit ipsilateral, long tract signs contralateral |
| Spinal cord | Sensory level, bilateral motor/reflex changes below level |
| Anterior horn/LMN | Flaccidity, hyporeflexia, atrophy, fasciculations |
| Peripheral nerve | Distal sensorimotor loss, hyporeflexia, glove-stocking distribution |
| Neuromuscular junction | Fatigable weakness, no sensory deficit (e.g., myasthenia) |
| Muscle | Proximal weakness, waddling gait, pseudohypertrophy, normal reflexes early |
Summary Checklist
- Mental status / developmental level
- Cranial nerves I–XII
- Motor: tone, bulk, power, abnormal movements
- Deep tendon reflexes + plantar response
- Primitive reflexes (age-appropriate integration)
- Sensory: touch, pain, vibration, proprioception
- Cerebellar: coordination, Romberg
- Gait and station
- Higher cortical functions (in older children)
in physiotherapy expsin pediatric neuroogical examination in detail
pediatric neurological physiotherapy assessment tone reflexes movement
physiotherapy functional assessment children cerebral palsy developmental delay motor function
pediatric physiotherapy neurological assessment postural reflexes tone gait
Pediatric Neurological Examination in Physiotherapy
Core PT Philosophy
"Observe before you touch. Play before you test."
- Use the child's spontaneous play and caregiver interaction as the richest source of information.
- Examination is dynamic — assess what the child can do, not just what they cannot.
- Findings must be linked to functional goals (sitting, walking, self-care, play).
- Always interpret findings against age-appropriate developmental norms.
Structure of the PT Neurological Examination
1. History & Interview
2. Observation (Posture, Spontaneous Movement)
3. Muscle Tone Assessment
4. Primitive & Postural Reflex Assessment
5. Muscle Power & Selective Motor Control
6. Range of Motion & Musculoskeletal Assessment
7. Sensory Assessment
8. Coordination & Balance
9. Functional Mobility & Gait Analysis
10. Standardized Assessment Tools
11. Participation & Activity Limitations
1. History & Interview (Parent/Caregiver)
| Area | Key Questions |
|---|---|
| Birth history | Prematurity, birth asphyxia, NICU stay, hypoxic-ischaemic encephalopathy |
| Motor milestones | Age of head control, rolling, sitting, standing, walking; any regression |
| Feeding/swallowing | Difficulty sucking, chewing, drooling |
| Communication | First words, babbling, current communication method |
| Functional concerns | What can't the child do that peers can? What worries the family most? |
| Medical history | Seizures, surgeries (SDR, orthopaedic), medications (baclofen, botulinum toxin) |
| Prior therapy | What therapies, frequency, perceived effect |
| Equipment | Orthotics, wheelchairs, walkers, splints |
| Home/school environment | Barriers to participation, school inclusion |
2. Observation
Resting Posture
| Posture | What to Note |
|---|---|
| Supine | Head position (ATNR dominant?), hip posture, fisting of hands, opisthotonus |
| Prone | Head lifting, weight-bearing through arms, pelvic position |
| Sitting | Trunk support required? Kyphosis, scoliosis, W-sitting, prop sitting |
| Standing | Alignment, base of support, toe-standing, knee hyperextension |
Spontaneous Movement
- Quality: Fluent vs. fragmented, symmetric vs. asymmetric
- General Movements Assessment (GMA / Prechtl): In infants <5 months — assess for Fidgety Movements (FMs)
- Absent FMs at 9–20 weeks corrected age = strong predictor of cerebral palsy
- Quantity: Is the child moving all limbs spontaneously?
- Facial expression: Grimacing during movement (pain? effort?)
Body Composition
- Muscle wasting (limb asymmetry, hemiatrophy)
- Pseudohypertrophy of calves (Duchenne MD)
- Joint deformities: equinus, hip dislocation, scoliosis
3. Muscle Tone Assessment
Types of Abnormal Tone
| Tone Type | Feel | Associated Condition |
|---|---|---|
| Spasticity | Velocity-dependent resistance; clasp-knife release | Cerebral palsy (UMN) |
| Rigidity | Constant resistance throughout range; lead-pipe or cogwheel | Basal ganglia disorders |
| Hypotonia (flaccidity) | Floppy, reduced resistance, excessive range | Down syndrome, SMA, cerebellar, LMN lesions |
| Dystonia | Fluctuating tone with sustained abnormal postures triggered by movement/effort | Dyskinetic CP, metabolic disorders |
| Mixed tone | Spastic + dystonic elements | Common in CP |
Techniques for Tone Assessment
A. Passive Movement
- Slowly then quickly move each joint through full range.
- Spasticity: Resistance increases with speed — use Modified Ashworth Scale (MAS).
| Score | Description |
|---|---|
| 0 | No increase in tone |
| 1 | Slight increase — catch and release at end of ROM |
| 1+ | Catch followed by minimal resistance throughout |
| 2 | Marked increase — passive movement difficult |
| 3 | Considerable increase — passive movement very difficult |
| 4 | Affected part rigid in flexion or extension |
B. Infant-Specific Tone Tests
| Test | Technique | Normal Finding | Abnormal |
|---|---|---|---|
| Pull-to-sit (traction) | Pull infant from supine to sitting by wrists | Head lags initially but righting by 4–5 months | Excessive head lag = hypotonia |
| Ventral suspension | Support infant prone in mid-air at examiner's hand | Head, hips, limbs extend by 3 months (Landau) | Hypotonia: U-shaped posture |
| Scarf sign | Pull arm across chest; note elbow position relative to midline | Elbow does not pass midline | Elbow easily past midline = hypotonia |
| Heel-to-ear | Flex hip, bring heel toward ipsilateral ear | Resistance felt before heel reaches ear | No resistance = hypotonia |
| Popliteal angle | Hip at 90°, extend knee; measure angle | Varies with age; decreases with gestational age | Tight hamstrings or spasticity |
| Adductor angle | Spread legs; measure angle between thighs | Widens with age | Reduced = adductor spasticity |
C. Tardieu Scale (PT Gold Standard for Spasticity)
- R1: Angle where catch is felt at fast speed (V3) — reflects spasticity
- R2: Full passive ROM at slow speed (V1) — reflects muscle length/contracture
- Spasticity angle = R2 − R1 (if >10°, significant dynamic component = responds to BTX)
4. Primitive and Postural Reflexes
A. Primitive Reflexes (Subcortical; should integrate with CNS maturation)
| Reflex | How to Elicit | Normal Response | Integration Age | PT Significance |
|---|---|---|---|---|
| Moro | Sudden head drop or startle | Arms abduct/extend → adduct/flex | 4–6 months | Persistence → limits protective extension, triggers startle in movement |
| Rooting | Stroke corner of mouth | Head turns toward stimulus | 3–4 months | Persistence → affects feeding, facial control |
| Sucking | Touch lips with fingertip | Sucking movement | 3–4 months (awake) | Persistence → oral motor problems |
| Palmar grasp | Press finger into palm | Finger flexion grip | 5–6 months | Persistence → limits voluntary hand release for function |
| Plantar grasp | Press under toes | Toe flexion | 9–12 months | Persistence → toe-curling in standing, limits balance |
| ATNR (asymmetric tonic neck) | Turn head to one side | Ipsilateral arm extends, contralateral flexes ("fencing") | 4–6 months | Persistence → limits midline hand use, rolling, bilateral activities |
| STNR (symmetric tonic neck) | Flex neck | Arms flex, legs extend | 8–12 months | Persistence → limits reciprocal crawling, W-sitting |
| TLR (tonic labyrinthine) | Prone: flexor tone↑; Supine: extensor tone↑ | Diminishes with postural control | 6 months | Persistence → limits antigravity posture, causes extensor thrust |
| Galant | Stroke paravertebral area | Trunk curves toward stimulus | 3–6 months | Persistence → affects sitting balance (hip sway), toilet training |
| Stepping | Hold upright, feet touch surface → reciprocal steps | Present at birth | 2 months | Used in treadmill training for locomotion facilitation |
TLR assessment (shown below): The child's head is flexed forward. Persistence causes involuntary knee deflection, fist-clenching, and postural instability — observed and graded by the physiotherapist.
B. Postural Reactions (Develop WITH CNS maturation; should APPEAR at expected ages)
| Reaction | Appearance Age | How to Test | Normal Response | PT Significance |
|---|---|---|---|---|
| Head righting (optical/labyrinthine) | 1–3 months | Tilt child sideways, prone, supine | Head rights to vertical | Absent = cannot achieve upright posture |
| Body-on-head righting | 4–6 months | Tilt in space — head rights body follows | Segmental alignment | Poor trunk control in sitting |
| Landau | 3–6 months | Ventral suspension → spine and head extend | Extends entire axial body | Absence = poor extensor tone |
| Protective extension (Parachute — forward) | 6–7 months | Tip child forward → arms extend | Arms extend to protect | Absent → falls forward without protection |
| Protective extension (lateral) | 6–8 months | Push sideways in sitting | Ipsilateral arm extends | Absent → lateral falls |
| Protective extension (backward) | 9–12 months | Push backward in sitting | Arms extend backward | Absent → posterior falls |
| Equilibrium reactions — prone | 5 months | Tilt prone on tilt board | Trunk curves toward raised side, limbs abduct | Absent = poor balance |
| Equilibrium reactions — supine | 7 months | Tilt supine | Righting response | Absent = balance disorder |
| Equilibrium reactions — sitting | 7–8 months | Displace in sitting | Trunk righting + limb reaction | Assesses functional sitting balance |
| Equilibrium reactions — standing | 12–18 months | Displace in standing | Step or trunk righting | Absent = cannot maintain independent stance |
Key PT principle: Therapy aims to inhibit persistent primitive reflexes and facilitate emergence/maturation of postural reactions.
5. Muscle Power & Selective Motor Control
Manual Muscle Testing (MMT) — Modified for Children
| Age | Method |
|---|---|
| Infant | Observe spontaneous antigravity movements |
| Toddler | Functional strength: standing from floor, climbing, throwing |
| >5 years | Formal MMT using MRC grading (0–5) |
Selective Motor Control (SMC)
- Ask child to: dorsiflex foot without moving knee or hip
- Graded: Normal → Impaired → Unable (important in CP for surgical planning)
- Selective Control Assessment of Lower Extremity (SCALE): Formal tool for CP
Key Functional Strength Observations
| Task | Muscle Group Inferred |
|---|---|
| Rising from floor without push (Gowers' sign negative) | Hip extensors/abductors |
| Gowers' sign positive: pushes up legs with hands | Proximal weakness (Duchenne MD, SMA) |
| Heel-toe walking | Gastrocnemius-soleus vs. tibialis anterior |
| Single-leg stance | Hip abductors (gluteus medius) |
| Stair climbing | Quadriceps, hip extensors |
6. Range of Motion & Musculoskeletal Assessment
| Joint | Common Contracture | Tool |
|---|---|---|
| Ankle | Equinus (plantarflexion) | Goniometry; Silfverskiöld test (distinguish gastrocnemius vs. soleus) |
| Knee | Flexion contracture, crouch | Popliteal angle (hamstrings), Thomas test (hip flexors) |
| Hip | Flexion, adduction, internal rotation | Modified Thomas, Ober's, Craig's (femoral anteversion) |
| Spine | Scoliosis, kyphosis | Adam's forward bend test, Cobb angle |
| Shoulder | Internal rotation, adduction | Passive ROM |
| Hand/wrist | Flexion deformity | Passive ROM, thumb-in-palm |
7. Sensory Assessment
| Modality | Age ≤ 5 years | Age > 5 years |
|---|---|---|
| Light touch | Watch for withdrawal or awareness | Monofilament or cotton wool |
| Pain | Observe response to pin | Pinprick test |
| Proprioception | Observe balance; spontaneous weight shifting | Joint position sense (move toe up/down) |
| Vibration | Observe awareness | 128 Hz tuning fork |
| Tactile discrimination | Observe preferences, tactile defensiveness | Stereognosis |
PT-Specific Sensory Concerns:
- Tactile defensiveness: Child avoids touch, textures — affects therapy participation
- Proprioceptive deficits: Poor joint awareness → unstable gait, falls, clumsiness
- Two-point discrimination: Relevant in hand function assessment
- Pain/temperature: Important in spina bifida (sensory level)
- Sensory level mapping: Dermatome testing in spinal cord conditions (spina bifida, SCI)
8. Coordination & Balance
Coordination Tests
| Test | Age | Assesses |
|---|---|---|
| Finger-nose-finger | ≥ 4 yrs | Upper limb coordination, dysmetria |
| Heel-shin test | ≥ 5 yrs | Lower limb coordination |
| Diadochokinesia (rapid alternating movements) | ≥ 5 yrs | Cerebellar function |
| Building block towers | 18 mo+ | Bilateral coordination, fine motor |
| Catching a ball | 3–4 yrs | Visuomotor coordination |
| Bead threading | 3–4 yrs | Fine motor coordination |
Balance Assessment
| Test | Age | Description |
|---|---|---|
| Romberg test | ≥ 5 yrs | Stand feet together, eyes open then closed; positive = sway/fall with eyes closed |
| Single-leg stance | ≥ 3 yrs | Normal: 3–5 sec at age 3; 10 sec at age 5 |
| Tandem stance/gait | ≥ 4 yrs | Heel-to-toe walking; cerebellar or vestibular ataxia |
| Perturbation test | All ages | Gentle push in standing — observe stepping reaction |
| Functional reach test | ≥ 5 yrs | Reach forward maximally without stepping |
| Timed Up and Go (TUG) | ≥ 3 yrs | Stand, walk 3m, return, sit — time and quality |
Pediatric Balance Scale (PBS)
- Modified Berg Balance Scale for children with motor impairments
- 14 items, scored 0–4 each; max 56
9. Functional Mobility & Gait Analysis
Observational Gait Analysis (OGA)
| Plane | What to Observe |
|---|---|
| Sagittal | Foot contact (heel/toe/flat), knee flexion in swing, trunk lean |
| Frontal | Lateral trunk sway, Trendelenburg, scissoring, step width |
| Transverse | Foot progression angle (in-toeing, out-toeing), arm swing |
Common Pediatric Gait Patterns (PT Classification)
| Gait Pattern | Characteristics | Common Cause |
|---|---|---|
| Hemiplegic | Circumduction, arm held in flexion, foot drop or equinus | Hemiplegia CP, stroke |
| Diplegic / Scissor | Knees/hips adducted, crossing steps, toe-walking | Spastic diplegia CP |
| Crouch gait | Excessive knee and hip flexion throughout stance | Weak plantarflexors, hamstring spasticity |
| Jump gait | Equinus + knee flexion + hip flexion | Spasticity at multiple levels |
| Ataxic | Wide base, irregular cadence, trunk sway | Cerebellar/vestibular |
| Trendelenburg (waddling) | Pelvis drops on swing side, trunk sway | Weak hip abductors (DMD, DDH) |
| Steppage | High hip/knee lift to clear foot drop | Peripheral nerve palsy (peroneal) |
| Antalgic | Shortened stance on painful limb | Pain |
| Toe-walking (bilateral) | Persistent, no heel strike | Spasticity, idiopathic, autism |
Functional Mobility Assessment
| Task | Typical Age of Acquisition |
|---|---|
| Rolls supine → prone | 4–5 months |
| Sits independently | 6–7 months |
| Pulls to stand | 9–10 months |
| Cruises along furniture | 9–12 months |
| Independent walking | 12–15 months |
| Running | 18 months |
| Stairs (two feet per step) | 24 months |
| Jumps with two feet | 24–30 months |
| Stairs (alternating feet) | 3 years |
| Hops on one foot | 4 years |
| Skips | 5–6 years |
10. Standardized PT Assessment Tools
Infant / Early Childhood
| Tool | Age | Measures | Notes |
|---|---|---|---|
| Prechtl's General Movement Assessment (GMA) | 0–5 months corrected | Quality of spontaneous movements | Best early CP predictor |
| Hammersmith Infant Neurological Exam (HINE) | 2–24 months | Cranial nerves, posture, movements, tone, reflexes | Validated CP predictor (Care for CP, p.1) |
| Alberta Infant Motor Scale (AIMS) | 0–18 months | Gross motor development (prone, supine, sit, stand) | Observe only, no handling |
| Test of Infant Motor Performance (TIMP) | 34 wks–4 months corrected | Motor control in infancy | NICU/early intervention |
| Bayley Scales (BSID-IV) | 1–42 months | Cognitive, language, motor | Comprehensive developmental |
Preschool / School Age
| Tool | Age | Measures |
|---|---|---|
| Gross Motor Function Measure (GMFM-66 / 88) | All ages with CP | 5 dimensions: lying, rolling, sitting, standing, walking/running/jumping |
| Gross Motor Function Classification System (GMFCS) | CP, all ages | Functional level I–V (I = walks without limits; V = dependent mobility) |
| Pediatric Balance Scale (PBS) | 5–15 yrs | Balance in 14 functional tasks |
| Timed Up and Go (TUG) | ≥ 3 yrs | Functional mobility speed |
| 6-Minute Walk Test (6MWT) | ≥ 5 yrs | Endurance, functional capacity |
| Movement ABC-2 (MABC-2) | 3–16 yrs | Manual dexterity, ball skills, balance |
| Bruininks-Oseretsky Test (BOT-2) | 4–21 yrs | Comprehensive motor proficiency |
| Pediatric Evaluation of Disability Inventory (PEDI-CAT) | 0–21 yrs | Self-care, mobility, social, responsibility |
| WeeFIM | 6 months–7 yrs | Functional independence in daily tasks |
| GMFM-66 Basal & Ceiling | CP | Most sensitive version for outcome tracking |
CP-Specific Classification Systems
| System | What It Classifies |
|---|---|
| GMFCS (Gross Motor Function Classification) | Gross motor function I–V |
| MACS (Manual Ability Classification) | Hand use I–V |
| CFCS (Communication Function Classification) | Communication I–V |
| EDACS (Eating & Drinking Ability Classification) | Feeding safety I–V |
| VFCS (Visual Function Classification) | Vision I–V |
11. Activity, Participation & Environment (ICF Framework)
Body Structure/Function → Activity → Participation
↑ ↑
(tone, power, (school, play,
reflexes) community)
↑_____________Context_________________↑
(family, equipment,
home, school)
| ICF Level | PT Assessment Focus |
|---|---|
| Body structure/function | Tone, power, ROM, reflexes, sensation, coordination |
| Activity | GMFM, TUG, PEDI-CAT, walking, transfers, self-care |
| Participation | School inclusion, sports, play, community access |
| Environmental factors | Home layout, assistive devices, caregiver support |
| Personal factors | Motivation, pain, fatigue, behavior, cognition |
12. Documentation & Clinical Reasoning
- Impairments (e.g., spastic diplegia, bilateral plantarflexor contracture, reduced balance)
- Activity limitations (e.g., GMFCS Level II — walks with limitation, no running)
- Participation restrictions (e.g., excluded from school PE, cannot access playground)
- Prognostic indicators (e.g., HINE score, GMA fidgety movement presence, MRI findings)
- SMART Goals — jointly set with child and family
- Treatment plan: NDT/Bobath, strength training, constraint-induced movement therapy (CIMT), treadmill training, orthotics, hydrotherapy, etc.
Summary Checklist for Pediatric PT Neurological Examination
- Detailed developmental and medical history
- Structured observation (resting posture, spontaneous movement quality)
- Muscle tone (MAS, Tardieu scale, infant tone tests)
- Primitive reflex integration (ATNR, TLR, Moro, palmar/plantar grasp, Galant, STNR)
- Postural reactions (head righting, protective extension, equilibrium reactions)
- Selective motor control and muscle power (functional + MMT)
- Musculoskeletal assessment (ROM, contracture, bony deformity)
- Sensory assessment (tactile, proprioception, pain)
- Coordination (dysmetria, diadochokinesia, fine motor)
- Balance (Romberg, PBS, single-leg stance, perturbation)
- Gait analysis (OGA, instrumented if available)
- Functional mobility milestones (GMFM, TUG, 6MWT)
- Standardized tools (HINE, GMA, AIMS, GMFCS, MABC-2 as appropriate)
- ICF-based summary with goals and plan
deveomemtka miestone swith examination in deati
developmental milestones gross motor fine motor language social infant child examination
developmental assessment red flags delay screening tools pediatric
developmental milestones chart infant child gross motor fine motor language
Developmental Milestones with Examination in Detail
Framework: The Five Domains
| Domain | What It Reflects | Key Pathways |
|---|---|---|
| Gross Motor | Posture, balance, locomotion | Corticospinal, cerebellar, musculoskeletal |
| Fine Motor / Visuomotor | Hand-eye coordination, manipulation | Corticospinal, parietal, cerebellar |
| Language / Communication | Receptive & expressive speech | Broca's, Wernicke's, auditory pathways |
| Personal-Social | Self-care, interaction, emotional regulation | Frontal, limbic, social cognition |
| Cognitive / Adaptive | Problem-solving, learning, daily living | Widespread cortical networks |
How to Examine Developmental Milestones
General Principles
- Begin with observation during free play and caregiver interaction — this reveals more than formal testing in young children.
- Use age-appropriate toys/stimuli: rattle (0–3 mo), colorful object (3–6 mo), cup/block (6–12 mo), picture book (12–24 mo), pencil/paper (>2 yrs).
- Correct for prematurity up to 24 months of age (use corrected age = chronological age − weeks premature).
- Involve caregivers — their report is validated and essential.
- Always check vision and hearing before attributing delay to another cause.
Age-by-Age Milestone Examination
🔹 Newborn (0–1 Month)
Gross Motor
| Milestone | How to Examine |
|---|---|
| Flexed posture (predominant) | Observe at rest — limbs flexed, fists clenched |
| Head control: turns side-to-side in prone | Place prone, observe head rotation |
| Brief head raising in prone | Place prone on flat surface, observe |
| Pull-to-sit: complete head lag | Hold wrists, pull to sit — head completely lags |
Fine Motor
| Milestone | Examination |
|---|---|
| Hands fisted | Observe resting hand posture |
| Grasp reflex present | Press finger into palm → fingers grip |
Language
| Milestone | Examination |
|---|---|
| Startle to loud sound | Clap or make loud noise — observe startle (Moro or blink) |
| Quiets to familiar voice | Speak softly near ear — observe calming |
| Cries to express need | Note quality: high-pitched cry = abnormal |
Social
| Milestone | Examination |
|---|---|
| Regards face | Hold face 20–30 cm away, move slowly — observe visual fixation |
| Responds to comforting | Hold and rock — observe calming |
🔹 2 Months
Gross Motor
| Milestone | Examination |
|---|---|
| Lifts head to 45° in prone | Place prone — observe head elevation |
| Less head lag on pull-to-sit | Pull to sit — some lag remains but reducing |
| Kicks symmetrically | Observe supine spontaneous kicking |
Fine Motor
| Milestone | Examination |
|---|---|
| Hands unfisted 50% of time | Observe resting posture |
| Follows object 180° | Hold red ball 30 cm from face, move side to side |
Language
| Milestone | Examination |
|---|---|
| Cooing (vowel sounds: "ooh", "aah") | Talk to baby, pause — listen for vocalization |
| Alerts to voice | Speak from behind — observe head/eye turn |
Social
| Milestone | Examination |
|---|---|
| Social smile ✦ | Smile and talk to baby — smiles back (KEY milestone) |
| Recognizes caregiver | Observe differential response to parent vs. stranger |
Red Flag at 2 months: No social smile, does not fix and follow, no response to sound.
🔹 4 Months
Gross Motor
| Milestone | Examination |
|---|---|
| Head steady in supported sitting | Hold in sitting position — note head stability |
| Lifts head and chest 90° in prone, weight on forearms | Place prone — observe full chest elevation |
| No head lag on pull-to-sit | Pull by wrists — head should come with body |
| Rolls prone to supine | Place prone — may roll spontaneously |
Fine Motor
| Milestone | Examination |
|---|---|
| Hands come to midline | Place supine — observe hands meeting at chest |
| Reaches for dangling object | Dangle bright object in midline — observe reach |
| Brings objects to mouth | Give a rattle — observe mouthing |
| Palmar grasp: ulnar > radial | Note which side of palm is used |
Language
| Milestone | Examination |
|---|---|
| Laughs aloud | Play peek-a-boo or tickle |
| Turns to voice | Call from the side — observe head turning |
| Babbles (consonant-vowel: "ba", "ga") | Elicit by talking; observe reciprocal vocalization |
Social
| Milestone | Examination |
|---|---|
| Recognizes familiar people | Note differential response to known vs. unknown |
| Enjoys social interaction | Observe excitement (arm/leg movement) when approached |
Red Flag at 4 months: No social smile, does not follow objects, does not bring hands to midline, no vocalization.
🔹 6 Months
Gross Motor
| Milestone | Examination |
|---|---|
| Sits with propping (tripod) | Place in sitting — props on extended arms |
| Rolls both directions | Observe or place supine and observe rolling |
| Weight bears on legs when held upright | Hold upright — legs should take weight (bouncing) |
| Pivots in prone | Observe self-propulsion in prone |
Fine Motor
| Milestone | Examination |
|---|---|
| Transfers object hand to hand | Give block in one hand — observe transfer |
| Raking grasp (all fingers) | Scatter small pellets — observe grasp pattern |
| Reaches with one hand | Hold object to one side — observe unilateral reach |
| Manipulates objects, mouths | Give toy — observe manipulation |
Language
| Milestone | Examination |
|---|---|
| Babbles (repetitive syllables: "ba-ba", "da-da") | Engage verbally — listen for syllables |
| Vocalizes to get attention | Observe spontaneous vocalization |
| Responds to name | Call child's name — looks toward voice |
| Localizes sound horizontally | Make sound at ear level to side — observe head turning |
Social
| Milestone | Examination |
|---|---|
| Stranger anxiety begins | Observe reaction to unfamiliar examiner |
| Smiles at mirror image | Hold up small mirror — observe self-recognition smile |
Red Flag at 6 months: No sitting even with support, no reaching, no babbling, not turning to sounds.
🔹 9 Months
Gross Motor
| Milestone | Examination |
|---|---|
| Sits independently without support | Place sitting — observe balance |
| Gets to sitting from lying | Observe transition |
| Crawls (may commando crawl) | Place prone — observe locomotion |
| Pulls to stand | Place at furniture — observe pull-to-stand |
| Cruises (steps sideways along furniture) | Observe lateral stepping holding furniture |
Fine Motor
| Milestone | Examination |
|---|---|
| Pincer grasp (inferior) — thumb + forefinger | Scatter small pellet — observe pincer attempt |
| Bangs objects together | Give two blocks — observe banging |
| Uses index finger to poke | Place object in container — observe poking |
| Releases voluntarily | Offer hand for block — observe release |
Language
| Milestone | Examination |
|---|---|
| Says "mama/dada" non-specifically | Ask caregiver — record |
| Imitates sounds | Make sounds — observe imitation |
| Understands "no" | Say "no" — observe behavioral response |
| Waves bye-bye (if prompted) | Wave and say "bye-bye" |
Social
| Milestone | Examination |
|---|---|
| Strong stranger anxiety | Observe distress with unfamiliar examiner |
| Joint attention begins | Look at object, then back to examiner (proto-declarative pointing) |
| Plays peek-a-boo | Initiate game — observe anticipation and joy |
| Separation anxiety | Observe distress when caregiver leaves |
Red Flag at 9 months: No sitting, no babbling, no response to name, does not reach for objects.
🔹 12 Months (1 Year)
Gross Motor
| Milestone | Examination |
|---|---|
| Stands independently momentarily | Let go of support — observe independent stance |
| Walks with 2 hands held | Hold both hands and walk |
| Cruises well | Observe lateral stepping at furniture |
| May take first independent steps | Observe or ask caregiver |
Fine Motor
| Milestone | Examination |
|---|---|
| Neat pincer grasp ✦ | Scatter raisin/pellet — observe tip-to-tip pincer |
| Puts objects in container | Give block and container — observe placing |
| Bangs two blocks together | Give two blocks |
| Marks with crayon | Give crayon — observe scribbling |
Language
| Milestone | Examination |
|---|---|
| 1–3 true words (besides mama/dada) ✦ | Ask caregiver; elicit during exam |
| Understands simple commands ("give me") | Ask for object — observe compliance |
| Gestures: waves, points | Observe spontaneous pointing to request (proto-imperative) |
| Jargon (strings of syllables with intonation) | Listen for expressive language quality |
Social
| Milestone | Examination |
|---|---|
| Points to show interest (proto-declarative) ✦ | Observe spontaneous pointing at interesting objects |
| Imitates actions | Wave, clap — observe imitation |
| Drinks from cup | Give cup — observe drinking |
| Cooperative in dressing | Observe holding out arm/leg |
Red Flag at 12 months: No babbling, no gestures (pointing/waving), no words, does not respond to name. Absolute red flags: any language or social regression.
🔹 15 Months
Gross Motor
| Milestone | Examination |
|---|---|
| Walks independently ✦ | Observe gait (wide-based is normal) |
| Climbs stairs with help | Lead to steps — observe climbing |
| Throws ball | Give ball — observe throw |
| Stoops and recovers | Drop toy — observe bend and recovery |
Fine Motor
| Milestone | Examination |
|---|---|
| Stacks 2 blocks | Give blocks — observe tower |
| Scribbles spontaneously | Give crayon on paper |
| Uses spoon (with spillage) | Observe self-feeding |
Language
| Milestone | Examination |
|---|---|
| 4–6 words | Ask caregiver |
| Uses words with intent | Observe word usage in context |
| Points to body parts (1–2) | Ask: "Where is your nose/eyes?" |
Social
| Milestone | Examination |
|---|---|
| Indicates wants by pointing | Observe communication of needs |
| Plays near but not with other children (parallel play) | Observe |
| Drinks well from cup | Observe |
🔹 18 Months
Gross Motor
| Milestone | Examination |
|---|---|
| Walks well (narrow base) | Observe — should no longer be wide-based |
| Runs (stiffly) | Observe running in corridor |
| Walks upstairs holding rail | Test on steps |
| Throws ball overhand | Give ball — observe throw |
| Kicks ball | Place ball in front — instruct to kick |
Fine Motor
| Milestone | Examination |
|---|---|
| Stacks 3–4 blocks ✦ | Give blocks — observe tower height |
| Scribbles, imitates vertical stroke | Show vertical stroke — ask to copy |
| Turns pages of book (2–3 at a time) | Give board book — observe |
| Removes shoes/socks | Observe undressing |
Language
| Milestone | Examination |
|---|---|
| 10–20 words ✦ | Ask caregiver for word list |
| Points to pictures in book (3–5) | Show picture book: "Where is the dog?" |
| Identifies 3 body parts | Ask child to point to own nose, eyes, ears |
| Follows 2-step commands | "Pick up the ball and give it to me" |
Social
| Milestone | Examination |
|---|---|
| Symbolic/pretend play begins | Offer toy phone — observe pretend talking |
| Feeds self with spoon | Observe |
| Separation anxiety decreasing | Observe |
Red Flag at 18 months: No words, no pointing, no pretend play, not walking. Immediate concern: no consistent words by 16 months.
🔹 24 Months (2 Years)
Gross Motor
| Milestone | Examination |
|---|---|
| Runs well | Observe running — note coordination |
| Walks up AND down stairs (two feet per step) | Test on stairs |
| Jumps with both feet | Ask child to jump — both feet leave ground |
| Kicks ball well | Instruct to kick — observe |
| Throws overhand | Observe |
Fine Motor
| Milestone | Examination |
|---|---|
| Stacks 6–7 blocks ✦ | Give blocks — observe |
| Copies vertical and horizontal line | Draw line, ask child to copy |
| Draws circle (not copies yet) | Observe spontaneous scribbling |
| Turns pages one at a time | Give book — observe |
| Uses fork and spoon | Ask caregiver |
Language
| Milestone | Examination |
|---|---|
| 50+ words ✦ | Ask caregiver |
| 2-word combinations ✦ ("more milk", "daddy go") | Ask caregiver; elicit |
| Refers to self by name | Ask "Who are you?" or observe |
| 50% speech intelligible to strangers | Ask caregiver |
| Points to pictures on request (10+) | Show picture book |
Social
| Milestone | Examination |
|---|---|
| Parallel play | Observe play |
| Imitates adult activities | Observe domestic mimicry (sweeping, cooking) |
| Helps with undressing | Observe |
| Symbolic play | Uses block as car, doll as baby |
Red Flag at 2 years: No 2-word phrases, less than 50 words, speech not 50% intelligible, no pretend play.
🔹 3 Years
Gross Motor
| Milestone | Examination |
|---|---|
| Pedals tricycle | Ask caregiver |
| Climbs stairs alternating feet going up | Test on stairs |
| Stands on one foot for 3 seconds | Demonstrate, ask to copy |
| Jumps off bottom step | Observe |
| Broad jump (both feet) | Ask to jump forward |
Fine Motor
| Milestone | Examination |
|---|---|
| Copies circle ✦ | Draw circle, ask to copy |
| Stacks 9–10 blocks | Give blocks |
| Draws person with 3 parts | Ask "Draw a person" |
| Uses scissors | Give child-safe scissors — observe cutting |
| Buttons large buttons | Observe |
Language
| Milestone | Examination |
|---|---|
| 3-word sentences ✦ | Observe spontaneous speech |
| 75% intelligible to strangers | Assess during conversation |
| Knows name, age, gender | Ask "What is your name? How old are you?" |
| Understands prepositions (in, on, under) | "Put the block under the table" |
| Asks "why?" questions | Observe spontaneously |
| 900+ word vocabulary | Ask caregiver |
Social/Cognitive
| Milestone | Examination |
|---|---|
| Associative/parallel play | Observe play with peers |
| Names 4 colors | Show colored blocks — "What color is this?" |
| Counts to 3 | Ask to count objects |
| Copies cross (+) | Draw cross, ask to copy (some do at 3½) |
🔹 4 Years
Gross Motor
| Milestone | Examination |
|---|---|
| Hops on one foot ✦ | Demonstrate, ask to copy — should do 2–3 hops |
| Alternates feet going DOWN stairs | Test on stairs |
| Throws ball overhand with accuracy | Observe |
| Tandem walk (heel-toe) | Demonstrate — can do at least 4 steps |
| Skips (unilateral) | Observe |
Fine Motor
| Milestone | Examination |
|---|---|
| Copies cross (+) ✦ | Draw, ask to copy |
| Draws person with 6 parts | Ask "Draw a person" |
| Cuts along a line with scissors | Observe |
| Uses fork well | Ask caregiver |
Language
| Milestone | Examination |
|---|---|
| 100% intelligible ✦ | Assess during conversation |
| Tells stories | Ask "Tell me what you did today" |
| Understands opposites | "Big-small, hot-cold" |
| Counts to 10 | Ask to count |
| Answers "how" and "why" questions | Ask age-appropriate questions |
| 1,500+ word vocabulary | Assess complexity |
Social/Cognitive
| Milestone | Examination |
|---|---|
| Cooperative play ✦ | Observe play with peers — rules, roles |
| Understands "same" and "different" | Show two objects — ask comparison |
| Knows colors and shapes | Test with colored shapes |
| Recognizes letters (some) | Show alphabet |
🔹 5 Years
Gross Motor
| Milestone | Examination |
|---|---|
| Skips alternating feet | Observe skipping |
| Hops on one foot 8–10 times | Test each side |
| Catches small ball with hands | Throw small ball — observe |
| Rides bicycle (with training wheels) | Ask caregiver |
| Tandem gait: 8+ steps | Test |
Fine Motor
| Milestone | Examination |
|---|---|
| Copies triangle ✦ | Draw triangle, ask to copy |
| Draws person with 10 parts | Ask "Draw a person" |
| Writes own first name | Give pencil and paper |
| Cuts out shapes with scissors | Observe |
| Colors within lines | Observe |
Language
| Milestone | Examination |
|---|---|
| 5–8 word sentences | Observe conversation |
| Tells stories with beginning-middle-end | Ask for a narrative |
| Uses all grammatical structures | Observe for tense, plural, possessive |
| Counts to 20+ | Ask to count |
| Names 10+ colors | Test |
Social/Cognitive
| Milestone | Examination |
|---|---|
| Plays complex games with rules | Ask caregiver |
| Knows home address | Ask |
| Draws recognizable figures | Assess drawing |
| Beginning reading/writing | Assess letter recognition |
Consolidated Milestone Summary Table
| Age | Gross Motor | Fine Motor | Language | Social |
|---|---|---|---|---|
| 1 mo | Flexion posture, head to side in prone | Fisted hands, grasp reflex | Cry, startles to sound | Regards face |
| 2 mo | Head 45° prone, less lag | Follows 180°, hands to midline | Coos | Social smile |
| 4 mo | Head 90° prone, no lag | Reaches, palmar grasp, transfers | Laughs, babbles | Recognizes people |
| 6 mo | Sits with propping, rolls both ways | Transfers hand-hand, raking grasp | Consonant babble, responds to name | Stranger anxiety begins |
| 9 mo | Sits independently, crawls, pulls to stand | Inferior pincer, bangs blocks | Mama/dada non-specific, waves | Joint attention, peek-a-boo |
| 12 mo | Stands alone, cruises, first steps | Neat pincer, puts in container | 1–3 words, follows commands | Points, imitates |
| 15 mo | Walks independently, stoops | Stacks 2, scribbles | 4–6 words | Points to show, parallel play |
| 18 mo | Runs, kicks, throws | Stacks 3–4, vertical line | 10–20 words, 2-step commands | Pretend play begins |
| 2 yrs | Runs well, jumps, stairs 2-feet | Stacks 6–7, copies lines | 50+ words, 2-word phrases | Symbolic play |
| 3 yrs | Tricycle, one-foot stand 3 sec, alternates up stairs | Copies circle, draws 3-part person | 3-word sentences, 75% clear | Cooperative play, knows colors |
| 4 yrs | Hops, alternates down stairs, tandem walk | Copies cross, 6-part person | 100% clear, stories | Cooperative play, counts 10 |
| 5 yrs | Skips, hops 8–10×, catches ball | Copies triangle, writes name | 5–8 word sentences, counts 20 | Complex games, reads letters |
Key "Must-Know" Milestones (Examination Anchors)
| Milestone | Age | Domain |
|---|---|---|
| Social smile | 6 weeks–2 months | Social |
| Head control (no lag) | 4 months | Gross Motor |
| Sits independently | 6–7 months | Gross Motor |
| Neat pincer | 9–12 months | Fine Motor |
| Walks independently | 12–15 months | Gross Motor |
| First words (non-mama/dada) | 12 months | Language |
| 2-word phrases | 24 months | Language |
| Copies circle | 3 years | Fine Motor |
| Hops on one foot | 4 years | Gross Motor |
| Copies triangle | 5 years | Fine Motor |
Absolute Red Flags (Immediate Referral)
| Red Flag | Action |
|---|---|
| Any developmental regression (loss of acquired skills) | Urgent neurology referral |
| No social smile by 3 months | Developmental + ophthalmology |
| No fixing/following by 3 months | Ophthalmology + neurology |
| No babbling by 9 months | Audiology + speech therapy |
| No gestures (waving, pointing) by 12 months | ASD evaluation |
| No single words by 16 months | Speech + hearing assessment |
| No 2-word phrases by 24 months | Speech + developmental assessment |
| Not walking by 18 months | Orthopaedics/neurology |
| Persistent toe-walking after 2 years | Neurology |
| Asymmetric hand use before 12 months (always uses one hand) | Neurology — early hemiplegia |
| Hand regard after 5 months | Neurology/vision |
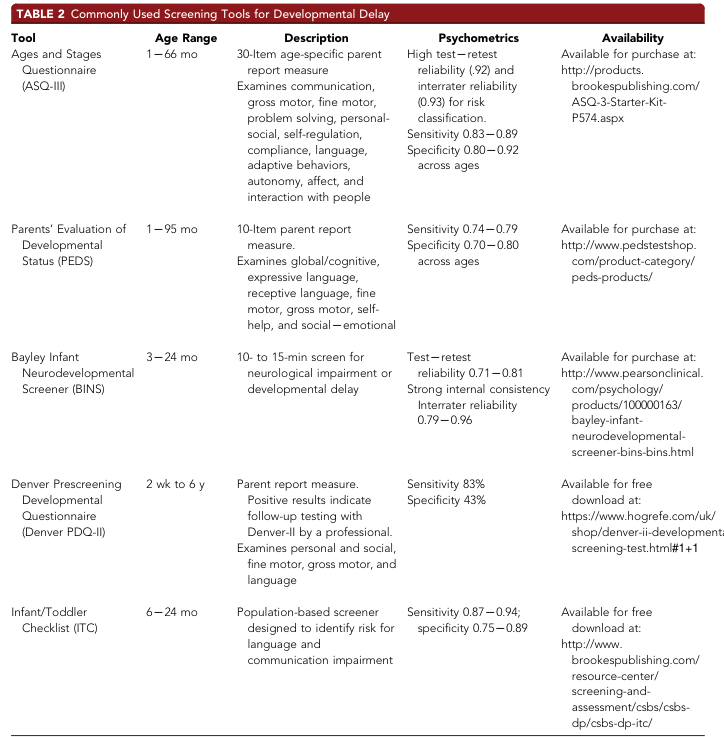
Developmental Screening Tools
| Tool | Age | Method | Notes |
|---|---|---|---|
| Ages & Stages Questionnaire (ASQ-3) | 1–66 months | Parent report | Most widely used; 5 domains |
| ASQ: Social-Emotional (ASQ:SE) | 3–66 months | Parent report | Screens for social/behavioral concerns |
| Parents' Evaluation of Developmental Status (PEDS) | 0–8 years | Parent report | 10 questions, broad screen |
| M-CHAT-R/F | 16–30 months | Parent report | Autism-specific screening |
| Denver Developmental Screening Test II (DDST-II) | 0–6 years | Clinician-administered | 125 items, 4 domains |
| Bayley Scales of Infant Development (BSID-IV) | 1–42 months | Clinician-administered | Gold standard; cognitive, language, motor |
| Griffiths Scales of Child Development | 0–8 years | Clinician-administered | 6 subscales |
| Vineland Adaptive Behavior Scales | All ages | Caregiver interview | Adaptive function; used for ID diagnosis |
Domain-Specific Examination Techniques Summary
Gross Motor Examination
- Posture at rest (supine, prone, sitting, standing)
- Transitions: roll, pull-to-sit, sit-to-stand
- Locomotion: crawl, walk, run, hop, skip, stairs
- Balance: single leg stance, tandem walk, Romberg (≥5 years)
- Ball skills: throw, catch, kick
Fine Motor Examination
- Grasp progression: palmar → raking → inferior pincer → neat pincer
- Block tower height (age-equivalent guide)
- Drawing tasks: scribble → vertical/horizontal line → circle → cross → triangle → diamond
- Drawing a person: count recognizable parts (3 at 3 yrs; 6 at 4 yrs; 10 at 5 yrs)
- Functional tasks: self-feeding, dressing, scissors
Language Examination
- Receptive: Does child follow commands? (1-step → 2-step → prepositions)
- Expressive: Number of words, combining words, sentence length, intelligibility
- Pragmatic: Eye contact, joint attention, turn-taking, pointing
- Tools: point to pictures in book, name objects, describe a scene
Social/Cognitive Examination
- Social smile, eye contact, joint attention, shared enjoyment
- Symbolic play: Does child pretend? Use objects functionally?
- Separation/stranger anxiety (normal 6–18 months; abnormal if absent)
- Theory of mind (emerges ~4 years): "Sally-Ann test"
- Imitation: facial, gestural, action
neurodeveupomtl sreenjg in destil
neurodevelopmental screening tools children developmental delay autism standardized assessment
developmental screening AAP guidelines ages stages questionnaire Denver MCHAT early intervention
neurodevelopmental screening developmental assessment chart tools children
Neurodevelopmental Screening in Detail
1. Definition & Purpose
Screening ≠ Diagnosis. A positive screen means risk — it mandates further evaluation, not a diagnosis.
- Identify delays early (before they manifest as school failure or functional impairment)
- Reduce the gap between symptom onset and diagnosis
- Enable early intervention, which has the greatest neuroplasticity benefit in the first 3–5 years of life
- Detect: Global Developmental Delay (GDD), Intellectual Disability (ID), Autism Spectrum Disorder (ASD), Language Disorders, Cerebral Palsy (CP), ADHD, Sensory Impairments
2. Guiding Principles & Policy Framework
| Organization | Recommendation |
|---|---|
| American Academy of Pediatrics (AAP) | Developmental surveillance at every well-child visit; standardized screening at 9, 18, 30 months; autism-specific screening at 18 and 24 months |
| Individuals with Disabilities Education Improvement Act (IDEA), 2004 | Mandates early identification and intervention for children 0–21 years with disabilities |
| Social Security Act (Title V) | Supports EPSDT — Early and Periodic Screening, Diagnostic, and Treatment |
| WHO | Recommends early childhood development screening as part of primary care |
3. Screening vs. Surveillance vs. Assessment
| Term | Definition | Who Does It | When |
|---|---|---|---|
| Surveillance | Ongoing, informal monitoring of development through clinical observation, history, and milestone review | All clinicians | Every visit |
| Screening | Brief, standardized test to identify children at risk | Clinician, nurse, trained staff | Scheduled visits or when concern arises |
| Diagnostic Assessment | Comprehensive, multidisciplinary evaluation to confirm diagnosis | Specialist team (pediatrician, psychologist, SLP, PT, OT) | After positive screen |
| Monitoring | Regular reassessment after a diagnosis is made | Therapy team | Ongoing |
4. Domains Assessed in Neurodevelopmental Screening
| Domain | What Is Measured | Example Concern |
|---|---|---|
| Gross Motor | Posture, locomotion, balance | Not walking by 18 months |
| Fine Motor | Hand-eye coordination, manipulation | No pincer by 12 months |
| Language (Expressive) | Spoken words, sentences, narrative | No words by 16 months |
| Language (Receptive) | Comprehension, following commands | Does not follow simple commands |
| Personal-Social | Self-care, relationships, emotional regulation | No joint attention, no eye contact |
| Cognitive / Problem-solving | Object permanence, cause-effect, learning | Cannot stack blocks, no symbolic play |
| Adaptive Behavior | Daily living skills, independence | Cannot self-feed, dress |
| Sensory | Vision, hearing, sensory processing | Does not respond to name, ignores sound |
| Behavioral/Emotional | Attention, behavior, regulation | Hyperactivity, tantrums, aggression |
5. Classification of Screening Tools
A. By Administration Method
| Type | Description | Examples |
|---|---|---|
| Parent/Caregiver Report | Questionnaire completed by parent | ASQ-3, PEDS, M-CHAT-R/F |
| Clinician-Administered | Clinician tests child directly | Denver II, BINS |
| Observational | Trained observer rates spontaneous behavior | Prechtl GMA |
| Combined | Parent report + clinician observation | CSBS-DP |
B. By Age Range
| Age | First-Line Tools |
|---|---|
| 0–6 months | Prechtl GMA, TIMP, HINE |
| 6–24 months | ASQ-3, ITC, BINS, HINE |
| 16–30 months | M-CHAT-R/F (autism) |
| 0–6 years | Denver II, PEDS, ASQ-3 |
| All ages | PEDS, Vineland-3 |
C. By Condition Targeted
| Condition | Primary Screening Tool |
|---|---|
| Global Developmental Delay | ASQ-3, PEDS, Denver II |
| Autism Spectrum Disorder | M-CHAT-R/F, CSBS-DP, ADOS-2 |
| Cerebral Palsy (early) | Prechtl GMA, HINE |
| Language Disorder | ITC, PEDS, ASQ-3 |
| Intellectual Disability | Vineland-3, ABAS-3 |
| ADHD | Vanderbilt, Conners, SNAP-IV |
| Sensory Processing | SPM, Sensory Profile-2 |
6. Detailed Profiles of Major Screening Tools
🔷 Ages and Stages Questionnaire – 3rd Edition (ASQ-3)
| Feature | Detail |
|---|---|
| Age range | 1–66 months (21 age-specific forms) |
| Type | Parent-report questionnaire |
| Time | 10–15 minutes to complete |
| Domains | Communication, Gross Motor, Fine Motor, Problem Solving, Personal-Social |
| Items | 30 items per form; Yes/Sometimes/Not yet scoring |
| Scoring | Total score per domain; cutoffs identify at-risk children |
| Sensitivity | 0.83–0.89 across ages |
| Specificity | 0.80–0.92 across ages |
| Test-retest reliability | 0.92 |
| Interrater reliability | 0.93 |
| Strengths | Widely validated, inexpensive, caregiver-friendly, multilingual |
| Limitations | Parent literacy required; does not diagnose; cultural factors |
| When to use | Routine well-child visits at 9, 18, 24/30 months; any visit with concern |
🔷 ASQ: Social-Emotional (ASQ:SE-2)
| Feature | Detail |
|---|---|
| Age range | 1–72 months (9 age-specific forms) |
| Type | Parent-report |
| Domains | Self-regulation, compliance, communication, adaptive functioning, autonomy, affect, interaction with people |
| Items | 22–36 items |
| Use | Companion to ASQ-3 for social-emotional and behavioral concerns |
| Strengths | Identifies emotional/behavioral issues missed by general screens |
🔷 Parents' Evaluation of Developmental Status (PEDS)
| Feature | Detail |
|---|---|
| Age range | 1 month–8 years |
| Type | Parent-report (10 open-ended questions) |
| Domains | Global/cognitive, expressive language, receptive language, fine motor, gross motor, self-help, social-emotional |
| Time | 2–5 minutes |
| Sensitivity | 0.74–0.79 |
| Specificity | 0.70–0.80 |
| Interpretation | Risk categorized as Significant, Non-significant, or No concerns → guides referral |
| Strengths | Very quick, conversation-based, low literacy demand |
| Limitations | Lower sensitivity than ASQ-3; broad screen only |
🔷 Denver Developmental Screening Test II (DDST-II / Denver II)
| Feature | Detail |
|---|---|
| Age range | 2 weeks – 6 years |
| Type | Clinician-administered |
| Domains | Personal-Social, Fine Motor-Adaptive, Language, Gross Motor |
| Items | 125 items plotted on age-based normative bars |
| Time | 20–30 minutes |
| Sensitivity | 83% |
| Specificity | 43% (lower — high false positive rate) |
| Scoring | Items scored as Pass/Fail/No Opportunity/Refusal; overall result: Normal / Suspect / Untestable |
| How to administer | Draw vertical line at child's chronological age; test items intersected by or just to left of line |
| Strengths | Clinician can observe behavior directly; covers 0–6 years comprehensively |
| Limitations | Time-intensive; lower specificity; requires trained examiner; not a diagnostic tool |
| Use in PT | Identifies motor and language concerns; guides referral |
🔷 Modified Checklist for Autism in Toddlers – Revised with Follow-Up (M-CHAT-R/F)
| Feature | Detail |
|---|---|
| Age range | 16–30 months |
| Type | Parent-report + structured follow-up interview |
| Items | 20 yes/no questions |
| Time | 5 minutes (screen); 5–10 min (follow-up) |
| Domains | Social communication, joint attention, pretend play, pointing, social referencing |
| Scoring | Score 0–20; Low risk (0–2), Medium risk (3–7 — do follow-up interview), High risk (8–20 or ≥2 on critical items) |
| Critical items | 2, 5, 12 (pointing, interest in other children, following a point) |
| Sensitivity | 0.87–0.95 with follow-up |
| Specificity | 0.95–0.99 with follow-up |
| Positive Predictive Value | ~47–65% for ASD (medium risk); ~94% for ASD (high risk) |
| Action | High risk → immediate ASD diagnostic referral; Medium risk → follow-up interview first |
| Availability | Free at m-chat.org |
| Strengths | Gold standard autism screen; validated; widely used globally |
| Limitations | Does not screen beyond 30 months; language barriers; misses higher-functioning ASD |
🔷 Bayley Infant Neurodevelopmental Screener (BINS)
| Feature | Detail |
|---|---|
| Age range | 3–24 months |
| Type | Clinician-administered |
| Time | 10–15 minutes |
| Domains | Neurological functions, expressive functions, receptive functions, cognitive processes |
| Scoring | Low, Moderate, or High risk classification |
| Test-retest reliability | 0.71–0.81 |
| Interrater reliability | 0.79–0.96 |
| Strengths | Specifically designed for neurological + developmental screening in infants; strong reliability |
| Use | Neonates, preterm infants, NICU follow-up |
🔷 Infant/Toddler Checklist (ITC) — CSBS-DP
| Feature | Detail |
|---|---|
| Age range | 6–24 months |
| Type | Parent-report (one-page checklist) |
| Focus | Language and communication risk — precursors to autism and language disorder |
| Domains | Social, speech, symbolic development |
| Sensitivity | 0.87–0.94 |
| Specificity | 0.75–0.89 |
| Availability | Free download |
| Strength | Identifies pre-verbal communication deficits early — before clear language delay is visible |
🔷 Prechtl's General Movements Assessment (GMA)
| Feature | Detail |
|---|---|
| Age range | Preterm → 5 months post-term |
| Type | Trained observer rates video of spontaneous movement |
| Phases assessed | Writhing movements (preterm–2 months), Fidgety movements (9–20 weeks) |
| What to observe | Quality, variability, fluency of spontaneous movement sequences |
| Key finding | Absent Fidgety Movements (FMs) at 9–20 weeks = highest predictor of cerebral palsy |
| Sensitivity for CP | >97% |
| Specificity for CP | >96% |
| Strengths | Non-invasive; best CP predictor available; can identify risk before clinical signs appear |
| Training required | Yes — standardized training course required |
| Used by | Neonatal PT, neonatologists, early intervention teams |
🔷 Hammersmith Infant Neurological Examination (HINE)
| Feature | Detail |
|---|---|
| Age range | 2–24 months |
| Type | Clinician-administered structured neurological exam |
| Sections | Cranial nerve function (6 items), Posture (8 items), Movements (3 items), Tone (4 items), Reflexes & reactions (9 items) |
| Total score | 0–78 (higher = better) |
| CP prediction | Score <40 at 6 months → high probability of CP |
| Combined with GMA + MRI | Best prediction model for CP before 6 months corrected age |
| Strengths | Standardized, validated, quick (~15 min), suitable for at-risk infants |
| Used by | Neonatal PT, developmental pediatricians |
🔷 Communication and Symbolic Behavior Scales – Developmental Profile (CSBS-DP)
| Feature | Detail |
|---|---|
| Age range | 6–24 months |
| Type | Parent questionnaire + clinician-administered behavior sample |
| Domains | Social (emotion, eye gaze, communication), Speech (sounds, words), Symbolic (understanding, play) |
| Strengths | Detects early communication and autism risk in pre-verbal children |
| Components | ITC (screen) → Caregiver Questionnaire → Behavior Sample |
7. Autism-Specific Screening in Detail
AAP ASD Screening Schedule
- M-CHAT-R/F at 18 months AND 24 months (universal)
- Additional screening whenever concern arises
M-CHAT-R/F 20 Questions (Overview)
- Enjoyment of being swung/bounced
- Interest in other children (Critical item)
- Climbing behavior
- Enjoyment of peek-a-boo/hide-and-seek
- Pretend play (Critical item — e.g., phone pretend)
- Pointing to ask for something
- Pointing to show interest
- Interest in other children
- Showing objects to caregiver
- Response to name
- Social smiling
- Following a point (Critical item)
- Motor imitation
- Response to name called
- Walking ability
- Eye contact during interaction
- Looking at caregiver's face
- Making unusual finger movements near face
- Getting caregiver's attention
- Bringing objects to show caregiver
M-CHAT-R/F Scoring Algorithm
Total score 0–2 → LOW RISK → Routine monitoring
Total score 3–7 → MEDIUM RISK → Complete Follow-Up Interview
Follow-up score 0–1 → LOW RISK
Follow-up score ≥2 → HIGH RISK → Refer for ASD evaluation
Total score 8–20 → HIGH RISK → Refer immediately for ASD evaluation
≥2 critical items failed → HIGH RISK → Refer immediately
8. Condition-Specific Screening Tools
ADHD Screening
| Tool | Age | Type | Notes |
|---|---|---|---|
| Vanderbilt Assessment Scale | 6–12 yrs | Parent + teacher | AAP-endorsed; free; ADHD + comorbidities |
| Conners 3 | 6–18 yrs | Parent + teacher + self | Comprehensive; requires purchase |
| SNAP-IV | 6–18 yrs | Parent + teacher | Free; DSM-based items |
| SDQ (Strengths & Difficulties Q) | 2–17 yrs | Parent + teacher | Emotional, behavioral, hyperactivity, peer, prosocial |
Sensory Processing Screening
| Tool | Age | Notes |
|---|---|---|
| Sensory Profile-2 (SP-2) | 0–14 yrs | Parent questionnaire; Dunn's model; 4 quadrants |
| Sensory Processing Measure (SPM-2) | 2–12 yrs | Home + school forms; 8 sensory systems |
| DeGangi-Berk Test | 3–5 yrs | Clinician-administered |
Cerebral Palsy Early Detection
| Tool | Age | Notes |
|---|---|---|
| GMA (Prechtl) | 0–5 months | Highest sensitivity/specificity for CP |
| HINE | 2–24 months | Structured neurological exam; score predicts CP |
| Developmental Assessment of Young Children (DAYC-2) | 0–5 yrs | 5 domains |
9. Standardized Screening Table (Validated Tools)
| Tool | Age Range | Sensitivity | Specificity | Time | Free? |
|---|---|---|---|---|---|
| ASQ-3 | 1–60 months | 0.83–0.89 | 0.80–0.92 | 10–15 min | Purchase |
| PEDS | 1–95 months | 0.74–0.79 | 0.70–0.80 | 2–5 min | Purchase |
| BINS | 3–24 months | — | — | 10–15 min | Purchase |
| Denver PDQ-II | 2 wks–6 yrs | 83% | 43% | 5–10 min | Free |
| ITC (CSBS-DP) | 6–24 months | 0.87–0.94 | 0.75–0.89 | 5 min | Free |
| M-CHAT-R/F | 16–30 months | 0.87–0.95 | 0.95–0.99 | 5 min | Free |
| GMA (Prechtl) | 0–5 months | >97% (CP) | >96% (CP) | 15–20 min | Training required |
| HINE | 2–24 months | High (CP) | High (CP) | 15 min | Free |
10. AAP Recommended Screening Schedule
| Age of Visit | Surveillance | Standardized Screening | ASD-Specific |
|---|---|---|---|
| Newborn | ✓ | — | — |
| 1 month | ✓ | — | — |
| 2 months | ✓ | — | — |
| 4 months | ✓ | — | — |
| 6 months | ✓ | — | — |
| 9 months | ✓ | ASQ-3 / PEDS | — |
| 12 months | ✓ | — | — |
| 15 months | ✓ | — | — |
| 18 months | ✓ | ASQ-3 / PEDS | M-CHAT-R/F |
| 24 months | ✓ | ASQ-3 / PEDS | M-CHAT-R/F |
| 30 months | ✓ | ASQ-3 / PEDS | — |
| 3 years | ✓ | — | — |
| 4 years | ✓ | — | — |
| Any visit with concern | ✓ | Appropriate tool | If ASD concern |
11. Screening Process: Step-by-Step Clinical Workflow
STEP 1: SURVEILLANCE (Every Visit)
↓
• Review developmental history
• Elicit caregiver concerns
• Observe child's behavior & interaction
• Check for red flags
STEP 2: STANDARDIZED SCREENING (Scheduled/When concern arises)
↓
• Choose age-appropriate tool (ASQ-3, PEDS, M-CHAT-R/F)
• Administer: caregiver completes OR clinician tests child
• Score: identify Pass / At Risk
STEP 3: INTERPRET RESULTS
↓
• Passed → continue surveillance, reassess at next visit
• At Risk → proceed to Step 4
STEP 4: COUNSELLING
↓
• Share results with family in plain language
• Explain what "at risk" means (not a diagnosis)
• Discuss next steps
STEP 5: REFERRAL & EARLY INTERVENTION
↓
• Refer for comprehensive diagnostic assessment
(Developmental Pediatrician, Psychologist, SLP, PT, OT)
• Refer for early intervention services (IDEA Part C: 0–3 yrs)
• Audiology & ophthalmology if sensory concern
• Genetics if dysmorphic features or family history
STEP 6: MONITOR & REASSESS
↓
• Track referral completion
• Re-screen at next visit
• Follow child's progress in therapy
12. Interpretation of Screening Results
| Result | Meaning | Action |
|---|---|---|
| Passed | Score within normal range | Continue surveillance; re-screen at next scheduled visit |
| At Risk / Failed | Score below cutoff | Does NOT mean diagnosis — refer for full assessment |
| Untestable | Child refused/uncooperative | Reschedule; note behavioral observation |
| Borderline | Score near cutoff | Rescreen in 1–3 months; intensify surveillance |
Positive Predictive Value (PPV) Note:
13. Absolute Red Flags Warranting Immediate Referral (No Waiting for Next Screen)
| Red Flag | Age | Suspected Condition |
|---|---|---|
| No social smile | >3 months | Visual impairment, ASD, GDD |
| Does not fix or follow | >3 months | Visual impairment, neurological |
| No babbling | >9 months | Hearing loss, ASD, GDD |
| No gestures (point, wave) | >12 months | ASD |
| No single words | >16 months | Language disorder, ASD |
| No 2-word phrases | >24 months | Language disorder, ASD, GDD |
| Any regression at any age | Any | Urgent — Rett syndrome, epileptic encephalopathy, metabolic disorder |
| Not walking independently | >18 months | CP, neuromuscular, orthopaedic |
| Asymmetric hand use | <12 months | Hemiplegia |
| Seizures | Any | Neurology referral |
| Abnormal head circumference (macro/microcephaly) | Any | Genetics, neurology |
14. Role of Physiotherapy in Neurodevelopmental Screening
| PT Role | How |
|---|---|
| First-contact screener | PT in community/school can administer ASQ-3, observe motor milestones |
| Motor domain specialist | Detailed gross and fine motor assessment; GMA-trained PTs in neonatal units |
| HINE administration | Neonatal PT uses HINE for CP early detection |
| Prechtl GMA | Video-based assessment of writhing and fidgety movements in NICU and early follow-up clinics |
| Multidisciplinary team | PT contributes motor assessment findings to diagnostic team |
| Early intervention | PT provides therapy once risk is identified — does not wait for formal diagnosis |
| Family education | PT teaches caregivers developmental play activities and red flags to watch for |
15. Summary: Choosing the Right Tool
Child 0–5 months (at-risk/NICU)
→ Prechtl GMA + HINE
Child 1–66 months (routine well-child)
→ ASQ-3 (first choice)
→ PEDS (quick alternative)
Child 16–30 months (autism concern)
→ M-CHAT-R/F
Child 6–24 months (language/communication concern)
→ ITC (CSBS-DP)
Child 3–24 months (neurological concern, NICU follow-up)
→ BINS
Child 2 weeks–6 years (clinical observation preferred)
→ Denver II
Child with confirmed delay (quantify function/adaptive behavior)
→ Vineland-3, Bayley-4, ABAS-3
Child with ADHD concern
→ Vanderbilt (free), Conners-3
Child with sensory concern
→ Sensory Profile-2, SPM-2
ACCORDIN TO THIS TRICKS FOR OBSERVATION PAPTION EXAMINATION
observation tricks pediatric neurological examination techniques
pediatric physiotherapy assessment spontaneous movement quality infant observation
Tricks for Observation in Pediatric Neurological/Physiotherapy Examination
1. Observe Before You Approach
| Setting | What to Observe |
|---|---|
| Child in parent's lap at entry | Postural tone, head control, spontaneous movement |
| Child walking in/playing in waiting room | Gait pattern, balance, coordination, arm swing symmetry |
| Child during undressing | Limb preference, dexterity, pain behavior |
| Child during free play with toys | Fine motor, hand dominance, problem-solving, attention |
Tip: Spend the first 2–3 minutes just talking to the parent while casually watching the child. This is the most unguarded, neurologically "honest" window you'll have.
2. Use the Parent as a Buffer
- Conduct the entire initial history while the child stays in the parent's lap — this reduces threat perception.
- Ask the parent to hand the child a toy while you talk — you observe the reach, grasp, and transfer.
- Watch the parent–child interaction: Is the parent anxious or detached? Does the child seek comfort? Social-emotional development is embedded in this dyad.
- Reciprocal gaze between parent and infant is a sensitive early marker of social development and cortical function.
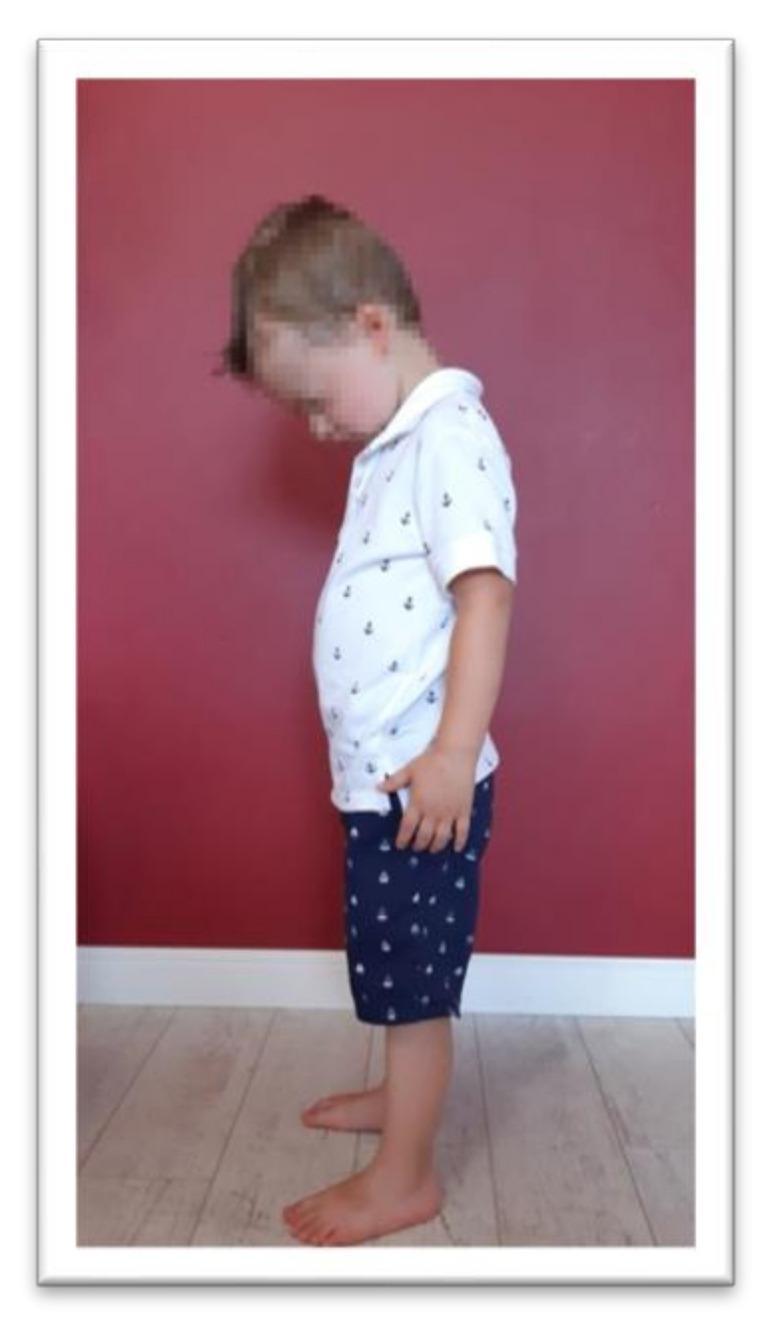
3. Resting Posture: Read the "Default State"
| Posture Finding | Likely Significance |
|---|---|
| Persistent fisting (thumb adducted) after 3 months | Upper motor neuron sign, corticospinal tract involvement |
| Asymmetric tonic neck reflex (ATNR) posturing at rest after 6 months | Persistent primitive reflex, suggests CNS immaturity |
| Opisthotonus (neck/back arching) | Meningeal irritation, kernicterus, severe tone disorder |
| Hypotonia — "frog-leg" position in supine | Lower motor neuron or cerebellar pathology |
| Scissoring of legs in vertical suspension | Spastic diplegic/quadriplegic pattern (e.g., cerebral palsy) |
| Asymmetric spontaneous limb movement | Hemiplegia — the affected limb moves less spontaneously |
4. Observe Spontaneous Movement Quality (Prechtl GMA Approach)
- Writhing movements (preterm to ~2 months): Should be complex, variable, fluent. If cramped-synchronized → high risk for CP.
- Fidgety movements (~3–5 months corrected): Small, circular, continuous movements of neck/trunk/limbs. Absence of fidgety movements has >95% sensitivity for CP.
5. Distraction Techniques to Elicit Authentic Responses
| Technique | Purpose |
|---|---|
| Bubbles blown toward the child | Tests tracking (smooth pursuit), visual attention, head turning |
| Rolling a ball on the floor | Elicits crawling, reaching, weight shift — assesses gross motor without formal testing |
| Rattles/squeaky toys at midline and sides | Tests auditory localization, head righting, reaching |
| Colorful spinning toy | Tests fixation, convergence, visual pursuit in infants |
| Phone screen with a video/cartoon | Tests sustained attention, visual processing, language response |
| Stacking blocks or posting shapes | Fine motor, bilateral coordination, cognitive problem-solving |
| Blowing a party whistle or bubbles yourself | Elicits imitation (12–18 months), oral-motor function |
Key tip: Always have 2–3 toys of different types available. Toy-switching also lets you observe bilateral hand use and transfer, a key milestone.
6. Gait and Movement Observation Tricks
- Ask the parent to walk the toddler down the corridor before entering — you observe unguarded natural gait.
- Ask an older child to run to a parent at the end of the room — running reveals subtle hemiplegia and coordination issues more clearly than walking.
- Tandem walking (heel-to-toe) is best observed by making it a game ("walk on the line like a tightrope walker").
- Watch arm swing during walking — unilateral reduction is a sensitive early sign of hemiparesis.
- Toe-walking should always be noted: idiopathic, spastic CP, or early ASD/sensory processing disorder.
- Ask the child to kick a ball — reveals weight-shifting ability and limb preference.
7. Functional Observation as a Neurological Proxy
| Functional Activity | What It Tests Neurologically |
|---|---|
| Feeding (infant at breast/bottle) | Oral-motor coordination, suck-swallow-breathe rhythm, hypotonia |
| Reaching for an object | Intentional movement, tone, shoulder girdle stability |
| Picking up a small pellet (Cheerio/raisin) | Pincer grasp maturation — cortical fine motor control |
| Turning pages / scribbling | Fine motor, visual-motor integration |
| Climbing onto a chair | Proximal strength, motor planning (praxis) |
| Undressing (socks, shoes) | Motor planning, bilateral coordination, problem-solving |
8. Neurobehavioral Observation Cues
| Observation | Significance |
|---|---|
| No social smile by 2 months | Possible visual impairment, cortical dysfunction, or ASD risk |
| No eye contact or gaze following | ASD spectrum concern, cortical visual impairment |
| No response to name at 9–12 months | ASD, hearing loss, cognitive delay |
| Excessive mouthing/drooling past 18 months | Oral hypotonia, motor planning difficulties |
| Stereotyped hand movements (flapping, wringing) | ASD, Rett syndrome |
| Reduced blink rate / staring spells | Absence seizures, visual processing issues |
| Irritability / hyperekplexia (excessive startle) | Hyperekplexia syndrome, metabolic disorders |
9. Observing Tone Without Formal Testing
- Scarf sign equivalent: Watch how the infant holds their arms — do they stay folded or swing freely?
- Head lag during transitions: Does the caregiver handle the child with extra head support? Parents unconsciously compensate for hypotonia.
- Sitting posture: A hypotonic child will sit in a "W-sit" or lean heavily on hands; a hypertonic child will be stiff and resist posture transitions.
- Quality of reaching: Stiff, guarded reaching with forearm pronation = upper motor neuron pattern.
10. Environmental and Behavioral Cues
| Cue | Interpretation |
|---|---|
| Child clings to parent, refuses all interaction | Normal stranger anxiety (6–18 months) — do not pathologize |
| Child is completely indifferent to separation | Consider ASD, attachment disorder, or cognitive delay |
| Extreme sensitivity to light/sound in clinic | Sensory processing disorder, migraine, meningism |
| Child examines room systematically but ignores people | Cognitive strength, social interest deficit — ASD screen |
| Child uses parent's hand as a tool (hand-leading) | Classic ASD sign |
| Child responds to non-verbal cues but not speech | Selective hearing vs. language disorder vs. hearing loss |
Summary Mnemonic: "POSTARE"
| Letter | Trick |
|---|---|
| P | Posture at rest — what does the default state tell you? |
| O | Observe before touch — unguarded behavior is the most valuable |
| S | Spontaneous movement — Prechtl quality, asymmetry, absence |
| T | Tone estimate from observation — lag, slump, stiffness |
| A | Age-appropriate distraction — toys, bubbles, games |
| R | Relational cues — parent–child interaction, eye contact, social smile |
| E | Environment responses — sensory reactivity, stranger anxiety, separation |
HIGHER MENATL FUNTION EXAMINATION IN DEATIL I PEDS
higher mental function examination children pediatric cognitive assessment
pediatric neuropsychological assessment memory attention language executive function
Higher Mental Function (HMF) Examination in Pediatrics — In Detail
Domains of Higher Mental Function
| Domain | Cortical Substrate |
|---|---|
| Consciousness & Arousal | Reticular activating system + thalamus |
| Orientation | Parietal, temporal lobes |
| Attention | Prefrontal cortex, anterior cingulate |
| Memory | Hippocampus, temporal lobes |
| Language | Broca's (L frontal), Wernicke's (L temporal) |
| Visuospatial function | Right parietal lobe |
| Executive function | Prefrontal cortex |
| Praxis | Left parieto-frontal network |
| Gnosis | Parieto-occipital association cortex |
| Behavior / Affect | Frontal lobe, limbic system |
| Intelligence / Reasoning | Diffuse, frontoparietal dominant |
1. Consciousness and Arousal
Tools:
- AVPU Scale (quick, any age): Alert / Voice / Pain / Unresponsive
- Glasgow Coma Scale (GCS) — Pediatric modification used for children <5 years:
| Component | Adult/Older Child | Pediatric Modification (<5 yrs) |
|---|---|---|
| Eye Opening | 1–4 | Same |
| Verbal | 1–5 | Modified: coos/babbles (5), irritable cry (4), cries to pain (3), moans (2), none (1) |
| Motor | 1–6 | Same, but "localizes" interpreted as age-appropriate purposeful movement |
- Full score: 15 — Scores ≤8 = severe impairment (intubation threshold)
What to observe:
- Is the child awake and alert on entry?
- Do they orient to voice/face without excessive latency?
- Note drowsiness, fluctuating alertness, or hyperarousal (all are abnormal)
2. Orientation
| Age | Expected Orientation |
|---|---|
| 2–3 years | Knows own name, recognizes parents |
| 4–5 years | Knows full name, age, town/city |
| 6–7 years | Knows day, month, school name |
| 8+ years | Full time orientation (day, date, month, year) |
How to test:
- "What is your name?" / "How old are you?"
- "Where are we right now?" / "What is the name of your school?"
- "What day is today?" / "What month?" (school-age)
- "Why did you come here today?" — tests situational orientation
Tip: A confused, disoriented child in a clear state of consciousness suggests toxic-metabolic encephalopathy, post-ictal state, or raised ICP.
3. Attention
Components:
| Type | Definition | How to Test |
|---|---|---|
| Sustained attention | Maintain focus over time | Continuous Performance Test (CPT); count backward from 20 |
| Selective attention | Focus on target, ignore distractors | Digit cancellation task; find all "A"s on a page |
| Divided attention | Attend to two things at once | Recite alphabet while tapping; dual-task walking |
| Shifting attention | Switch between tasks | Trail Making Test B; "Day-Night" task |
Bedside Tests by Age:
| Age | Test |
|---|---|
| 3–4 years | Follow a 2-step command without gestural cues |
| 5–6 years | Digit span forward (normal: 4 digits); name colors in sequence |
| 7–9 years | Serial 3 subtraction from 20; Days of the week backwards |
| 10+ years | Serial 7 subtraction from 100; Months of the year backwards |
- Age 5: 4 digits
- Age 7: 5 digits
- Age 10: 6 digits
- Adult: 7 ± 2
Clinical flag: Digit span <3 at any age above 5, inability to hold a 2-step command, or constant distractibility → screen for ADHD, frontal pathology, or intellectual disability.
4. Memory
Three Stages:
- Encoding (registering information)
- Storage / Consolidation (hippocampal processing)
- Retrieval (access from storage)
Types and Testing:
| Memory Type | Substrate | Bedside Test |
|---|---|---|
| Immediate memory | Working memory (prefrontal) | Digit span; repeat 3 words immediately |
| Short-term (recent) memory | Hippocampus | Recall 3 words after 5 minutes; "What did you have for breakfast?" |
| Long-term (remote) memory | Neocortex | "What was the name of your last school?" / family members' names |
| Episodic memory | Hippocampus + prefrontal | "Tell me about your last birthday party" |
| Semantic memory | Temporal lobe | "What is a dog?" / "Name 5 fruits" |
| Procedural memory | Basal ganglia, cerebellum | Demonstrated in motor tasks — tying laces, riding a bike |
| Prospective memory | Frontal lobe | "Remember to remind me when we finish" |
Practical 3-Word Test (Modified for Age):
- Age 4–5: Use 3 objects placed on the table (car, cup, pen) → ask recall after 5 mins
- Age 6+: Use 3 spoken words (apple, table, London) → immediate recall → recall at 5 mins
- Normal: Recall 2–3/3 after 5 minutes
Key distinction: Failure of immediate recall = attention/encoding problem. Failure of delayed recall with intact immediate = true amnestic syndrome (hippocampal).
5. Language
Components of Language:
| Component | What to Test | How |
|---|---|---|
| Comprehension | Understanding spoken language | 1-step → 3-step commands; point to body parts; "Put the pen on the book then clap" |
| Expression / Fluency | Spontaneous speech output | Observe during conversation; note word-finding pauses, circumlocutions |
| Naming | Object naming | Show pen, watch, stethoscope, coin, shoe — "What is this?" |
| Repetition | Repeat sentences | "No ifs, ands, or buts" / "The boy walked to school" |
| Reading | Age-appropriate reading aloud | Graded word/sentence card |
| Writing | Write name / sentence | Age-appropriate |
| Phonology | Sound production | "Say: pa-ta-ka" rapidly |
Language Milestones (Developmental Norms):
| Age | Expected Language |
|---|---|
| 12 months | 1–2 meaningful words; mama/dada with intent |
| 18 months | 10–20 words; follows 1-step commands |
| 24 months | 50+ words; 2-word phrases; 50% intelligible to strangers |
| 3 years | 3–4 word sentences; asks "why/what"; 75% intelligible |
| 4 years | Tells a story; uses past tense; 100% intelligible |
| 5 years | Full sentences; narrative; grammar near adult |
| 6–7 years | Reads simple words; phonemic awareness |
| 8+ years | Fluent reading; complex grammar; metaphors |
Aphasia Classification in Children (Acquired):
| Type | Fluency | Comprehension | Repetition | Lesion |
|---|---|---|---|---|
| Broca's | Non-fluent | Intact | Impaired | Left inferior frontal |
| Wernicke's | Fluent (jargon) | Impaired | Impaired | Left superior temporal |
| Conduction | Fluent | Intact | Severely impaired | Arcuate fasciculus |
| Global | Non-fluent | Impaired | Impaired | Large left MCA territory |
| Anomic | Fluent | Intact | Intact | Variable |
Note: Children rarely present with classic adult aphasia patterns post-stroke due to cerebral plasticity — right hemisphere compensates significantly before age 10.
6. Visuospatial and Visuoconstructive Function
Tests by Age:
| Age | Test |
|---|---|
| 2–3 years | Match shapes; complete a simple formboard puzzle |
| 3–4 years | Copy a circle; recognize faces in pictures |
| 4–5 years | Copy a cross (+); draw a person (Goodenough Draw-A-Person) |
| 5–6 years | Copy a square; basic jigsaw puzzles |
| 6–7 years | Copy a triangle/diamond; block designs |
| 8+ years | Copy Rey-Osterrieth Complex Figure (ROCF); 3D cube drawing |
- Score = number of body parts/details drawn
- Each feature = 1 year of developmental age (rough approximation)
- Reliable from age 3–10 years
- Draw a clock face → place numbers → set hands to 10:10
- Tests visuospatial planning, number knowledge, executive function simultaneously
What deficits indicate:
| Finding | Interpretation |
|---|---|
| Hemispatial neglect (ignores left side of drawing) | Right parietal lesion |
| Poor constructional ability with good copying | Frontal planning deficit |
| Mirror writing/reversal of letters | Normal up to age 7; dyslexia if persistent |
| Cannot recognize faces (prosopagnosia) | Right occipito-temporal lesion |
7. Executive Function
Components and Tests:
| EF Component | Definition | Bedside/Formal Test |
|---|---|---|
| Inhibition | Suppress a prepotent response | Go/No-Go task; Stroop Color-Word test; "Don't say yes" game |
| Working memory | Hold and manipulate information | Digit span backward; Letter-Number Sequencing |
| Cognitive flexibility | Shift mental set | Trail Making Test B; WCST (Wisconsin Card Sorting) |
| Planning | Sequence steps toward a goal | Tower of London/Tower of Hanoi; "How would you make a sandwich?" |
| Fluency | Generate items within a category | Name as many animals as you can in 1 minute (>12 for age 7+) |
| Abstract reasoning | Proverbs, analogies | "What does 'spilled milk' mean?" / "How are a dog and a cat alike?" |
| Judgment/insight | Understand consequences | "What would you do if you found a wallet?" |
Age-Appropriate EF Expectations:
| Age | Normal EF Capacity |
|---|---|
| 3–4 years | Simple rule-following; inhibits reaching for a reward briefly |
| 5–6 years | Follows 2–3 step rules; understands "wait"; basic planning |
| 7–9 years | Organizes tasks; basic abstract thinking; understands consequences |
| 10–12 years | Multi-step planning; handles ambiguity; perspective-taking |
| 12–14 years | Hypothesis testing; complex analogies; moral reasoning |
| 16+ years | Near-adult EF; complex decision making |
Flag: EF deficits are the hallmark of ADHD, frontal lobe epilepsy, TBI, and autism spectrum disorder. They are frequently missed because the child may have intact IQ and memory.
8. Praxis
Types:
| Type | Description | Test |
|---|---|---|
| Ideomotor apraxia | Impaired isolated movement on command | "Show me how to wave goodbye / comb your hair / use a toothbrush" — without the object |
| Ideational apraxia | Impaired sequencing of multi-step acts | "Pretend to fold a letter, put it in an envelope, and seal it" |
| Constructional apraxia | Impaired assembly/building | Block designs; ROCF copy; matchstick patterns |
| Gait apraxia | Inability to initiate walking despite intact motor/sensory | Observed on walking; "magnetic gait" |
| Oral/bucco-facial apraxia | Impaired voluntary oral movements | "Stick out your tongue / blow a kiss / click your teeth" |
| Dressing apraxia | Cannot organize clothing to body | Observe undressing/dressing |
In children, developmental dyspraxia / DCD (Developmental Coordination Disorder) is the most common praxis disorder — clumsy, poor handwriting, difficulty learning new motor skills, without primary motor or sensory lesion.
9. Gnosis (Agnosia)
| Type | Description | Test |
|---|---|---|
| Visual agnosia | Cannot name/recognize objects by sight | Place object in front: "What is this?" — if fails, allow to touch |
| Tactile agnosia (astereognosis) | Cannot recognize objects by touch | Eyes closed: place a coin, key, button in hand — "What is this?" |
| Prosopagnosia | Cannot recognize familiar faces | Show photos of family members / famous characters |
| Finger agnosia | Cannot identify which finger is touched | "Which finger did I touch?" (eyes closed) |
| Color agnosia | Cannot name colors despite seeing them | Point to red/blue/green; name colors of objects |
| Body schema (autotopagnosia) | Cannot identify body parts on self or examiner | "Show me your elbow / right knee / left ear" |
10. Behavior, Affect, and Insight
| Feature | Observations | Significance |
|---|---|---|
| Affect | Flat, blunted, labile, euphoric | Frontal lobe pathology, mood disorder, TBI |
| Disinhibition | Impulsivity, inappropriate comments, touching objects | Orbitofrontal cortex lesion, ADHD, manic episodes |
| Perseveration | Repeating same answer/movement | Frontal/subcortical pathology |
| Concrete thinking | Interprets everything literally | Frontal immaturity, ASD, intellectual disability |
| Insight | Awareness of their own difficulties | "Do you find reading hard?" — poor insight in frontal lesions |
| Social cognition | Reading emotions, theory of mind | Ask: "What is this person feeling?" (show emotional face pictures) — impaired in ASD |
Structured HMF Examination Sequence (Bedside Protocol)
1. CONSCIOUSNESS → AVPU / GCS pediatric
2. ORIENTATION → Person → Place → Time → Situation
3. ATTENTION → Digit span / serial subtraction / command-following
4. MEMORY → 3 words: immediate + 5-minute recall
5. LANGUAGE → Spontaneous speech → naming → comprehension → repetition
6. VISUOSPATIAL → Draw a person / copy shapes / clock drawing (age-appropriate)
7. EXECUTIVE → Fluency / abstraction / Go-No-Go / planning task
8. PRAXIS → "Show me how to comb your hair / wave / fold paper"
9. GNOSIS → Identify objects by sight/touch; finger recognition
10. BEHAVIOR/AFFECT → Observed throughout; social cognition probe
Standardized Tools for Formal HMF Assessment in Children
| Tool | Age Range | Domains | Use |
|---|---|---|---|
| WISC-V (Wechsler) | 6–16 years | IQ, working memory, processing speed, VCI, PRI | Gold standard IQ + cognitive profile |
| WPPSI-IV | 2.5–7 years | IQ domains adapted for young children | Pre-school cognitive assessment |
| NEPSY-II | 3–16 years | Attention, memory, language, visuospatial, EF, sensorimotor | Comprehensive neuropsychological battery |
| KABC-II | 3–18 years | Sequential/simultaneous processing, learning, planning | Kaufman battery — culturally fair |
| BRIEF-2 | 5–18 years | Executive function (parent/teacher rating scale) | Behavioral EF rating in real-world settings |
| CMS (Children's Memory Scale) | 5–16 years | Memory: verbal, visual, attention/concentration | Memory disorder diagnosis |
| PDMS-2 | 0–5 years | Gross + fine motor with cognitive components | Early childhood |
| Conners-3 | 6–18 years | ADHD symptom profiling | Attention/EF behavioral rating |
| Vineland-3 | Any age | Adaptive behavior (real-world function) | ID, ASD |
Summary: HMF by Domain — Key Clinical Flags
| Domain | Key Red Flag |
|---|---|
| Attention | Digit span <3 at age ≥5; cannot follow 2-step commands |
| Memory | Immediate recall intact but no delayed recall = hippocampal lesion |
| Language | Regression of language at any age = urgent investigation |
| Visuospatial | Neglect; cannot copy basic shapes for age |
| Executive | Severe perseveration, disinhibition, no planning ability |
| Praxis | Cannot perform learned motor acts on command |
| Gnosis | Fails to recognize objects by sight while primary vision is intact |
| Behavior | Personality change, loss of empathy, disinhibition = frontal alarm |