expali in deatil goal and pt mnagment for post op mastectomy describe phases of rehab after breas surgery assessment and maagement of shoulder dysfunccyion after mastetcomy in detail
Reading File
search_medical_text
post operative mastectomy physiotherapy goals patient management rehabilitation
search_medical_text
phases of rehabilitation after breast cancer surgery exercise program
search_medical_image
post mastectomy shoulder rehabilitation exercises lymphedema
GradeResponse
GradeResponse
GradeResponse
search_medical_text
shoulder dysfunction after mastectomy axillary lymph node dissection assessment range of motion
search_medical_text
breast cancer surgery complications lymphedema cording axillary web syndrome management
Here is a comprehensive, clinically structured answer drawing from retrieved sources and established evidence-based practice.
Post-Operative Mastectomy: Goals, Patient Management, Rehabilitation Phases & Shoulder Dysfunction
1. GOALS OF POST-OPERATIVE MANAGEMENT AFTER MASTECTOMY
The overarching aim of post-mastectomy rehabilitation is to restore full functional independence, minimize surgical morbidity, and support the patient's physical and psychological recovery. Goals are staged across time:
Immediate/Acute Goals (Days 1–7)
| Goal | Rationale |
|---|---|
| Pain control | Prevents splinting, guarded posture, and early shoulder stiffness |
| Wound healing and infection prevention | Seromas/dehiscence are common early complications |
| Prevention of DVT/pulmonary embolism | Early mobilization is key |
| Drain management education | Surgical drains are usually in place 5–14 days |
| Posture awareness | Prevents forward head/rounded shoulder compensation pattern |
| Early gentle shoulder mobilization | Prevents capsular contracture, adhesions |
| Psychological support | Adjustment to body image, grief, anxiety |
| Patient education | Activity restrictions, lymphedema precautions, warning signs |
Short-Term Goals (Weeks 1–6)
- Full, pain-free shoulder ROM (flexion, abduction, external rotation)
- Reduce post-surgical edema and seroma risk
- Restore normal scapular mechanics
- Scar tissue mobility and desensitization
- Return to activities of daily living (ADLs)
- Lymphedema surveillance and early intervention
Long-Term Goals (Months 2–12+)
- Full upper extremity strength and endurance
- Normal neuromuscular control of the shoulder girdle
- Prevention or management of lymphedema
- Return to recreational and occupational activities
- Optimize quality of life and reduce cancer-related fatigue
- Psychological well-being and social reintegration
2. PHASES OF REHABILITATION AFTER BREAST SURGERY
Rehabilitation is divided into four phases, each with specific criteria for progression.
Phase 1 — Acute/Inpatient Phase (Days 1–7)
Setting: Hospital or immediate post-discharge home
Key Priorities:
- Deep breathing exercises and incentive spirometry (prevent atelectasis, pain management)
- Gentle hand, wrist, and elbow ROM — full range permitted immediately
- Shoulder ROM is restricted if drains are in place — typically limited to 90° shoulder flexion/abduction to prevent seroma and drain dislodgement
- Positioning: elevate arm on pillow, avoid dependent positioning
- Ambulation and lower limb exercises to prevent DVT
- Edema monitoring — baseline arm circumference measurements
Patient Education:
- Lymphedema precautions (avoid BP cuffs, blood draws, tight clothing on affected arm)
- Signs of infection, seroma, or hematoma
- Activity restrictions (no lifting >1 kg initially)
- Scar care post-wound closure
Contraindications at this stage:
- No aggressive shoulder stretching while drains are present
- No resistive exercise
- Avoid extreme positions that increase seroma risk
Phase 2 — Early Rehabilitation (Weeks 2–6, Post-Drain Removal)
Trigger for progression: Drain removal (usually when output <30 mL/24 hours)
Goals:
- Restore full shoulder ROM progressively
- Normalize scapulothoracic rhythm
- Begin soft tissue mobilization around incision
- Gentle aerobic reconditioning
Exercises Introduced:
| Exercise | Purpose |
|---|---|
| Pendulum (Codman) exercises | Gravity-assisted glenohumeral distraction |
| Active-assisted shoulder flexion (wand/pulley) | Restore overhead range |
| Wall climbing (finger walking) | Progressive shoulder flexion and abduction |
| Shoulder external rotation stretches | Prevent capsular tightening |
| Pectoralis minor stretching | Counter surgical shortening of anterior chest |
| Scapular retraction and depression | Restore scapular kinematics |
| Cervical ROM exercises | Address cervical compensatory patterns |
| Scar massage (once healed, ~3–4 weeks) | Prevent adherent scar, improve tissue mobility |
Monitoring:
- ROM measured at each visit (goniometry)
- Limb girth measurements (lymphedema surveillance)
- Pain score assessment (VAS/NRS)
- Wound healing status
Phase 3 — Progressive Strengthening Phase (Weeks 6–12)
Goals:
- Restore rotator cuff and periscapular strength
- Normalize upper extremity strength symmetry
- Begin functional task training
- Aerobic fitness reconditioning
Exercises:
- Rotator cuff strengthening: internal/external rotation with resistance bands
- Serratus anterior activation: wall push-ups, protraction exercises
- Lower/middle trapezius strengthening: rows, prone Y/T/W exercises
- Progressive resistance training: light dumbbells, resistance bands
- Postural correction exercises: thoracic extension over foam roller
- Aerobic exercise: walking, stationary cycling — building to 150 min/week moderate intensity
Evidence Base: Exercise during and after breast cancer treatment is supported by the ACSM (American College of Sports Medicine) exercise guidelines for cancer survivors. Supervised cancer-specific exercise programs are recommended for patients with comorbidities or treatment toxicities (Exercise, Diet, and Weight Management During Cancer Treatment, p. 8). Many patients can safely transition to unsupervised home programs after initial supervised rehabilitation.
Important Considerations:
- Monitor for axillary web syndrome ("cording") — tight bands in axilla with arm elevation
- Screen for signs of lymphedema before each session
- Avoid blood pressure cuffs and venipuncture on the affected arm
Phase 4 — Return to Function and Long-Term Maintenance (Months 3–12+)
Goals:
- Full return to occupational and recreational activities
- Continued lymphedema management
- Psychological adaptation
- Cancer surveillance integration
Components:
- High-level resistance training progression
- Occupational task simulation
- Sports-specific training if applicable
- Ongoing lymphedema monitoring ± compression garment use
- Fatigue management strategies
- Bone health (osteoporosis risk with chemotherapy/hormonal therapy)
- Psychosocial support — support groups, counselling referral
3. ASSESSMENT OF SHOULDER DYSFUNCTION AFTER MASTECTOMY
Shoulder dysfunction occurs in 30–67% of women after mastectomy with axillary lymph node dissection (ALND), and in lower percentages after sentinel lymph node biopsy (SLNB).
Subjective Assessment
History:
- Type and extent of surgery (total mastectomy, modified radical, radical, skin-sparing, nipple-sparing)
- Axillary intervention (SLNB vs. ALND — ALND carries significantly higher morbidity)
- Adjuvant therapy (radiation to axilla/chest wall worsens fibrosis; chemotherapy causes neuropathy)
- Pre-surgical shoulder function baseline
- Dominant hand status
Symptoms to Explore:
- Pain (location, nature, severity — NRS 0–10)
- Stiffness and restricted movement
- Weakness (difficulty lifting, overhead tasks)
- Numbness or tingling (intercostobrachial nerve distribution — medial upper arm)
- Swelling (arm, hand, breast area)
- Tight bands/cords in axilla (axillary web syndrome)
- Sleep disturbance due to shoulder pain
- Psychological distress and fear of movement (kinesiophobia)
Objective Assessment
1. Posture and Observation
- Forward head, protracted shoulder, depressed affected shoulder
- Trunk lateral flexion toward affected side
- Scapular winging or tipping
- Breast asymmetry, chest wall deformity
- Skin color changes, visible swelling of upper extremity
As shown in the clinical photograph below, radical mastectomy can result in significant chest wall deformity, depressed and medially rotated shoulder, and post-mastectomy lymphedema with markedly restricted shoulder abduction:
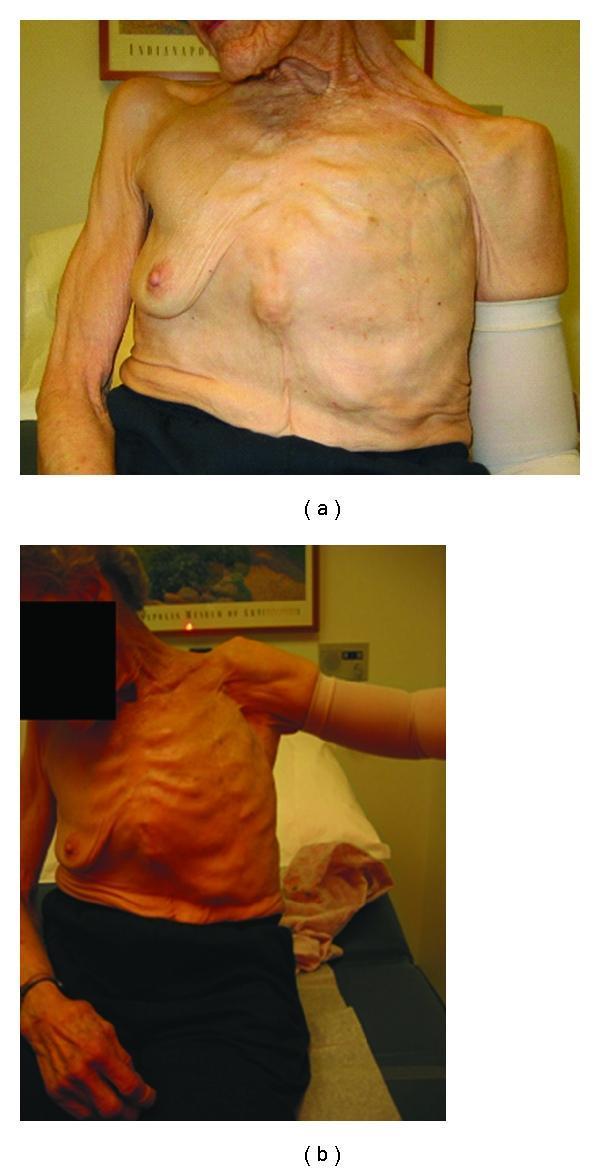
(Clinical image: Long-term sequelae of radical left mastectomy — chest wall deformity, shoulder depression/internal rotation, post-mastectomy lymphedema managed with compression sleeve, restricted shoulder abduction)
2. Range of Motion Assessment
Goniometric measurement of the affected vs. contralateral shoulder:
| Movement | Normal | Post-Mastectomy Red Flag |
|---|---|---|
| Shoulder Flexion | 0–180° | <120° at 6 weeks = significant restriction |
| Shoulder Abduction | 0–180° | Asymmetry >15° requires intervention |
| External Rotation | 0–90° | Often restricted from anterior scarring |
| Internal Rotation | 0–70° | |
| Horizontal Adduction | 0–130° |
- Document the end feel (soft/firm/hard — fibrotic capsule vs. muscular guarding vs. bony block)
- Assess for painful arc (subacromial impingement pattern common post-surgery)
3. Muscle Strength Testing
- Manual Muscle Testing (MMT) — graded 0–5
- Key muscles assessed:
- Serratus anterior (long thoracic nerve injury risk with ALND)
- Trapezius (spinal accessory nerve at risk in extensive dissections)
- Pectoralis major/minor (resected in radical mastectomy)
- Deltoid, rotator cuff (secondary weakness from disuse/pain inhibition)
- Latissimus dorsi (may be used in reconstruction flap)
4. Neurological Assessment
Post-ALND nerve injuries are common:
| Nerve | Injury Consequence |
|---|---|
| Intercostobrachial nerve | Numbness/dysesthesia medial upper arm (most common) |
| Long thoracic nerve | Serratus anterior palsy → winged scapula |
| Thoracodorsal nerve | Latissimus dorsi weakness |
| Medial pectoral nerve | Pectoralis minor weakness |
| Brachial plexus | Radiation-induced plexopathy (delayed, months–years post-RT) |
- Sensory testing: light touch, pin prick, vibration in dermatomal distributions
- Reflexes: biceps, triceps, brachioradialis
- Screen for radiation-induced brachial plexopathy if prior axillary radiation
5. Lymphedema Assessment
- Arm circumference measurements at standardized landmarks (olecranon, +10 cm, –10 cm, wrist)
- Bioimpedance spectroscopy (L-Dex) — gold standard for early subclinical detection
- Volume by water displacement
- Skin changes: pitting vs. non-pitting, fibrosis, skin texture changes
- Stemmer's sign (skin fold at base of finger — positive = lymphedema)
- International Society of Lymphology (ISL) Staging:
| Stage | Description |
|---|---|
| 0 | Subclinical — no swelling, abnormal transport |
| I | Pitting edema, reduces with elevation |
| II | Non-pitting, does not reduce with elevation |
| III | Lymphostatic elephantiasis, skin changes |
6. Axillary Web Syndrome (Cording) Assessment
- Palpate axilla and medial arm for fibrous cord-like structures
- Visible/palpable taut bands from axilla along medial arm to wrist
- Presents typically 2–8 weeks post-surgery
- Restricts shoulder flexion and elbow extension
- Assessed with shoulder flexion + elbow extension provocation test
7. Functional Outcome Measures
| Tool | What It Measures |
|---|---|
| DASH (Disabilities of the Arm, Shoulder, Hand) | Upper extremity disability |
| QuickDASH | Abbreviated UE function |
| FACT-B (Functional Assessment Cancer Therapy – Breast) | Cancer-specific QoL |
| EORTC QLQ-BR23 | Breast cancer QoL |
| VAS/NRS | Pain intensity |
| Constant-Murley Score | Shoulder function |
| Southampton Hand Assessment Procedure | Hand function |
4. MANAGEMENT OF SHOULDER DYSFUNCTION AFTER MASTECTOMY
A. Physiotherapy Interventions
Manual Therapy
- Glenohumeral joint mobilizations (Maitland Grades I–IV) for capsular restriction
- Scar tissue mobilization — transverse friction massage, instrument-assisted (IASTM)
- Myofascial release — pectoralis major/minor, anterior chest wall, cervical region
- Axillary web syndrome (cording) treatment:
- Progressive shoulder abduction and elbow extension stretching
- Direct cord mobilization/massage
- Contract-relax techniques
- Usually resolves within 3 months with treatment
Therapeutic Exercise (detailed in Phase 2–3 above)
Progressive sequence:
- Pendulum → AAROM → AROM → Resisted
- Scapular stabilizers before global strength
- Closed-chain before open-chain for pain control
- Functional task integration
Electrophysical Agents
- TENS/IFC — pain management, allows participation in exercise
- LLLT (Low-Level Laser Therapy) — reduces post-mastectomy pain and improves ROM per some RCTs
- Ultrasound — scar tissue management (limited evidence, used adjunctively)
- Heat (moist heat packs) — pre-exercise muscle relaxation
- Cryotherapy — post-exercise inflammation control
B. Lymphedema Management
Complete Decongestive Therapy (CDT) — gold standard:
- Manual Lymphatic Drainage (MLD) — specialized massage redirecting lymph to functional nodes
- Multilayer compression bandaging — worn 23 hours/day in intensive phase
- Decongestive exercise — limb movement within bandaging activates muscle pump
- Skin care — prevent infection, maintain skin integrity
- Compression garments — Class II (30–40 mmHg) for maintenance phase
- Self-care education — self-MLD technique, garment management
C. Neuropathic Pain Management
- Post-mastectomy pain syndrome (PMPS) — chronic neuropathic pain in chest wall/axilla/arm
- Affects 20–50% of patients
- Management:
- Desensitization techniques (graded tactile stimulation)
- TENS over painful area
- Pharmacotherapy (gabapentin, pregabalin, amitriptyline — in coordination with oncology team)
- Mirror therapy / graded motor imagery for central sensitization
D. Winged Scapula (Serratus Anterior Palsy)
- Long thoracic nerve neuropraxia from ALND
- Conservative management is first-line (most resolve 6–24 months):
- Scapular taping to prevent winging during exercise
- Serratus anterior facilitation: wall push-ups, protraction in supine with resistance
- Thoracic brace to unload scapula if severe
- Avoid overhead loading until nerve recovery evident
- Surgical referral if no recovery by 24 months (nerve decompression, muscle transfer)
E. Postural Re-education
- Thoracic spine extension mobilization
- Cervical retraction exercises
- Chin tucks for forward head correction
- Proprioceptive neuromuscular facilitation (PNF) for trunk–shoulder coordination
- Mirror biofeedback for scapular alignment
F. Psychosocial Management
- Screen for depression/anxiety (PHQ-9, GAD-7)
- Refer for psychological support — cognitive behavioral therapy shown effective
- Body image therapy / peer support groups
- Graded exposure for kinesiophobia (fear-avoidance model)
- Fatigue management: energy conservation techniques, graded activity
G. Multidisciplinary Team (MDT) Integration
| Team Member | Role |
|---|---|
| Breast surgeon | Drain removal decisions, wound oversight |
| Oncologist | Coordinate timing around chemotherapy cycles |
| Radiation oncologist | Counsel on radiation fibrosis risk |
| Physiotherapist | Primary rehab, exercise, manual therapy |
| Occupational therapist | ADL retraining, splinting, lymphedema garments |
| Lymphedema specialist/nurse | CDT, garment fitting |
| Psychologist/social worker | Psychosocial support |
| Dietitian | Nutritional support for healing and cancer treatment |
| Prosthetics/orthotics | Breast prosthesis fitting |
SUMMARY TABLE: Phase-by-Phase Overview
| Phase | Timeframe | Key Focus | Restrictions |
|---|---|---|---|
| Phase 1 | Days 1–7 | Breathing, hand/wrist/elbow ROM, posture, education | Shoulder ROM limited to 90° while drains in situ |
| Phase 2 | Weeks 2–6 | Full shoulder ROM restoration, scar mobility, scapular kinematics | No resistance; monitor for seroma/cording |
| Phase 3 | Weeks 6–12 | Strengthening (rotator cuff, periscapular), aerobic conditioning | Lymphedema monitoring before each session |
| Phase 4 | Months 3–12+ | Return to function, long-term lymphedema management, QoL | Ongoing precautions indefinitely |
Clinical Pearl: The timing of drain removal is the critical gating event for shoulder rehab progression. Waiting for drain removal before initiating full shoulder ROM exercises reduces seroma risk without significantly compromising long-term outcomes. After drain removal, rapid progressive ROM work over the following 4–6 weeks is essential to prevent permanent restriction.
Red Flags requiring urgent referral: sudden increase in arm swelling (cellulitis/acute lymphedema), signs of brachial plexopathy, shoulder pain unresponsive to 6 weeks of physiotherapy (consider imaging to exclude axillary recurrence), or wound dehiscence/signs of infection.
This is a shared conversation. Sign in to Orris to start your own chat.