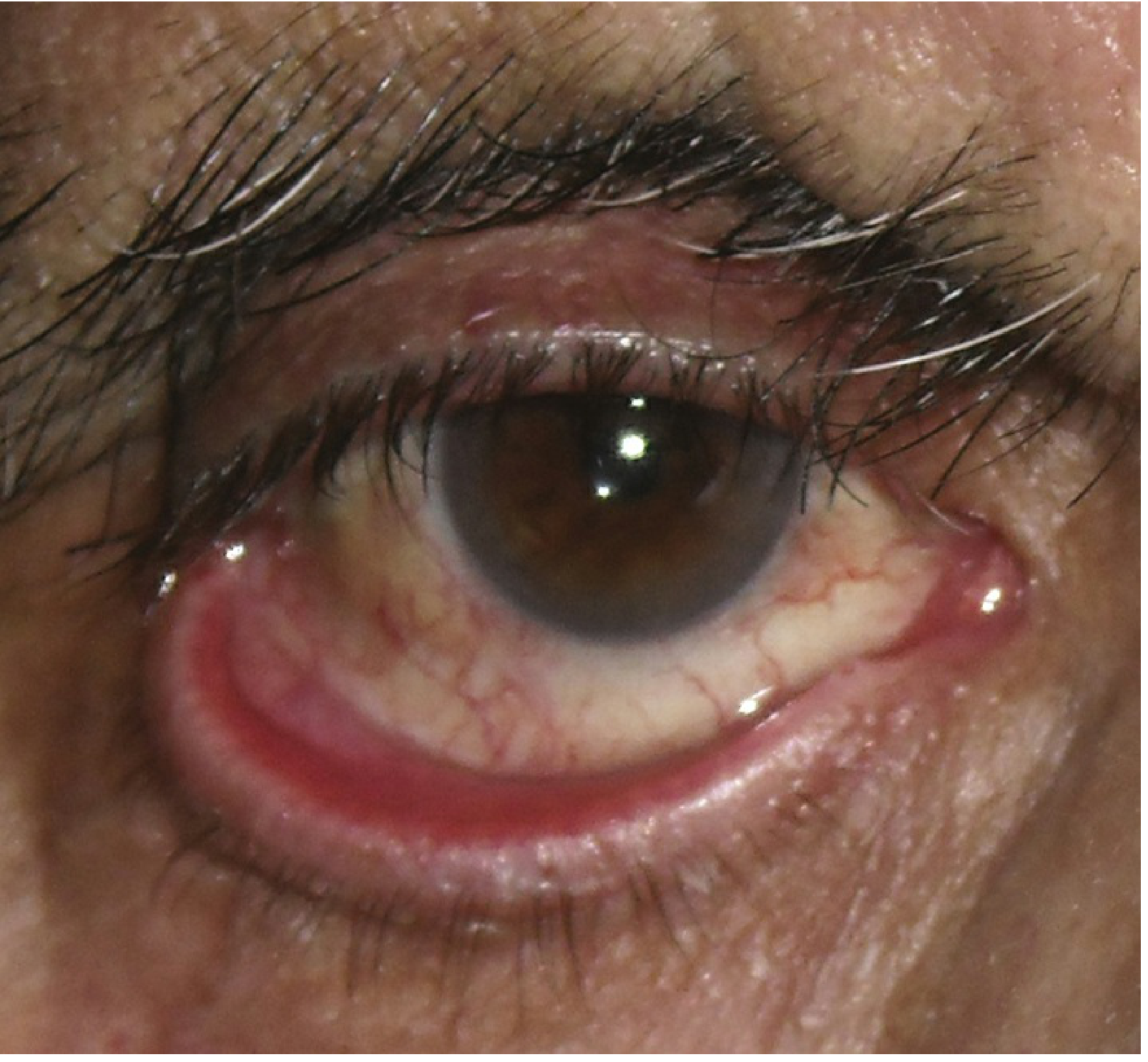
Ectropion
Reading File
Finding Sources
Searching PubMed
ectropion eyelid
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete clinical overview of ectropion, sourced from Kanski's Clinical Ophthalmology and The Wills Eye Manual.
Ectropion
Ectropion is the outward turning (eversion) of the eyelid margin away from the globe. It almost exclusively affects the lower lid.
Symptoms
- Tearing (epiphora) - most common
- Ocular irritation and redness
- Mucous discharge
- May be asymptomatic in mild cases
Types and Etiology
1. Involutional (Age-related) - MOST COMMON
Affects the lower lid of elderly individuals. Aetiological factors:
- Horizontal lid laxity: lower lid pulled >8 mm from globe, fails to snap back without blinking ("snap-back test")
- Lateral canthal tendon laxity: rounded lateral canthus, lower lid can be pulled medially >2 mm
- Medial canthal tendon laxity: pulling the lid laterally displaces the inferior punctum beyond 1-2 mm (reaches limbus if mild, reaches pupil if severe)
2. Paralytic
- Caused by ipsilateral CN VII (facial nerve) palsy
- Associated with upper and lower lid retraction, brow ptosis
- Complications: exposure keratopathy from lagophthalmos, epiphora from malpositioned punctum and failed lacrimal pump, reflex tearing from corneal irritation
3. Cicatricial
- Scarring or contracture of anterior lamella (skin and underlying tissue) pulls lid away from globe
- Causes: burn injury, prior surgery or trauma, actinic damage, chronic inflammation, skin diseases (eczema, ichthyosis)
- Clinical clue: pushing skin up over orbital margin relieves the ectropion; opening the mouth accentuates it
- Both lids may be involved
4. Mechanical
- Herniated orbital fat, eyelid tumour, or other mass effect
5. Congenital
- Associated with Down syndrome, Treacher Collins syndrome, or isolated abnormality
6. Allergic
- Contact dermatitis
Signs
| Feature | Description |
|---|---|
| Critical | Outward turning of the eyelid margin |
| Conjunctival changes | Injection, thickening, eventual keratinization (chronic exposure) |
| Corneal changes | Superficial punctate keratopathy (SPK) from exposure |
| Cicatricial cases | Eyelid scarring visible |
| Paralytic cases | Facial hemiparesis, lagophthalmos |
Workup
- History: Previous surgery, trauma, chemical burn, CN VII palsy?
- External exam:
- Orbicularis oculi function
- Horizontal lid laxity (snap-back test, distraction test)
- Punctal position
- Check for eyelid tumour, scarring, herniated fat
- If CN VII palsy + CN VIII deficit (hearing loss): CT/MRI brain to rule out acoustic neuroma
- Slit-lamp: Evaluate for exposure keratopathy and conjunctival inflammation
Treatment
Medical / Temporizing
- Lubricating drops/ointment to treat exposure keratopathy
- Warm compresses + antibiotic ointment (bacitracin or erythromycin q.i.d.) for inflamed, exposed lid margin
- Short course of antibiotic-steroid ointment (e.g., neomycin/polymyxin B/dexamethasone) if close follow-up ensured
- Lid taping as a temporizing measure
- For CN VII palsy: high-viscosity tear substitutes during day, ointment + lid taping at night; delay surgery 3-6 months as ectropion may resolve spontaneously
Surgical - by Type
| Type | Procedure |
|---|---|
| Involutional - generalized | Lateral tarsal strip (LTS): tightens lower canthal tendon by shortening and reattachment to lateral orbital rim; or tarsoconjunctival pentagon excision |
| Involutional - medial | Medial conjunctival diamond excision (medial spindle procedure), often combined with tarsal strip |
| Cicatricial - mild/localized | Excision of scar tissue + vertical skin lengthening (Z-plasty) |
| Cicatricial - severe/generalized | Transposition flaps or free skin grafts (from upper lids, posterior/pre-auricular, or supraclavicular areas) |
| Paralytic - temporary | Botulinum toxin injection into levator to induce ptosis; temporary tarsorrhaphy (especially if poor Bell phenomenon) |
| Paralytic - permanent | Medial canthoplasty (if medial canthal tendon intact); gold weight implant or lower lid tightening; permanent tarsorrhaphy if necessary |
Permanent repair for paralytic ectropion is indicated when facial nerve damage is irreversible or no improvement has occurred after 6-12 months in Bell palsy.
Follow-Up
- Patients with corneal/conjunctival exposure: follow up based on severity
- Patients using topical steroids: routine follow-up for steroid-induced IOP rise and other side effects
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 95-102; The Wills Eye Manual, pp. 384-386
This is a shared conversation. Sign in to Orris to start your own chat.