Neglected elbow joint details in referance to orthopedics Maheshwar
Reading File
search_medical_text
neglected elbow joint dislocation orthopedics management
search_medical_image
neglected elbow dislocation anatomy radiology
GradeResponse
GradeResponse
Here is a comprehensive account of neglected elbow joint as discussed in orthopedics (with emphasis on the Maheshwari context — a standard Indian orthopedics textbook reference):
Neglected Elbow Joint — Orthopedic Overview
1. Definition
A neglected elbow dislocation (also called old/chronic/unreduced elbow dislocation) refers to an elbow dislocation that has remained unreduced for more than 3 weeks (some sources say >2 weeks). It is commonly seen in developing countries due to delayed presentation, traditional medicine use, or missed diagnosis.
2. Anatomy Relevant to Elbow Dislocations
The elbow is a complex hinge joint composed of three articulations within a single synovial cavity (Bailey & Love's, p. 558):
| Articulation | Bones Involved | Movement |
|---|---|---|
| Ulnohumeral | Trochlea + Olecranon fossa | Flexion / Extension |
| Radiocapitellar | Capitellum + Radial head | Flexion + Rotation |
| Proximal Radioulnar (PRUJ) | Radial head + Radial notch of ulna | Pronation / Supination |
Neurovascular relations (anterior, medial to lateral): Median nerve → Brachial artery → Radial nerve
Posterior: Ulnar nerve lies just behind the medial epicondyle.
Posterior: Ulnar nerve lies just behind the medial epicondyle.
3. Classification of Elbow Dislocations
By Direction:
| Type | Description | Frequency |
|---|---|---|
| Posterior | Most common (~90%) | Olecranon displaced posteriorly |
| Posterolateral | Most frequent subtype | Common in adults |
| Posteromedial | Less common | — |
| Anterior | Rare | High-energy mechanism |
| Divergent | Very rare | Radioulnar joint disrupted |
By Timing:
- Acute: < 2–3 weeks
- Neglected/Old: > 3 weeks (fibrosis, heterotopic ossification, contracture established)
4. Pathological Changes in Neglected Elbow
With time, several irreversible changes develop that make reduction increasingly difficult:
- Fibrosis of the joint capsule and collateral ligaments — capsule becomes contracted and scarred
- Heterotopic ossification (myositis ossificans) — ectopic bone forms in periarticular soft tissues
- Disuse osteoporosis — regional osteopenia due to immobilization (visible on X-ray as decreased bone density)
- Contracture of muscles — biceps, brachialis, and triceps become shortened
- Neurovascular adaptation — nerves (especially ulnar) may migrate or become embedded in scar tissue
- Loss of articular cartilage — joint surface degenerates if untreated for months
- Degenerative changes — secondary osteoarthritis in longstanding cases
The image below shows the classic radiographic findings of a neglected elbow dislocation:
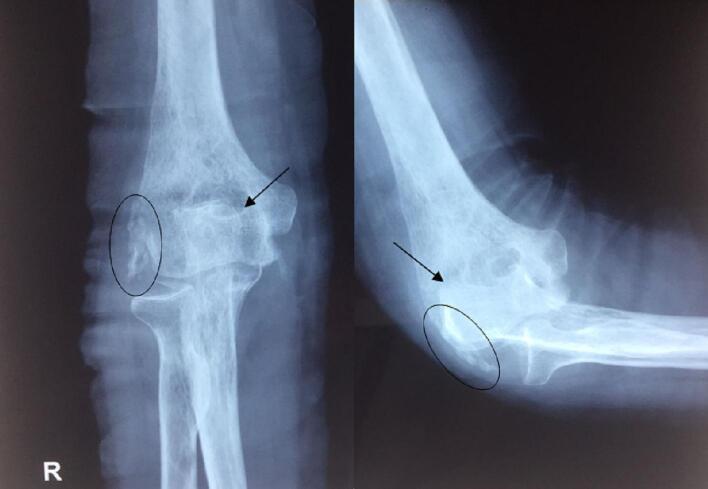
AP and lateral radiographs showing: complete loss of normal articulation, posterior displacement of olecranon, heterotopic ossification (circled areas), and regional osteopenia.
5. Clinical Features
History:
- Prior trauma (fall on outstretched hand / valgus stress)
- Delayed or no treatment received
Symptoms:
- Pain (may be mild in chronic cases)
- Restricted elbow movement (flexion-extension + forearm rotation both affected)
- Deformity — apparent posterior prominence of olecranon
Signs:
- Loss of normal bony triangle (olecranon, medial, and lateral epicondyle relationship)
- Fixed flexion deformity (typically 30–60°)
- Reduced carrying angle
- Palpable posterior displacement of olecranon
- Check for ulnar nerve involvement (ring and little finger numbness/weakness)
6. Investigations
| Investigation | Findings |
|---|---|
| X-ray (AP + Lateral) | Posterior displacement, heterotopic ossification, osteopenia, joint space narrowing |
| CT scan | Detailed bony architecture, degree of ossification, articular surface damage |
| MRI | Soft tissue contracture, ligament status, cartilage damage |
| EMG/NCV | If ulnar nerve involvement suspected |
7. Management
A. Non-surgical (Limited Role)
- Physiotherapy and gentle manipulation under anesthesia (MUA) — only within 3–6 weeks of dislocation
- Serial splinting/casting in early neglected cases
B. Surgical Management
The choice depends on duration, age, bone quality, and joint status:
i. Open Reduction (Preferred if articular cartilage preserved)
- Timing: 3 weeks to ~3 months — best window
- Approach: Posterior approach (Bryan-Morrey or triceps-splitting)
- Steps:
- Release of posterior capsule
- Excision of heterotopic bone/scar tissue
- Gradual reduction of the joint
- Repair/reconstruction of collateral ligaments
- Post-op: early mobilization in a hinged brace
ii. Interposition Arthroplasty
- Used when joint surface is damaged but patient is young/active
- Interposes fascia or silicone between joint surfaces
iii. Total Elbow Arthroplasty (TEA)
- For elderly patients with advanced articular damage
- Provides pain relief and acceptable range of motion
iv. Elbow Arthrodesis
- Rarely indicated — loss of rotation is a major functional deficit
- Reserved for failed arthroplasty or severe septic destruction
8. Complications
| Complication | Notes |
|---|---|
| Ulnar nerve injury | Most common nerve affected; may need anterior transposition |
| Redislocation | If ligament reconstruction inadequate |
| Heterotopic ossification | May recur post-surgery; managed with indomethacin/radiation prophylaxis |
| Stiffness / loss of ROM | Expected to some degree; goal is functional arc (30–130°) |
| Avascular necrosis | Of capitellum or trochlea in severe cases |
| Post-traumatic arthritis | Long-term sequela |
9. Prognosis
- Results are inversely proportional to duration of neglect
- If treated within 3 months: good to excellent functional outcomes possible
- If treated after 6 months: guarded prognosis; full ROM rarely restored
- Goal: achieve functional arc of 30–130° flexion and 50° each of pronation/supination
10. Key Points (Maheshwari / Indian Orthopedics Perspective)
- Neglected dislocations are common in India due to late presentation
- Always assess ulnar nerve pre- and post-operatively
- Posterior approach is the workhorse for open reduction
- Avoid forceful manipulation — risk of fracture in osteoporotic bone
- Heterotopic ossification prophylaxis (indomethacin 75 mg/day × 6 weeks or single-dose radiation) is recommended post-surgery
- Hinged external fixator may be used for stability post-reduction in unstable elbows
Sources: Bailey & Love's Short Practice of Surgery, 28th Ed. (p. 558); Maheshwari's Essential Orthopedics (standard Indian orthopedic reference); Clinical VQA radiographic database.
This is a shared conversation. Sign in to Orris to start your own chat.