Obesity hypoventilation syndrome full details for md exams 10 marks answer with ventilator settings
Reading File
Finding Sources
Finding Sources
Searching PubMed
"obesity hypoventilation syndrome" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive 10-mark MD exam answer. Here it is:
Obesity Hypoventilation Syndrome (OHS) - Complete 10 Mark Answer
Definition
OHS (also historically called "Pickwickian Syndrome") is defined by the triad of:
- Obesity - BMI ≥ 30 kg/m²
- Daytime hypercapnia - awake PaCO₂ ≥ 45 mmHg
- Sleep-disordered breathing - in the absence of other causes of chronic alveolar hypoventilation (e.g., COPD, neuromuscular disease, chest wall deformity, hypothyroidism, central hypoventilation)
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set
- Harrison's Principles of Internal Medicine 22E (2025)
Epidemiology
| Population | Prevalence of OHS |
|---|---|
| General adult population | 0.15 - 0.3% |
| Obese patients referred for OSA evaluation | 8 - 20% |
| Hospitalized patients with BMI ≥ 50 kg/m² | ~50% |
| Obese patients with OSA overall | 10 - 20% |
- OSA is present in 90% of OHS patients; ~70% have severe OSA (AHI >30 events/h)
- OHS often remains undiagnosed - patients have increased healthcare utilization up to 5 years before diagnosis
Pathophysiology
The pathogenesis is multifactorial. Three major interacting mechanisms operate (see diagram below):
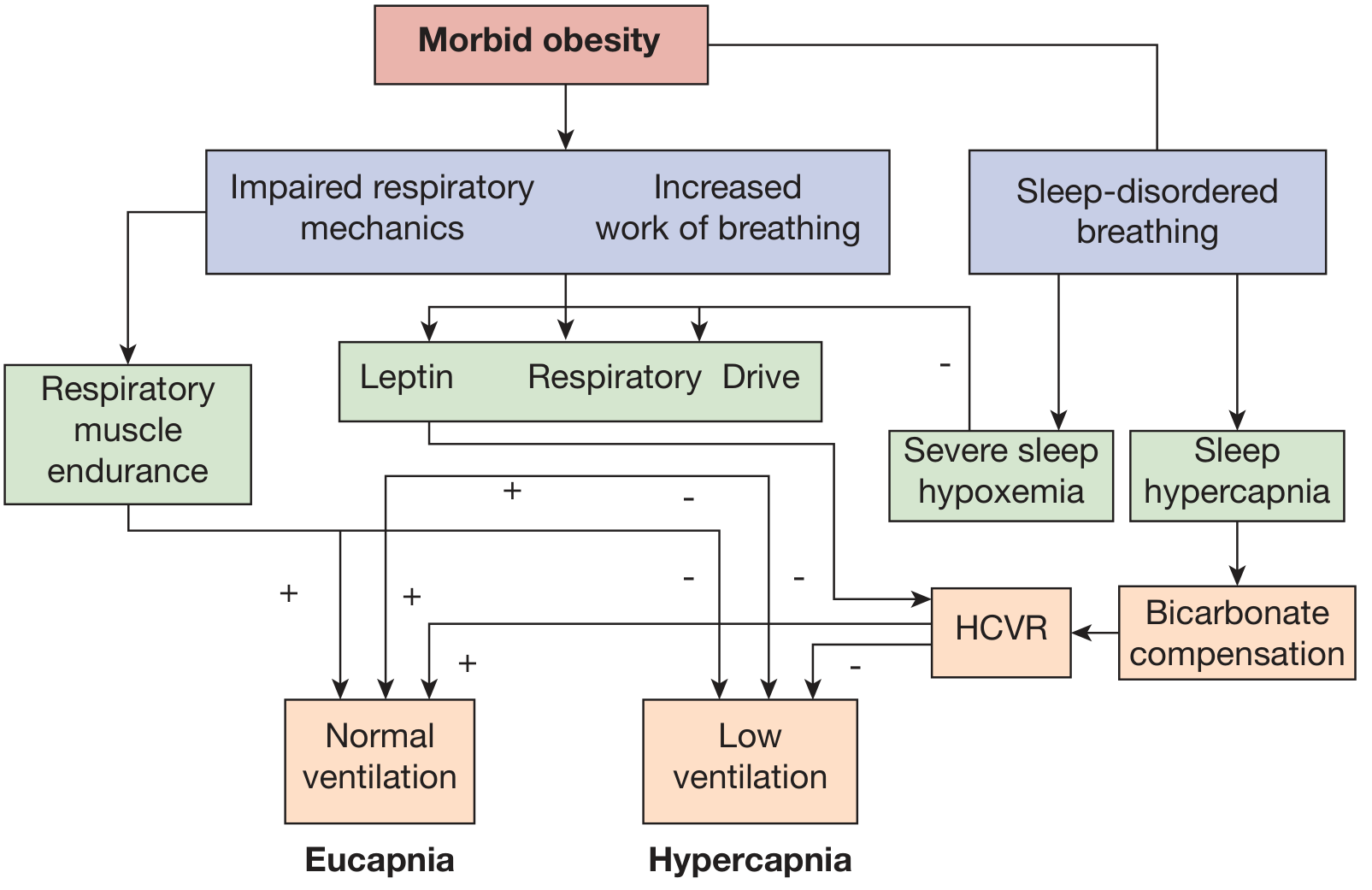
1. Abnormal Respiratory Mechanics (Mechanical Load)
- Excess adipose tissue on thorax and abdomen reduces chest wall compliance and end-expiratory lung volume
- Increases elastic and resistive work of breathing
- Cranial displacement of the diaphragm (especially supine) impairs respiratory pump efficiency
- Premature airway closure causes atelectasis, V/Q mismatch, increased A-a gradient, and hypoxemia
- CO₂ production is 2-3x normal in morbid obesity - requires doubled alveolar ventilation to maintain eucapnia
2. Sleep-Disordered Breathing
- Recurrent apneas/hypopneas cause episodic CO₂ accumulation during sleep
- Retained bicarbonate (renal compensation) blunts the hypercapnic ventilatory response (HCVR)
- Progressive CO₂ retention extends from sleep to wakefulness
- The remaining 10% of OHS patients (without OSA) show pure non-obstructive sleep hypoventilation with PaCO₂ rising >10 mmHg above wakefulness
3. Blunted Central Ventilatory Drive
- Impaired chemosensitivity to both hypercapnia and hypoxemia
- Key role of leptin resistance: leptin (produced by adipose tissue) normally stimulates ventilation via hypothalamic receptors; in OHS, central leptin resistance blunts this drive
- This blunting is likely a consequence of chronic hypoventilation rather than a primary cause - it often reverses with PAP treatment even without weight loss
- Eucapnic obese subjects show greater diaphragmatic electrical activity response to CO₂ than hypercapnic subjects
Consequences of Chronic Hypercapnia
- Polycythemia
- Pulmonary hypertension
- Cor pulmonale
- Right ventricular failure
Clinical Features
Symptoms:
- Excessive daytime somnolence (Epworth Sleepiness Scale typically elevated)
- Morning headaches (CO₂ retention)
- Dyspnea on exertion, orthopnea
- Loud snoring, witnessed apneas
- Cognitive impairment, fatigue, depression
Signs:
- Morbid obesity (BMI often >35-40 kg/m²)
- Cyanosis, plethora
- Edema (cor pulmonale)
- Loud P2, raised JVP
- Features of right heart failure
Investigations
Blood Gas and Biochemistry
| Test | Finding | Significance |
|---|---|---|
| ABG (awake) | PaCO₂ ≥ 45 mmHg, PaO₂ low | Diagnostic |
| Serum bicarbonate | ≥ 27 mEq/L | Sensitive screening test |
| Serum HCO₃ < 27 mEq/L | Dramatically decreases OHS probability | High NPV |
| Polycythemia | Hb elevated | Chronic hypoxemia |
Screening: Serum bicarbonate is the rapid screening test. A value < 27 mEq/L has high negative predictive value for OHS. If bicarbonate is elevated (≥27) or pretest probability is high - proceed to ABG.
Pulmonary Function Tests
- Reduced TLC, FRC, ERV, VC
- Reduced respiratory system compliance
- Possible mild obstructive or restrictive pattern
Sleep Study (Polysomnography)
- AHI - determines OSA severity
- Pulse oximetry - nocturnal desaturation
- End-tidal CO₂ (ETCO₂) or transcutaneous CO₂ monitoring
- Sleep-related hypoventilation: PaCO₂ (or surrogate) rises >10 mmHg during sleep to >50 mmHg for >10 minutes
Imaging
- CXR: cardiomegaly, plethoric lung fields
- ECG: RVH, RAD, P pulmonale
- Echocardiogram: pulmonary hypertension, RV dilation, LV diastolic dysfunction
Treatment
1. Weight Loss
- Substantial weight loss (20-25% of actual body weight) alone can normalize PaCO₂
- Bariatric surgery is the most effective method; difficult to achieve and sustain otherwise
- First-line long-term strategy but rarely achieves rapid reversal
2. Positive Airway Pressure (PAP) Therapy - Stepwise Algorithm
OHS Diagnosed
|
▼
Severe OSA present (AHI >30)?
|
YES → Start CPAP first (treats both OSA and hypoventilation in ~80% of OHS+OSA)
|
▼
Re-evaluate in 4-8 weeks
|
Hypercapnia persists despite good CPAP adherence?
|
YES → Upgrade to BiPAP-S (Spontaneous mode)
|
▼
Still inadequate (low minute ventilation, ongoing CO₂ elevation)?
|
YES → BiPAP-ST (Spontaneous-Timed / backup rate) or AVAPS
- If no severe OSA (low-AHI OHS): Start directly with BiPAP-ST or VAPS mode
- Acute decompensated OHS: Start BiPAP-ST or NIV immediately during hospitalization
VENTILATOR SETTINGS IN OHS (High-Yield for MD Exams)
A. CPAP (Continuous Positive Airway Pressure)
- Indication: OHS with severe OSA (AHI >30/hr) as first-line therapy
- Starting pressure: Typically 8-15 cmH₂O, titrated by PSG or auto-titration
- Goal: Eliminate obstructive events, allow CO₂ to normalize
- Success: Eliminates both OSA and OHS in ~80% of patients with predominant obstructive etiology
- Failure criteria: Persistent hypercapnia (PaCO₂ still elevated or serum HCO₃ not normalizing after 4-8 weeks of adherent CPAP use)
B. BiPAP-S (Bilevel PAP - Spontaneous Mode)
- Indication: Failed CPAP (obstructive events persist or maximum CPAP pressure 20 cmH₂O reached); poor CPAP tolerance
- Settings:
- IPAP: 12-20 cmH₂O (higher than EPAP by at least 4-6 cmH₂O to generate adequate pressure support/tidal volume)
- EPAP: 4-10 cmH₂O (titrated to abolish obstructive events and PEEP effect)
- No backup rate in spontaneous mode
- Note: Only suitable when respiratory drive is adequate
C. BiPAP-ST (Bilevel PAP - Spontaneous/Timed Mode) - Most Important for OHS
- Indication:
- OHS without severe OSA
- Failed BiPAP-S (reduced minute ventilation)
- Acute decompensated OHS
- Hypercapnia persisting despite CPAP adherence
- Settings:
| Parameter | Recommended Setting |
|---|---|
| IPAP | 14-25 cmH₂O (titrate to normalize PaCO₂ and achieve adequate tidal volume) |
| EPAP | 4-10 cmH₂O (higher EPAP for higher AHI/greater obstruction) |
| Backup Rate (BUR) | 2 breaths/min below patient's spontaneous rate, or set to auto-rate; typically 10-14 breaths/min |
| Inspiratory Time (Ti) | Prolonged (increase to favor larger tidal volumes) |
| Rise Time | Increased to improve ventilation and gas exchange |
| Cycle Sensitivity | Lowered to prolong inspiratory time |
| Target Tidal Volume | Not preset in S/T mode (driven by pressure) |
- Key principle: Strategies that increase inhalation time (longer rise time, longer Ti, lower cycle sensitivity) favor larger tidal volumes and improved gas exchange
- The backup rate ensures ventilation during periods of reduced or absent spontaneous effort
D. AVAPS / VAPS (Average Volume-Assured Pressure Support)
- Mode: Hybrid adaptive algorithm - automatically adjusts IPAP/PS between a minimum and maximum to achieve a preset target tidal volume or minute ventilation
- Devices: AVAPS (Philips); iVAPS (ResMed)
- Target tidal volume: 8-10 mL/kg ideal body weight (NOT actual body weight - critical point for OHS)
- Use ideal body weight to avoid over-ventilation
- Settings:
| Parameter | Setting |
|---|---|
| IPAP min | 14 cmH₂O (starting point) |
| IPAP max | 25-30 cmH₂O |
| EPAP | 4-10 cmH₂O (as per obstruction) |
| Target Vt | 8-10 mL/kg ideal body weight |
| Backup Rate | 10-14 breaths/min |
| AVAPS AE | Adds autotitrating EPAP - useful in OHS with significant OSA component |
- Advantage: Automatically compensates for fluctuating respiratory mechanics (e.g., REM sleep, positional changes, disease progression), prevents hypoventilation from leaks
- Caveats: Overestimation of exhaled Vt due to mask leak can cause algorithm-induced hypoventilation; higher cost; not superior to BiPAP-ST in most RCTs (minimal additional PaCO₂ reduction of ~2 mmHg); may impair subjective sleep quality
E. Summary of Mode Selection
| Clinical Scenario | Recommended Mode |
|---|---|
| OHS + severe OSA (AHI >30) | CPAP first |
| CPAP failure, good drive | BiPAP-S |
| Reduced drive, low MV, no severe OSA | BiPAP-ST |
| Acute decompensated OHS | BiPAP-ST (or invasive if failing NIV) |
| OHS with pulmonary HTN | BiPAP-ST (NIV improves cardiac function) |
| Malignant OHS (BMI >40 + ICU + multiorgan dysfunction) | BiPAP-ST; consider tracheostomy |
| Fluctuating mechanics, need for auto-titration | AVAPS/iVAPS |
Supplemental Oxygen
- Used adjunctively when hypoxemia persists despite adequate PAP therapy
- Avoid oxygen alone without PAP - it can worsen hypercapnia by blunting hypoxic drive
- Added as supplemental O₂ bled into circuit when SpO₂ targets not met on NIV alone
Monitoring Response to Treatment
- Serum bicarbonate normalization - within weeks of effective PAP
- ABG normalization (PaCO₂ to <45 mmHg)
- Epworth Sleepiness Scale improvement
- Polysomnography with CO₂ monitoring: formal PSG and ventilator titration recommended within 3 months of discharge (ATS recommendation)
- Surrogate CO₂ monitoring: ETCO₂ or transcutaneous CO₂ (PtcCO₂) used during titration night
Prognosis and Mortality
- 2-year all-cause mortality in hospitalized OHS patients: ~23% (vs. 9% in simple obesity)
- 1-year mortality after acute-on-chronic hypercapnic respiratory failure in OHS: ~18%
- Untreated OHS is associated with significantly higher mortality than BMI-matched OSA
- Effective PAP therapy and weight loss improve cardiovascular outcomes and survival
- Recent meta-analysis (PMID: 40605318, 2025) confirms PAP therapy reduces pulmonary artery pressure in OHS with pulmonary hypertension
Key Exam Points to Remember
- Diagnostic triad: BMI ≥30 + PaCO₂ >45 + sleep-disordered breathing (after excluding other causes)
- Screening: Serum HCO₃ < 27 virtually excludes OHS; ≥27 needs ABG confirmation
- 90% have OSA; CPAP resolves OHS in 80% of these - try CPAP first
- AVAPS target Vt = 8-10 mL/kg IDEAL body weight (not actual)
- Backup rate in BiPAP-ST = ~2 breaths below spontaneous rate (typically 10-14/min)
- Leptin resistance is the key endocrine mechanism of blunted drive
- Never give O₂ alone - it worsens hypercapnia by removing hypoxic drive
- Acute decompensated OHS: start NIV in hospital and continue at discharge
- Formal PSG + ventilator titration within 3 months of hospital discharge (ATS guideline)
- Weight loss of 20-25% normalizes PaCO₂ - bariatric surgery is most reliable method
Sources: Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders, 2-Volume Set; Harrison's Principles of Internal Medicine 22E (2025); Miller's Anesthesia 10e; Recent evidence: Sarvananda et al. 2025, PMID 40605318 (systematic review - PAP on pulmonary artery pressure in OHS); Pépin JL et al. 2025, PMID 40203613 (narrative review - OHS current status)
This is a shared conversation. Sign in to Orris to start your own chat.