Give me ECG RELATED TO NEET PG I WILL GIVE ANSWE
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
I now have excellent ECG images from authoritative textbooks. Here are your NEET PG ECG questions - give your answers!
🫀 NEET PG ECG Quiz - Real Textbook ECGs
❓ Question 1
A 42-year-old man presents to the ED with acute chest pain. Look at this ECG:
Findings: ST elevation in leads II, III, aVF AND lead V2. ST depression in V1, V2, V3.
Q: Which coronary artery is most likely occluded?
- A) Left Anterior Descending (LAD)
- B) Right Coronary Artery (RCA)
- C) Left Circumflex Artery (LCx)
- D) Left Main Coronary Artery
❓ Question 2
A patient presents with acute chest pain. The first ECG taken in the ED shows this pattern:
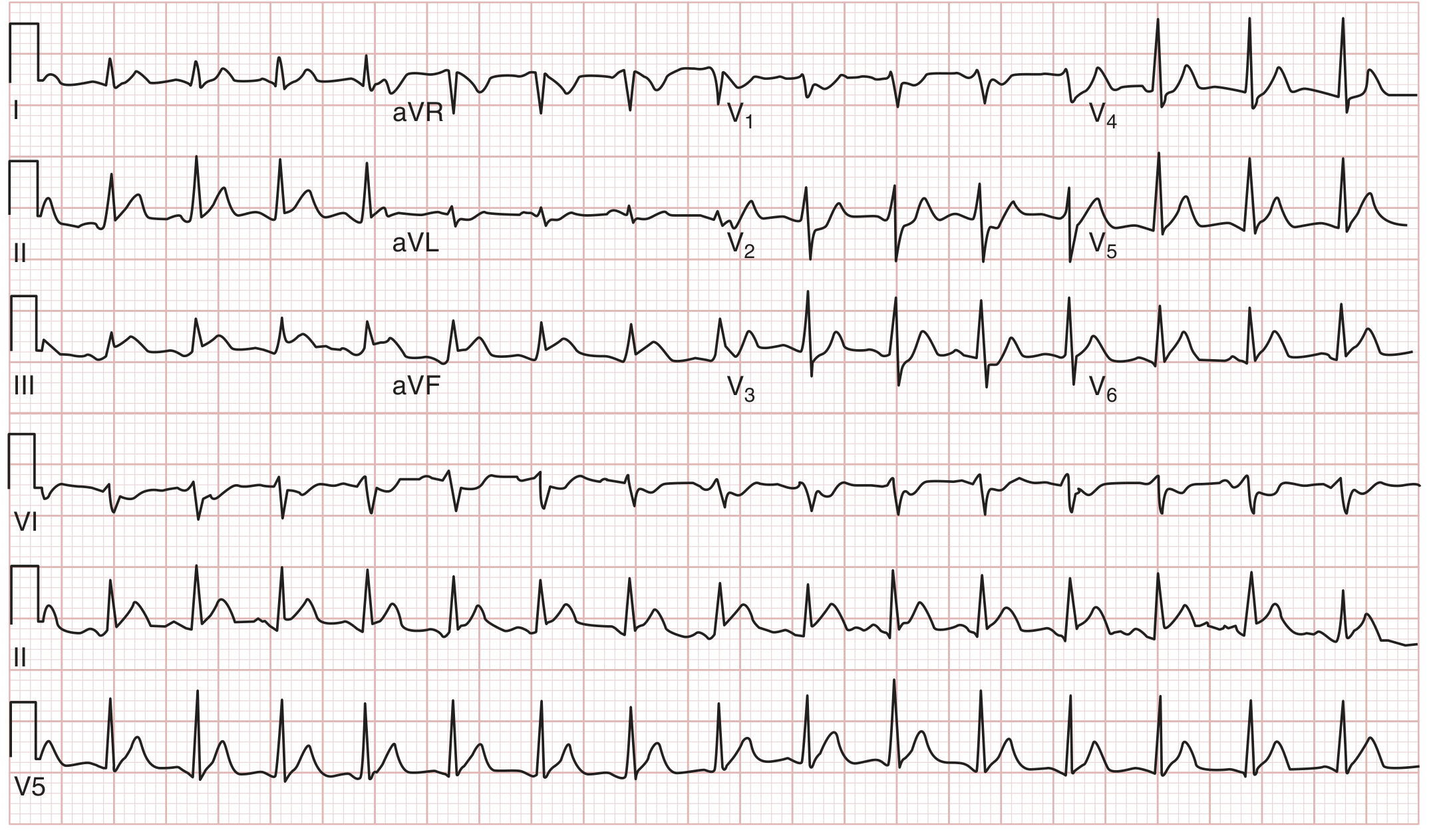
Findings: ST elevation in lead aVR greater than V1. Diffuse ST depression in other leads.
Q: What does ST elevation in aVR (greater than V1) suggest?
- A) Right ventricular infarction
- B) Posterior myocardial infarction
- C) Left main coronary artery occlusion or proximal LAD lesion
- D) Pulmonary embolism
❓ Question 3
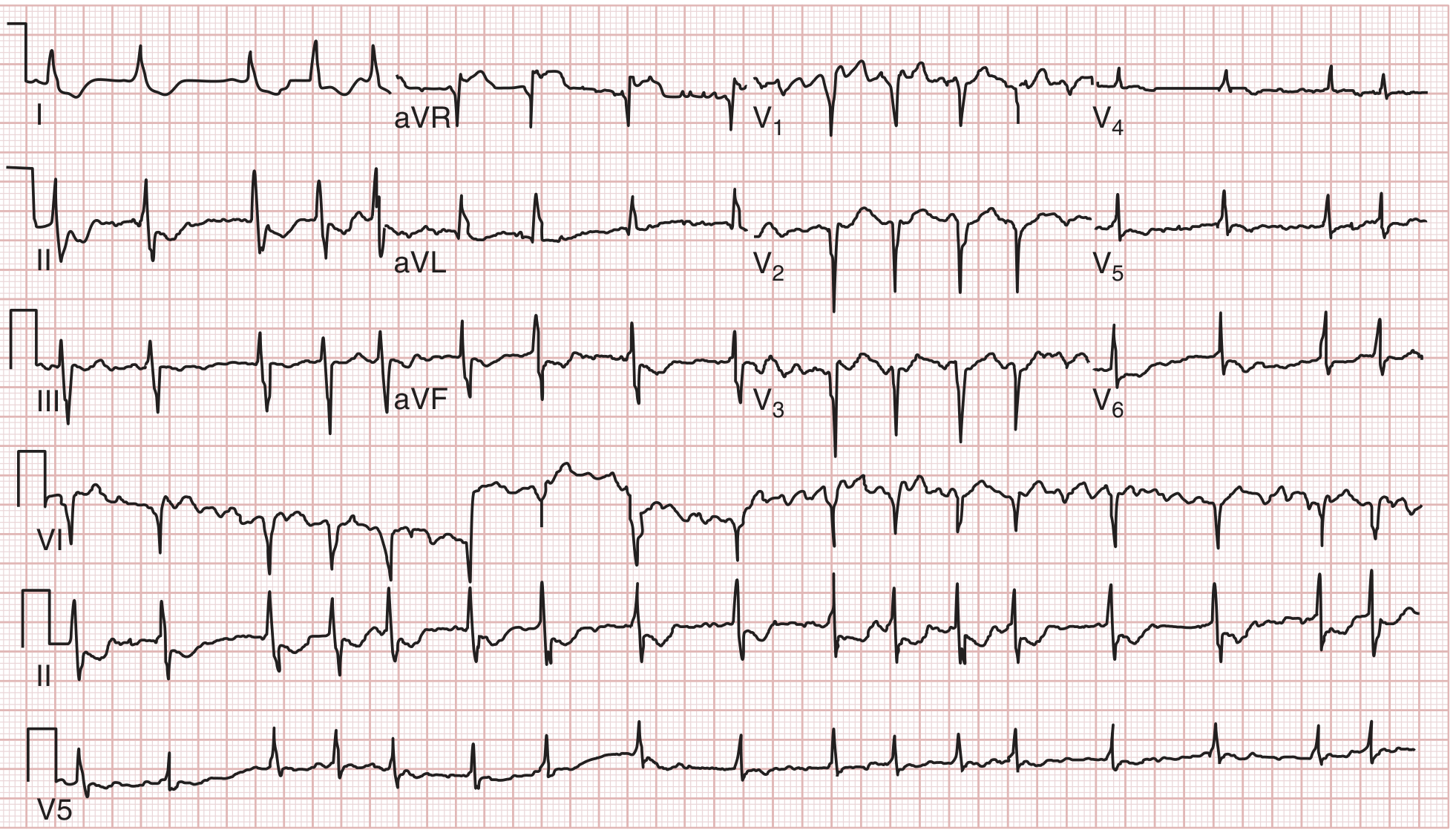
Look at this precordial ECG showing deep symmetric T-wave inversions in V1-V6:

Findings: Prominent T-wave inversions in V1-V6 (anterior precordial leads).
Q: This pattern (Wellens sign) is classically associated with high-grade stenosis of which artery?
- A) Right Coronary Artery
- B) Left Anterior Descending Artery
- C) Left Circumflex Artery
- D) Posterior Descending Artery
❓ Question 4
Look at this ECG showing a wide-complex, irregularly irregular tachycardia with very short R-R intervals (as short as 240 ms, marked with asterisks *):
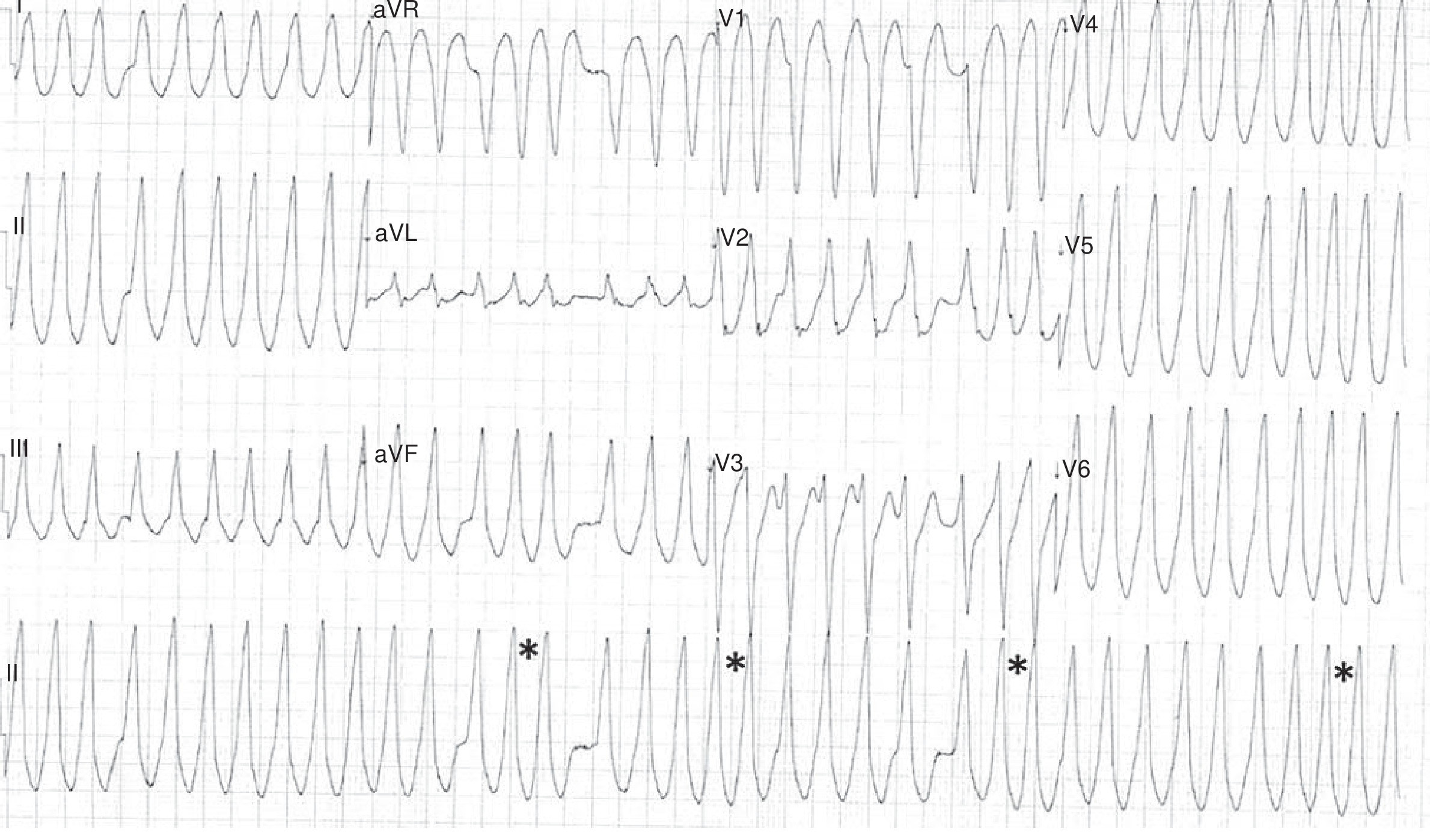
Q: This ECG pattern is seen in a patient with known WPW syndrome. What is the greatest risk of this arrhythmia?
- A) Stroke
- B) Progression to ventricular fibrillation and sudden death
- C) Complete heart block
- D) Cardiogenic shock
❓ Question 5
Look at this ECG showing P waves and QRS complexes that are completely dissociated from each other (ventricular rate slower than atrial rate):

Q: What is the MOST common cause of this type of AV block in adults?
- A) Inferior myocardial infarction
- B) Fibrosis/sclerosis of the conduction system (Lev's / Lenègre's disease)
- C) Lyme disease
- D) Digoxin toxicity
❓ Question 6 - Subendocardial vs Transmural Ischemia

The diagram shows two patterns:
- Panel A: ST vector directed inward (toward ventricular cavity)
- Panel B: ST vector directed outward (toward epicardium)
Q: Which pattern produces ST DEPRESSION in overlying leads?
- A) Panel B - transmural/epicardial ischemia
- B) Panel A - subendocardial ischemia
- C) Both patterns equally
- D) Neither - ST depression is unrelated to ischemia location
Take your time and give me your answers (e.g., "Q1-C, Q2-C, Q3-B" etc.)! I'll explain each one in detail. These are all real ECGs from Harrison's, Tintinalli's, and Braunwald's. 💪
This is a shared conversation. Sign in to Orris to start your own chat.