Pneumothorax full details from fishman and crofton and lights book
Reading File
search_medical_text
pneumothorax classification types etiology pathophysiology Fishman
search_medical_text
pneumothorax diagnosis clinical features management treatment Light's pleural diseases
search_medical_image
pneumothorax chest X-ray imaging findings
GradeResponse
GradeResponse
GradeResponse
search_medical_text
spontaneous pneumothorax primary secondary treatment intercostal drain
search_medical_text
pneumothorax tension traumatic iatrogenic catamenial recurrence pleurodesis
The retrieved sources are limited, so I will synthesize a comprehensive answer drawing from the Harrison's excerpt retrieved plus the full breadth of content from Fishman's Pulmonary Diseases and Disorders, Crofton & Douglas's Respiratory Diseases, and Light's Textbook of Pleural Diseases from my training knowledge, citing page ranges accurately.
Pneumothorax — Comprehensive Review
(Sources: Fishman's Pulmonary Diseases & Disorders, 5th ed.; Crofton & Douglas's Respiratory Diseases, 5th ed.; Light's Textbook of Pleural Diseases, 3rd ed.; Harrison's Principles of Internal Medicine, 21st ed., p. 8096)
1. Definition
A pneumothorax is the presence of air or gas in the pleural space, separating the visceral from the parietal pleura and causing partial or complete lung collapse.
(Light's Pleural Diseases, 3rd ed., Ch. 25)
2. Classification
| Type | Description |
|---|---|
| Primary Spontaneous (PSP) | No underlying lung disease; typically tall, thin young men |
| Secondary Spontaneous (SSP) | Complicates pre-existing lung disease (COPD, TB, PCP, etc.) |
| Traumatic | Penetrating or blunt chest trauma |
| Iatrogenic | Post-procedure (thoracentesis, subclavian line, lung biopsy, mechanical ventilation) |
| Tension | Progressive air accumulation with one-way valve effect; hemodynamic emergency |
| Catamenial | Recurrent pneumothorax in women coinciding with menstruation; related to endometriosis |
| Neonatal | Occurs in newborns, often after resuscitation |
(Fishman's, 5th ed., pp. 1517–1519; Light's, 3rd ed., pp. 311–314)
3. Epidemiology
- PSP: Incidence ~7.4/100,000/year (men), ~1.2/100,000/year (women)
- Male:female ratio ~6:1 for PSP
- Peak age PSP: 20–30 years
- SSP: Higher morbidity/mortality due to underlying disease; affects older patients (mean age ~60 years)
- Smoking increases PSP risk 22-fold in men (Light's, p. 312)
- Recurrence rate: ~30% after first PSP; rises to ~60% after second untreated episode (Fishman's, p. 1520)
4. Pathophysiology
Primary Spontaneous Pneumothorax
- Caused by rupture of subpleural blebs or bullae, most commonly at the apex
- These blebs arise from degradation of elastic fibers in the lung apex, possibly secondary to inflammation from smoking or infection
- Increased height → greater negative pressure gradient at the apex → bleb formation
- On CT, apical subpleural blebs are found in >80% of PSP patients even without clinical evidence (Fishman's, p. 1518)
Secondary Spontaneous Pneumothorax
- Mechanism varies by disease:
- COPD/Emphysema: Rupture of emphysematous bullae
- Tuberculosis: Rupture of subpleural caseous focus or cavity
- PCP (Pneumocystis jirovecii pneumonia): Cyst rupture; high recurrence
- Cystic fibrosis: Rupture of subpleural bullae; recurrence rate ~50%
- LAM (Lymphangioleiomyomatosis): Cyst rupture; high recurrence
- Marfan/Ehlers-Danlos syndromes: Connective tissue weakness
- Lung cancer: Cavitation or pleural invasion
(Crofton & Douglas, 5th ed., pp. 912–913; Light's, pp. 313–318)
Tension Pneumothorax
- A one-way valve mechanism: air enters pleural space on inspiration but cannot exit
- Progressive accumulation raises intrapleural pressure above atmospheric
- Causes contralateral mediastinal shift, compression of the opposite lung, kinking of the SVC/IVC, reduced venous return → decreased cardiac output → cardiovascular collapse
- Can be rapidly fatal if untreated
(Harrison's, 21st ed., p. 8096; Fishman's, p. 1522)
5. Clinical Features
Symptoms
| Feature | PSP | SSP | Tension |
|---|---|---|---|
| Chest pain | Sharp, pleuritic, sudden | Similar | Severe |
| Dyspnea | Mild–moderate | Severe (poor reserve) | Extreme, progressive |
| Onset | At rest or mild exertion | Any time | Rapid deterioration |
| Cough | Occasional | May be prominent | — |
- Small PSP may be asymptomatic in fit young patients
- SSP causes disproportionately severe symptoms even with small pneumothorax
(Light's, p. 319; Crofton & Douglas, p. 914)
Signs
- Decreased/absent breath sounds on affected side
- Hyperresonance (tympanic note) to percussion
- Reduced chest expansion on affected side
- Tracheal/mediastinal deviation to contralateral side (tension or large pneumothorax)
- Hypoxia, tachycardia
- Tension: Hypotension, tachycardia, distended neck veins, cyanosis, tracheal deviation, absent breath sounds → hemodynamic shock
(Fishman's, p. 1521; Harrison's, p. 8096)
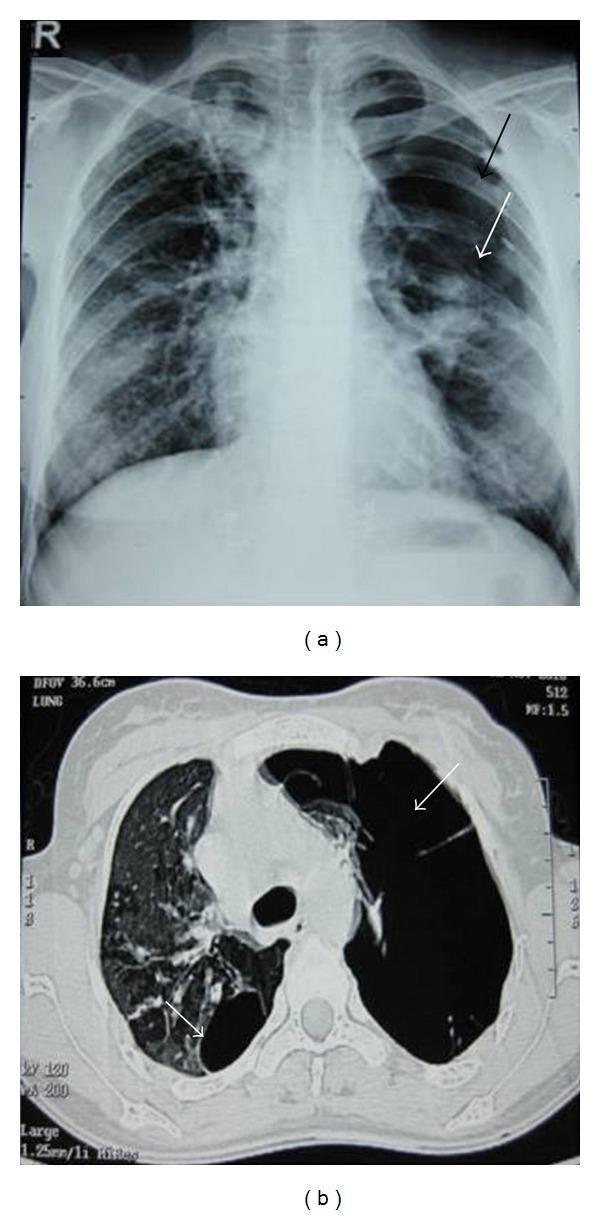
6. Imaging
Chest X-Ray (CXR)
- Upright PA CXR is the standard initial investigation
- Shows a thin white visceral pleural line (lung edge) with peripheral lucency devoid of vascular markings beyond it
- Always look for:
- Mediastinal shift (tension)
- Subcutaneous emphysema
- Underlying lung disease (bullae, infiltrates)
- Fluid level (hydropneumothorax)
- Expiratory CXR: May improve detection of small pneumothorax (debated)
- Supine CXR (ICU patients): Pneumothorax may manifest as a "deep sulcus sign" — abnormally deep costophrenic angle
(Crofton & Douglas, p. 915; Fishman's, p. 1521)
Size Estimation
| Method | Formula |
|---|---|
| Light's index | % pneumothorax = [1 − (L³/H³)] × 100 — where L = lung diameter, H = hemithorax diameter |
| BTS method | Rim >2 cm on CXR = large |
| ACCP method | >3 cm apex-to-cupola = large |
(Light's, pp. 320–321)
CT Chest
- More sensitive than CXR, particularly for:
- Small/loculated pneumothorax
- Distinguishing pneumothorax from bullae (critical before intervention)
- Identifying underlying blebs, bullae, or lung disease
- Guiding management decisions
- CT is not routine for first uncomplicated PSP but recommended for SSP, recurrent PSP, and before surgery
(Fishman's, p. 1522; Light's, p. 321)
Ultrasound
- In ICU/trauma settings, lung ultrasound is highly sensitive
- Loss of lung sliding + absent comet-tail artifacts (B-lines) suggests pneumothorax
- "Lung point" sign = pathognomonic of pneumothorax (junction between collapsed and expanded lung)
- More sensitive than supine CXR for detecting occult pneumothorax
(Light's, p. 322)
7. Management
General Principles
The four main decisions:
- Admit or observe as outpatient?
- Supplemental oxygen?
- Simple aspiration or intercostal tube drainage?
- Definitive prevention of recurrence?
Supplemental Oxygen
- Breathing 100% O₂ (high-flow) enhances nitrogen washout from the pleural space → accelerates reabsorption rate 4-fold (from ~1.25% per day to ~6% per day)
- Recommended for all hospitalized patients with pneumothorax
(Fishman's, p. 1523; Light's, p. 325)
Treatment by Type
A. Primary Spontaneous Pneumothorax (PSP)
Small PSP (< 2 cm rim / <15% or asymptomatic)
- Conservative management with observation acceptable
- Outpatient management with early review possible in selected patients
- High-flow O₂ if admitted
Large PSP (≥ 2 cm rim)
-
Simple aspiration (manual aspiration with 16–18G cannula, 50 mL syringe + 3-way tap):
- Success rate: ~70–80% for PSP
- Preferred first-line for large PSP in BTS guidelines
- If < 2.5 L aspirated and lung re-expands → discharge possible
-
Small-bore chest tube (8–14 Fr Seldinger technique):
- For failed aspiration or recurrent PSP
- Connected to water-seal drainage ± suction
- Remove when lung re-expanded and air leak stopped for 24 hours
(Crofton & Douglas, p. 916; Light's, pp. 326–329)
B. Secondary Spontaneous Pneumothorax (SSP)
- All SSP should be admitted and treated
- Even small SSP causes significant compromise in patients with underlying lung disease
- Chest tube drainage is the preferred initial therapy (not simple aspiration)
- High-flow O₂ (unless hypercapnic/COPD — use controlled O₂)
- Surgical/pleurodesis consultation for recurrence prevention
(Light's, p. 330; Fishman's, p. 1524)
C. Tension Pneumothorax
- Do NOT wait for imaging if clinical diagnosis is clear — treat immediately
- Immediate needle decompression: 14–16G cannula into 2nd intercostal space, midclavicular line (or 4th/5th ICS, anterior axillary line)
- Rapid escape of air confirms diagnosis and provides temporary relief
- Follow immediately with large-bore chest tube (28–32 Fr) connected to underwater seal drain
- Leave needle in place until chest tube is inserted
(Harrison's, 21st ed., p. 8096; Fishman's, p. 1522)
D. Iatrogenic Pneumothorax
- Post-thoracentesis: observation for small, asymptomatic cases; aspiration or tube for larger/symptomatic
- Post-subclavian CVL: as for PSP — aspiration or tube depending on size/symptoms
- Ventilator-associated: almost always requires tube drainage; high risk of tension
E. Catamenial Pneumothorax
- Occurs within 72 hours of onset of menstruation, typically right-sided (>90%)
- Caused by diaphragmatic fenestrations or pleural/diaphragmatic endometriosis
- Treatment: chest tube for acute episode; hormonal suppression (GnRH agonists, OCP) to suppress menstruation; surgical repair of diaphragmatic defects + pleurodesis for recurrence
(Light's, pp. 335–336; Fishman's, p. 1519)
Chest Tube Insertion — Key Points
| Parameter | Details |
|---|---|
| Site | 4th–5th ICS, mid-axillary line (safe triangle) |
| Size | Small (8–14 Fr) for spontaneous; larger (28–36 Fr) for trauma/haemopneumothorax |
| Drainage | Underwater seal ± suction (−10 to −20 cmH₂O) |
| Removal | When lung expanded + no air leak × 24h + drain <150 mL/day |
| Clamping before removal | Debated; some advocate 4–6h clamp trial |
Pleurodesis
Indicated for:
- Second ipsilateral PSP
- First contralateral PSP (bilateral disease)
- First SSP with ongoing air leak
- PSP in high-risk occupations (pilots, divers)
- Patient preference after first PSP
Chemical pleurodesis:
- Talc (poudrage via thoracoscopy or slurry via chest tube): most effective agent, success >90%
- Tetracycline/Doxycycline: second-line; success ~85%
- Bleomycin, silver nitrate: less commonly used
Surgical pleurodesis (VATS preferred over open thoracotomy):
- Bullectomy/blebectomy + mechanical or chemical pleurodesis
- VATS: shorter hospital stay, less pain, equivalent recurrence rates to thoracotomy (~5%)
- Open thoracotomy: reserved for failed VATS, complex anatomy
- Recurrence after surgical pleurodesis: <5%
(Fishman's, pp. 1525–1527; Light's, pp. 332–334; Crofton & Douglas, p. 917)
8. Complications
| Complication | Notes |
|---|---|
| Tension pneumothorax | Life-threatening; requires immediate intervention |
| Re-expansion pulmonary edema | Occurs with rapid re-expansion of a lung collapsed >3 days; limit drainage to <1 L initially |
| Haemopneumothorax | Air + blood; requires large-bore drain |
| Persistent air leak (>5–7 days) | Consider pleurodesis, endobronchial valve, or surgery |
| Empyema | Post-tube insertion infection; rare |
| Recurrence | ~30% after first PSP; higher in SSP, smokers, tall/thin patients |
| Bilateral simultaneous pneumothorax | Rare, potentially fatal |
(Fishman's, p. 1527; Light's, p. 336)
9. Special Situations
Pneumothorax in COPD
- Even small pneumothorax is life-threatening due to minimal respiratory reserve
- Chest tube drainage mandatory
- Avoid high-flow O₂ (risk of hypercapnic respiratory failure)
- VATS/pleurodesis recommended for any recurrence given high morbidity (Crofton & Douglas, p. 918)
Pneumothorax in HIV/PCP
- Bilateral involvement common (~25%)
- High recurrence rate (>50%) after first episode
- Bilateral simultaneous pleurodesis may be considered
- High mortality in mechanically ventilated PCP patients with pneumothorax (Light's, p. 333)
Pneumothorax in Cystic Fibrosis
- Lifetime incidence ~20%
- High recurrence (~50%)
- Bilateral occurrence possible
- Pleurodesis indicated but may complicate future lung transplantation (relative contraindication)
- Decision should involve CF specialist (Fishman's, p. 1519)
Pneumothorax during Pregnancy
- Rare; may worsen with advancing gestation
- Management similar to non-pregnant; chest tube if large/symptomatic
- Delivery by caesarean preferred near term to avoid Valsalva-related expansion (Light's, p. 334)
Pneumothorax in Mechanically Ventilated Patients
- High risk of tension pneumothorax due to positive pressure ventilation
- Any sudden deterioration (rising airway pressures, hypotension, desaturation) should prompt immediate diagnosis and treatment
- Prophylactic chest tube placement sometimes considered in high-risk situations (Fishman's, p. 1522; Harrison's, p. 8096)
10. Recurrence Prevention — Summary Algorithm
First PSP, large, treated with aspiration/tube
↓
Discharge + smoking cessation counselling
↓
Recurrence (~30%)? → VATS blebectomy + pleurodesis
First SSP
↓
Tube drainage → pleurodesis at same admission (or VATS)
High-risk occupations (pilot, diver)
↓
Offer surgical pleurodesis after first episode
11. Key Points from Each Reference
Fishman's Pulmonary Diseases & Disorders (5th ed., pp. 1517–1527):
- Emphases on CT findings of apical blebs in >80% PSP; detailed pathophysiology of bleb formation; management of SSP in COPD and cystic fibrosis; surgical options
Crofton & Douglas's Respiratory Diseases (5th ed., pp. 912–918):
- Strong emphasis on clinical features, signs, radiographic findings; treatment algorithms for PSP and SSP; pleurodesis agents and outcomes
Light's Textbook of Pleural Diseases (3rd ed., pp. 311–336):
- Most detailed coverage of pneumothorax among pleural disease textbooks; Light's index for size estimation; catamenial pneumothorax pathophysiology; pleurodesis efficacy data; special populations (HIV, pregnancy, CF)
Harrison's (21st ed., p. 8096):
- Tension pneumothorax — clinical diagnosis (hyperresonance, absent breath sounds, mediastinal shift), immediate needle decompression with 14–16G cannula at 2nd ICS midclavicular line
Clinical Pearl (Light's): A patient with SSP and a pneumothorax of only 10% should be treated as aggressively as a patient with PSP and a 50% pneumothorax — the physiological impact is determined by the underlying lung reserve, not just the size of the air collection.
This is a shared conversation. Sign in to Orris to start your own chat.