Incompetent lower oesophageal sphincter with grade II reflux oesophagitis in the lower end. Resolving, acute erosive gastritis noted in the distal stomach and antrum. The fundus and proximal body appear normal. Samples were collected for H.pylori presence. To await report. Oedematous and congested pylorus. There are multiple small erosions seen on the anterior and inferior walls of the duodenal bulb. No cicatrisation. The rest of the duodenum is normal. H pylori positive ( mild )
gastro-oesophageal reflux disease grade II oesophagitis lower oesophageal sphincter management
H pylori positive erosive gastritis duodenal erosions treatment eradication
H pylori eradication triple therapy first line treatment peptic ulcer disease
reflux oesophagitis proton pump inhibitor treatment GERD lifestyle modification
Upper GI Endoscopy — Findings Summary & Clinical Interpretation
1. Incompetent Lower Oesophageal Sphincter (LOS) + Grade II Reflux Oesophagitis
| LA Grade | Description |
|---|---|
| A | Mucosal breaks ≤5 mm |
| B (Grade II) | Mucosal breaks >5 mm, not confluent between fold tops |
| C | Confluent breaks <75% circumference |
| D | Mucosal break ≥75% circumference |
- Proton pump inhibitor (PPI) — e.g., Omeprazole 20–40 mg or Pantoprazole 40 mg once daily before meals, for 8 weeks initially
- Lifestyle measures: Head-of-bed elevation, avoid late meals, reduce caffeine/alcohol/fatty foods, weight loss if overweight
- Repeat endoscopy after 8–12 weeks of therapy to confirm healing
- Long-term maintenance PPI if symptoms recur on stopping
2. Resolving Acute Erosive Gastritis — Distal Stomach & Antrum
- H. pylori infection (confirmed here — see below)
- NSAIDs / aspirin
- Alcohol
- Stress (critical illness)
3. H. pylori Positive (Mild)
| Drug | Dose | Frequency |
|---|---|---|
| PPI (e.g., Omeprazole) | 20–40 mg | Twice daily |
| Amoxicillin | 1 g | Twice daily |
| Clarithromycin | 500 mg | Twice daily |
Where clarithromycin resistance is high (>15–20% locally), Bismuth quadruple therapy is preferred: PPI + Bismuth subsalicylate + Metronidazole + Tetracycline × 10–14 days.
4. Oedematous and Congested Pylorus
5. Multiple Small Erosions — Anterior & Inferior Walls of Duodenal Bulb
Integrated Management Plan
- Initiate H. pylori eradication (14-day triple or quadruple therapy as above) — this addresses the gastritis, pyloric congestion, and duodenal erosions simultaneously
- Continue PPI throughout and for 4–8 weeks post-eradication to heal oesophagitis and duodenal erosions
- Confirm eradication at 4–6 weeks post-therapy (urea breath test preferred)
- Lifestyle modification for GERD
- Avoid NSAIDs, aspirin, steroids, and alcohol during healing phase
- Follow-up endoscopy at 8–12 weeks to reassess Grade II oesophagitis healing and confirm duodenal erosion resolution
- If GERD symptoms persist despite PPI, consider oesophageal manometry and 24-hour pH monitoring to guide further management (possible fundoplication in refractory cases)
How does h pylori attack ?
H pylori pathogenesis mechanism of injury virulence factors CagA VacA
H pylori pathogenesis gastric mucosa infection mechanism
H pylori urease ammonia mucosal damage colonisation gastric epithelium inflammation
How H. pylori Attacks
Step 1 — Survival in Acid: The Urease Shield
Step 2 — Colonisation & Burrowing into the Mucus Layer
Step 3 — Disruption of the Mucosal Barrier
| Enzyme/Product | Effect |
|---|---|
| Urease | Produces toxic ammonia; damages epithelium |
| Proteases & Lipases | Degrade mucus glycoproteins, thinning the protective gel |
| Phospholipases | Break down the hydrophobic lipid layer lining the stomach wall |
Step 4 — Injecting Virulence Proteins (CagA)
- Proliferative changes — abnormal cell growth (cancer risk)
- Cytoskeletal disruption — alters cell shape and tight junctions
- Pro-inflammatory signalling — triggers release of IL-8 and other cytokines, recruiting neutrophils
Step 5 — VacA Toxin
- Forms pores in cell membranes
- Causes vacuolation (bubble-like spaces) inside epithelial cells, leading to cell death
- Disrupts mitochondrial function
- Suppresses the local immune response, helping the bacteria evade clearance
Step 6 — Triggering Inflammation
- Acute phase: Neutrophils migrate to the mucosa and degranulate, releasing oxidative species that damage tissue further
- Chronic phase: Macrophages and lymphocytes accumulate — this is the hallmark of chronic active gastritis (Type B gastritis)
- Persistent inflammation leads to mucosal erosion, ulceration, and over decades, atrophy
The Disease Spectrum — Where It All Leads
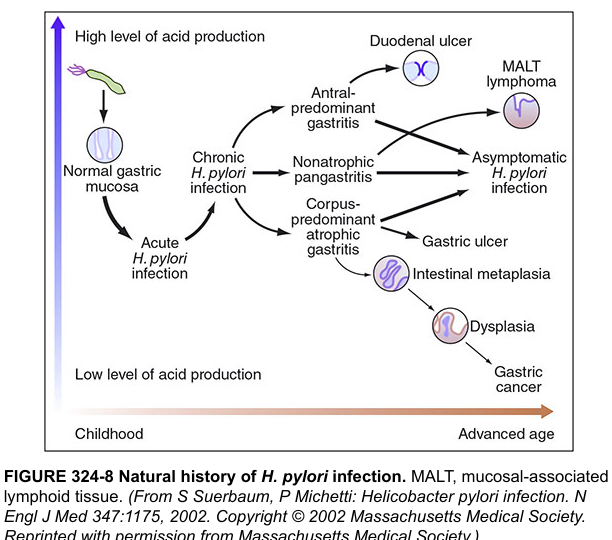
| Pattern | Consequence |
|---|---|
| Antral-predominant gastritis | High acid → Duodenal ulcer (your patient's pattern) |
| Corpus-predominant atrophic gastritis | Low acid → Gastric ulcer, gastric cancer |
| Pangastritis | MALT lymphoma, intestinal metaplasia |