20 yo patient came with a history of breathlessness and chest pain
Reading File
search_medical_text
young patient breathlessness chest pain differential diagnosis
search_medical_text
20 year old chest pain dyspnea evaluation workup ECG echocardiography
search_medical_image
chest pain breathlessness young patient diagnostic approach
GradeResponse
GradeResponse
GradeResponse
Here is a structured clinical approach for a 20-year-old presenting with breathlessness and chest pain:
Initial Clinical Assessment
History — Key Questions to Ask
| Domain | Questions |
|---|---|
| Chest pain | Onset (sudden vs. gradual), character (sharp/dull/pleuritic/pressure-like), location, radiation, duration, aggravating/relieving factors |
| Breathlessness | At rest or on exertion? Orthopnea? Paroxysmal nocturnal dyspnea? |
| Associated symptoms | Fever, cough, palpitations, syncope, leg swelling, rash |
| Triggers | Exercise, emotional stress, recent viral illness, trauma |
| Past history | Congenital heart disease, asthma, sickle cell, connective tissue disorders |
| Family history | Sudden cardiac death, cardiomyopathy, Marfan syndrome |
| Social history | Smoking, cocaine/stimulant use, oral contraceptive pill use (PE risk) |
Differential Diagnosis
Given the young age, the differentials span cardiac, pulmonary, and other causes:
Cardiac
| Condition | Key Clues |
|---|---|
| Myocarditis | Recent viral illness (1–3 weeks), elevated troponin, ST changes on ECG |
| Hypertrophic Cardiomyopathy (HCM) | Exertional symptoms, family history of sudden death, harsh systolic murmur |
| Pericarditis | Sharp, pleuritic pain, worse lying flat, relieved leaning forward; friction rub |
| Aortic dissection | Marfan habitus, tearing pain radiating to back, wide mediastinum |
| Arrhythmia (e.g., SVT, WPW) | Palpitations, sudden onset and termination |
| Mitral valve prolapse | Mid-systolic click, young women |
Pulmonary
| Condition | Key Clues |
|---|---|
| Spontaneous pneumothorax | Tall thin young male, sudden sharp pleuritic pain, reduced breath sounds |
| Pulmonary embolism (PE) | OCP use, immobility, long-haul travel, pleuritic pain, tachycardia |
| Asthma / EIB | Exertional wheeze, breathlessness, history of atopy |
| Pleuritis / pneumonia | Fever, productive cough, pleuritic pain |
Other
| Condition | Key Clues |
|---|---|
| Costochondritis | Reproducible tenderness on palpation |
| GERD / esophageal spasm | Burning, postprandial, relieved by antacids |
| Anxiety / panic attack | Situational, hyperventilation, no organic findings |
| Anemia | Exertional dyspnea, pallor, fatigue |
Initial Investigations
First-line (All Patients)
- ECG — ST changes (myocarditis, pericarditis, PE — S1Q3T3), LVH (HCM), delta wave (WPW), arrhythmia
- Chest X-ray — Pneumothorax, cardiomegaly, pleural effusion, mediastinal widening, pulmonary infiltrates
- Pulse oximetry + ABG if hypoxic
- CBC — Anemia, infection
- Troponin I/T — Myocardial injury (myocarditis, ACS)
Based on Clinical Suspicion
| Suspicion | Investigation |
|---|---|
| Myocarditis | Echo, cardiac MRI (gold standard), troponin, CRP/ESR, viral serology |
| HCM | Echocardiography — asymmetric septal hypertrophy (≥15 mm), LVOTO |
| PE | D-dimer, CT pulmonary angiography (CTPA), Wells score |
| Pericarditis | Echo (effusion), ESR, CRP, PR depression + diffuse ST elevation on ECG |
| Pneumothorax | CXR (expiratory film), CT chest if doubt |
| Arrhythmia | Holter monitor, EP study if WPW suspected |
Red Flags Requiring Urgent Escalation
- Syncope or presyncope with exertion → HCM, arrhythmia
- Oxygen saturation < 95%
- Troponin elevation
- Hemodynamic instability (hypotension, tachycardia)
- ST-segment elevation on ECG
- Absent breath sounds (pneumothorax)
- Tearing chest pain + Marfan features (aortic dissection)
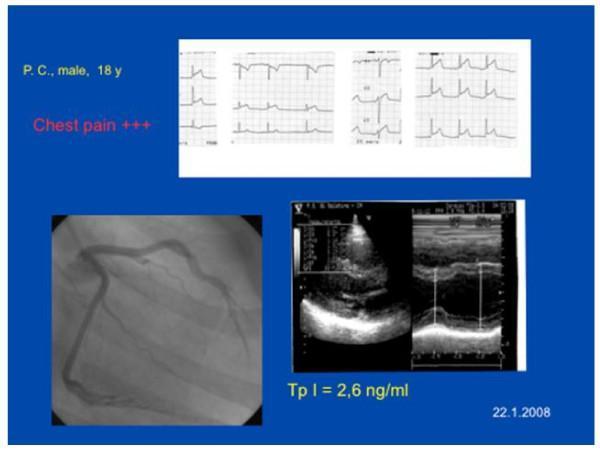
Illustrative Case Panel
Below is a clinical panel from a similar young patient — note the ST elevations on ECG, elevated troponin (2.6 ng/mL), and echocardiographic findings consistent with myocarditis/acute myocardial injury:
Summary Approach
Breathlessness + Chest Pain in 20 yo
↓
History + Vitals + O₂ sat
↓
ECG + CXR + Troponin
↓
Hemodynamically unstable? → Emergency management
Troponin ↑ / ST changes? → Myocarditis / ACS workup
Reduced breath sounds? → Pneumothorax
Pleuritic pain + risk? → Rule out PE
Exertional + FHx SCD? → HCM evaluation (Echo)
Reproducible tenderness? → Musculoskeletal
All clear? → Anxiety / functional
The most common serious causes in a 20-year-old are myocarditis (especially post-viral), spontaneous pneumothorax, HCM, and PE. ECG and troponin are the pivotal first tests. (Harrison's Principles of Internal Medicine, 21st Ed., p. 552)
Can you share any additional history, physical findings, or investigations already done? That will help narrow the differentials further.
This is a shared conversation. Sign in to Orris to start your own chat.