Uterus anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have rich textbook content and excellent anatomical diagrams. Let me compose a comprehensive answer.
Uterus Anatomy
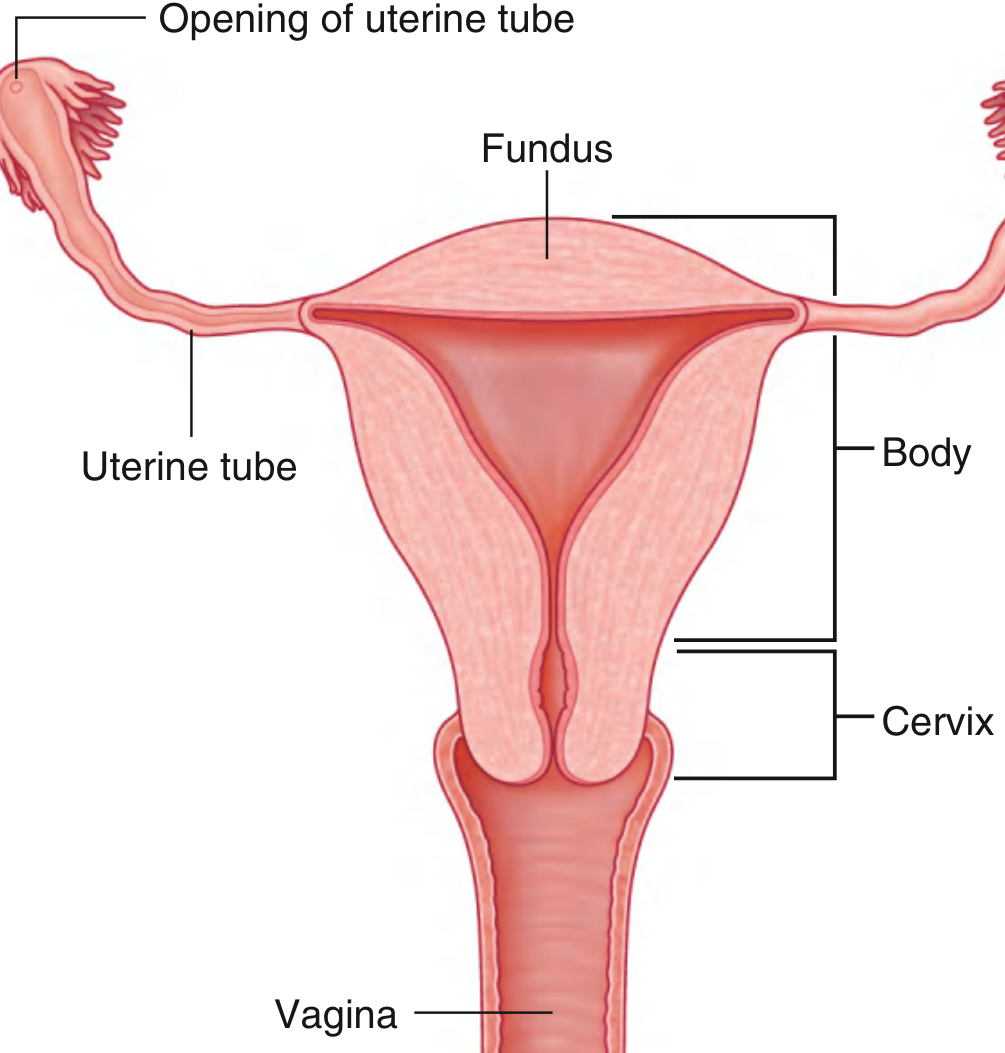
Fig. 5.54 - Gray's Anatomy for Students: Anterior view with the anterior halves of the uterus and vagina cut away
1. Overview and Position
The uterus is a thick-walled, hollow muscular organ situated in the midline of the pelvis, between the bladder anteriorly and the rectum posteriorly. It is a pear-shaped organ, roughly 7.5 cm long, 5 cm wide, and 2.5 cm thick in the nulliparous state (nonpregnant weight ~70 g). - Gray's Anatomy for Students
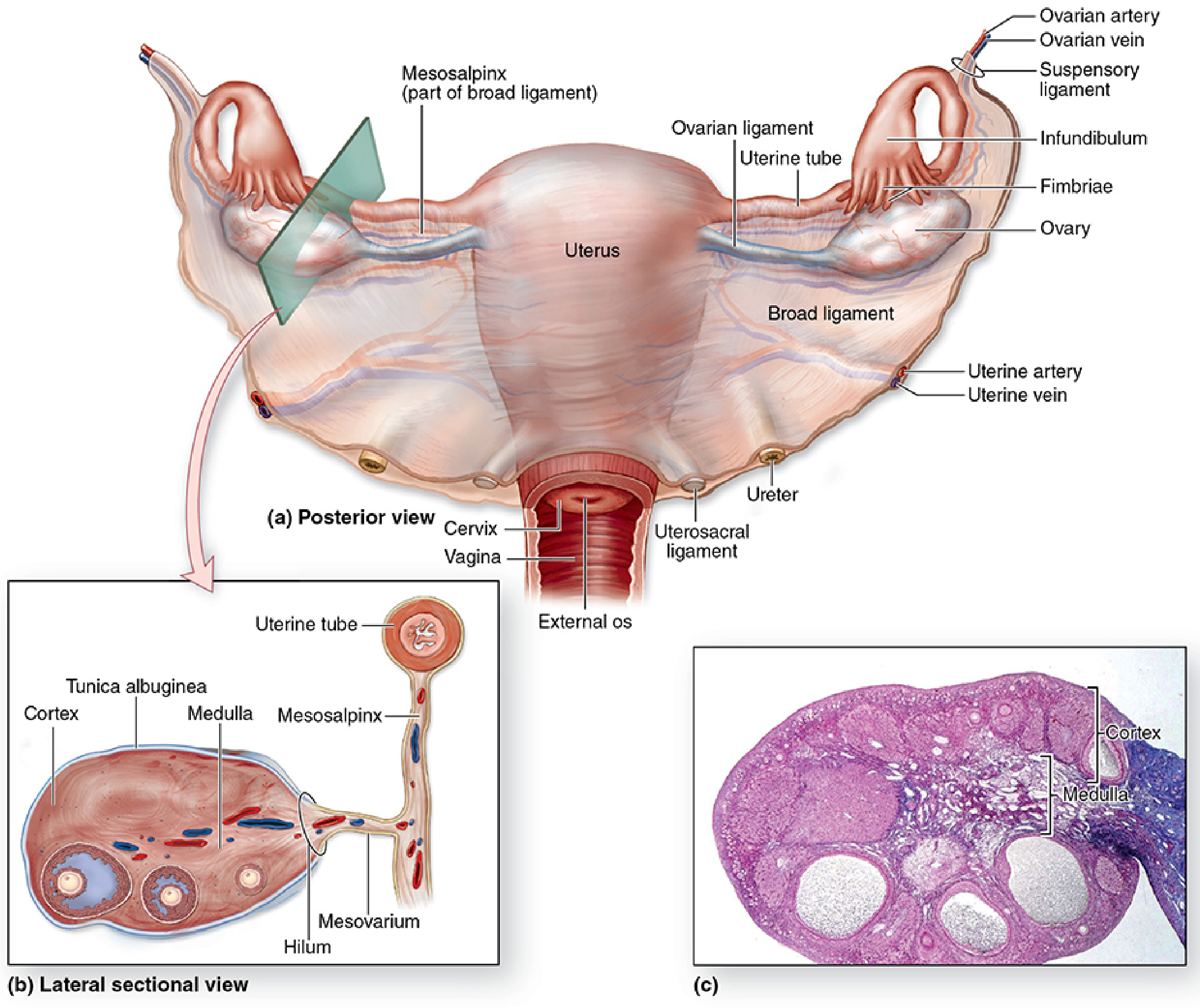
Fig. 22-1 - Junqueira's Basic Histology: Posterior view of the female pelvic organs with ligaments and vasculature
2. Parts of the Uterus
| Part | Description |
|---|---|
| Fundus | The rounded dome-shaped superior end, above the level of origin of the uterine tubes |
| Body (Corpus) | The main part; flattened anteroposteriorly; cavity is an inverted triangle when viewed from the front |
| Isthmus | A narrow constriction between the body and the cervix; becomes the lower uterine segment in pregnancy |
| Cervix | The cylindrical inferior part that projects into the vagina; divided into supravaginal and vaginal (portio vaginalis) parts |
The cavity of the body is a narrow slit viewed laterally but an inverted triangle anteriorly. Each superior corner communicates with a uterine tube; the inferior corner is continuous with the cervical canal. - Gray's Anatomy for Students
3. Wall Layers (from lumen outward)
Endometrium (innermost)
The mucosal lining rests directly on the myometrium with no submucosa. It has:
- Simple columnar epithelium with ciliated and secretory cells
- Tubular uterine glands that invaginate into the stroma
- Two functional zones:
- Basalis (basal layer) - not shed during menstruation; source of cyclical regeneration
- Functionalis (functional layer) - undergoes cyclic changes and is shed during menstruation (consists of the spongy layer deep and compact layer superficially)
- Color Atlas of Human Anatomy, Vol. 2 (Internal Organs)
Myometrium (middle, thickest layer)
Composed of smooth muscle cells, connective tissue, and blood vessels. Three layers are recognized:
- Inner (subvascular) layer - thin
- Middle layer - thickest; richly vascularized, spongelike; muscle fibers form a 3D meshwork; this is the layer mainly responsible for expelling the fetus during birth
- Outer (supravascular) layer - thin
During pregnancy, myometrial smooth muscle cells undergo first hyperplasia (early pregnancy) then hypertrophy (later pregnancy), enlarging the uterus to ~1100-1200 g at term. - Creasy & Resnik's Maternal-Fetal Medicine
Perimetrium (serosa, outermost)
The peritoneal covering of the uterus; continuous with the broad ligament.
4. Cervix
The cervix ("neck" of the uterus) has a different structure from the body:
-
Mostly fibrous connective tissue (collagen types I and III), with circumferentially oriented smooth muscle cells more abundant in the upper half
-
Endocervical canal lined by columnar epithelium with branching, tubular cervical glands secreting alkaline mucus
-
Vaginal part (ectocervix/portio) covered by stratified non-keratinized squamous epithelium
-
The transformation zone (squamocolumnar junction) where columnar epithelium meets squamous epithelium is the most common site for cervical carcinoma
-
Color Atlas of Human Anatomy, Vol. 2 (Internal Organs); Creasy & Resnik's Maternal-Fetal Medicine
5. Ligaments and Supports
| Ligament | Description |
|---|---|
| Broad ligament | Double fold of peritoneum extending from uterus to lateral pelvic walls; contains the mesosalpinx (encloses the uterine tubes), mesovarium (suspends the ovaries), and the round and ovarian ligaments |
| Round ligament | Runs from the uterine cornu, through the inguinal canal, to the labium majus; maintains anteversion |
| Cardinal (transverse cervical) ligament | Primary support against prolapse; extends from the cervix and vaginal vault to the pelvic sidewall |
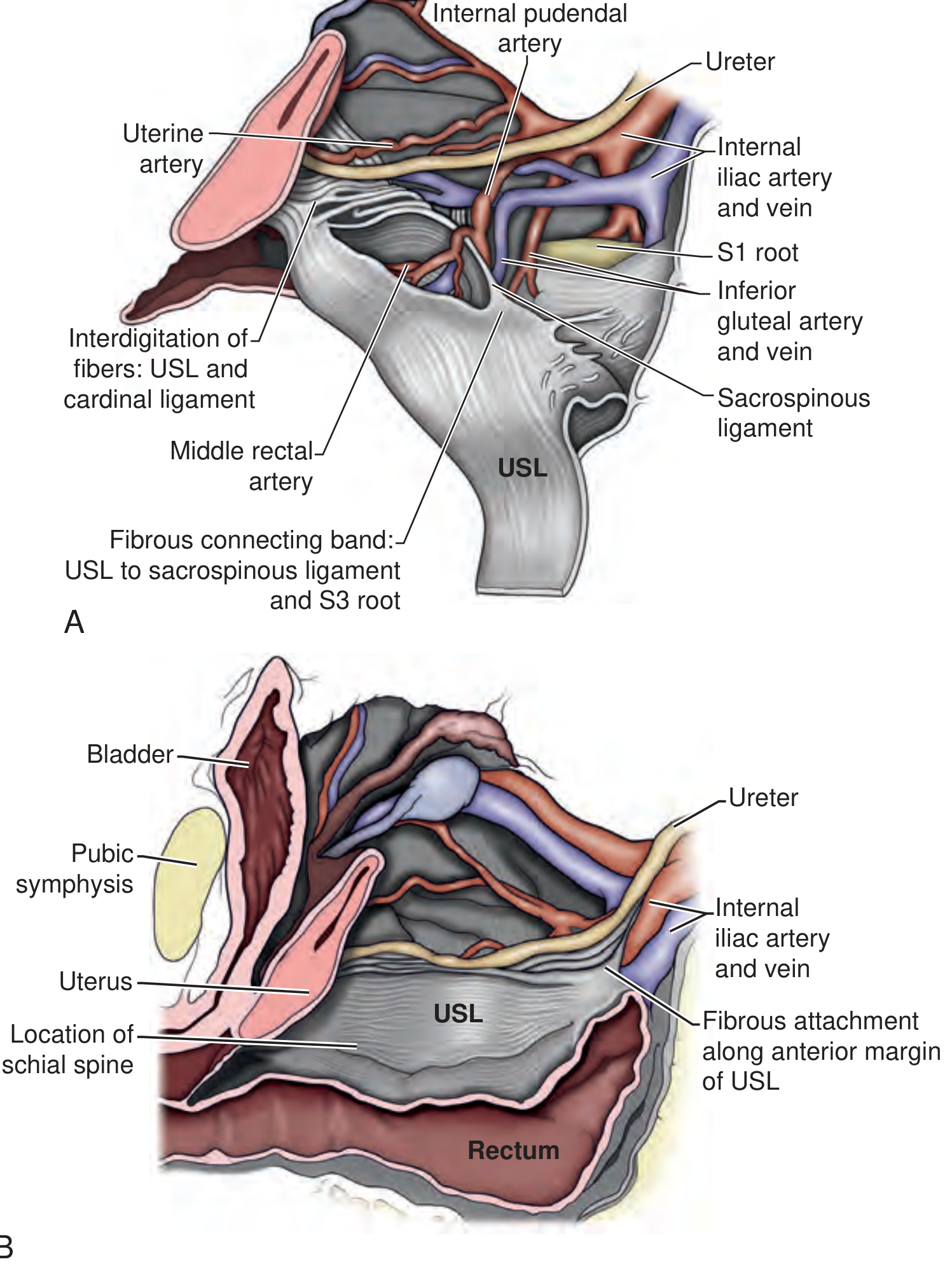
| Uterosacral ligament | Runs posteriorly from the cervix to the sacrum; maintains anteflexion |
| Pubocervical ligament | Runs anteriorly from the cervix to the pubic symphysis |
| Ovarian ligament | Connects ovary to uterine cornu |
| Suspensory ligament of ovary | Contains ovarian artery and vein |
6. Blood Supply
- Uterine artery - the main supply; a branch of the internal iliac artery. It crosses above the ureter ("water under the bridge") near the lateral fornix of the vagina - a key surgical landmark during hysterectomy
- Ovarian artery - supplements the upper uterus and tubes; arises directly from the aorta
- Venous drainage mirrors the arterial supply via the uterine venous plexus → internal iliac vein
During pregnancy, uterine blood flow increases 10-fold, from ~2% of cardiac output to ~17% at term, with 80-90% directed to the placenta. - Creasy & Resnik's Maternal-Fetal Medicine
7. Lymphatic Drainage
- Fundus and upper body → para-aortic (lumbar) lymph nodes (following the ovarian vessels)
- Body → internal and external iliac lymph nodes
- Cervix → internal and external iliac lymph nodes, and obturator nodes
8. Nerve Supply
- Sympathetic - T10-L1 (via hypogastric plexus); responsible for vasoconstriction and uterine contractions
- Parasympathetic - S2-S4 (pelvic splanchnic nerves / nervi erigentes)
- Sensory - pain from the body travels via T10-L1; pain from the cervix travels via S2-S4
9. Normal Position
- Anteverted (long axis of uterus angled forward relative to vagina at ~90°)
- Anteflexed (body tilted forward on the cervix)
- Retroversion/retroflexion are common anatomical variants (seen in ~20% of women)
10. Menstrual Cycle and the Endometrium
The endometrial functionalis undergoes three phases:
- Proliferative phase (days 5-14) - estradiol-driven restoration of the shed layer; glands elongate
- Secretory phase (days 15-28) - progesterone + estrogen cause glands to coil, secrete glycogen-rich mucus; stromal cells become pseudodecidual
- Menstrual phase (days 1-4) - progesterone withdrawal → ischemia → shedding of the functionalis
Curettage (D&C) removes the functionalis while leaving the basalis intact for regeneration. - Color Atlas of Human Anatomy, Vol. 2 (Internal Organs)
Key Clinical Notes:
- The ureter crosses under the uterine artery ~1.5 cm lateral to the cervix - the most common site of ureteric injury during hysterectomy (Gray's Anatomy for Students)
- Leiomyomas (fibroids) are benign smooth muscle tumors of the myometrium, the most common pelvic tumor in women
- Adenomyosis = endometrial tissue within the myometrium, causing an enlarged globular uterus, dysmenorrhea, and menorrhagia
- The lower uterine segment (formed from the isthmus) is the preferred site for Cesarean section incision
Diagram of uterus explain superior inferior posterior parts
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
I have excellent diagrams and rich textbook content. Now I'll compose the full explained answer.
Uterus Anatomy: Superior, Inferior, Anterior & Posterior Parts Explained
Diagram 1 - Anterior View (Sectioned)
Diagram 2 - Macroscopic Structure (Longitudinal & Anterior Views)
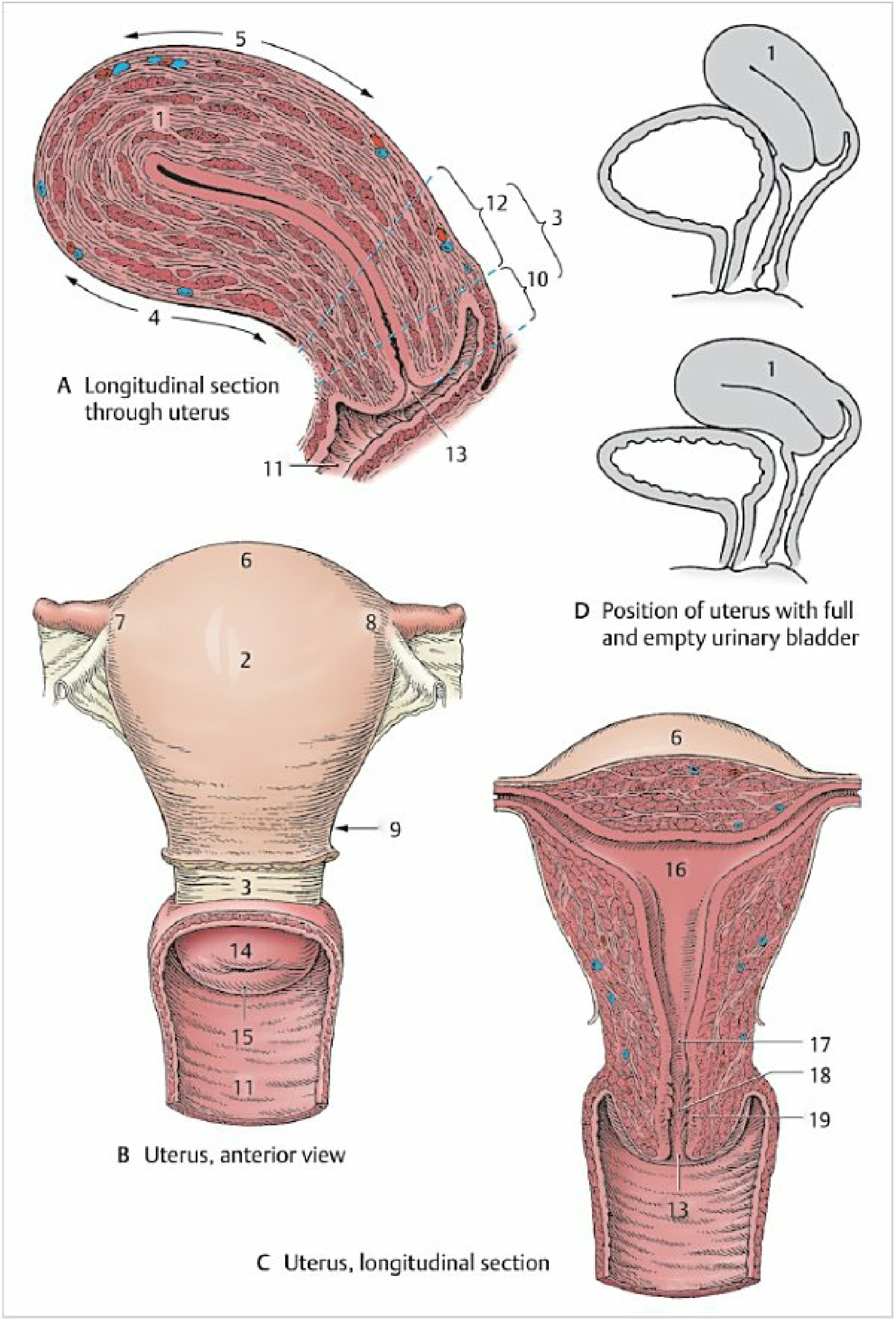
Fig. 7.5 - Color Atlas of Human Anatomy, Vol. 2: (A) Longitudinal section showing myometrium muscle layers. (B) Anterior view: fundus (6), body (2), isthmus (9), cervix (3), vagina (11). (C) Cavity view: fundus (6), uterine cavity (16), isthmus (17), cervical canal (18), palmate folds (19), external os (13). (D) How the uterus tilts differently when the bladder is full (top) vs empty (bottom).
Diagram 3 - Posterior View with Ligaments & Vasculature
Diagram 4 - Sagittal/Lateral Section Showing Uterus in Pelvic Context
Superior Parts
Fundus
- The rounded dome-shaped top of the uterus, projecting above the openings of the uterine (fallopian) tubes
- It is the most superior part of the organ
- During pregnancy it rises progressively into the abdomen; at term it can reach the epigastric region
- The fundus has a convex posterior surface and a slightly flattened anterior surface
- It is covered by peritoneum (perimetrium) on all sides
Uterine Horns (Cornua)
- Where the uterine tubes enter the uterus at its superolateral corners
- The right horn (cornu) and left horn are the entry points for sperm and the sites of tubal implantation in ectopic pregnancy
Middle Parts
Body (Corpus)
- The large middle portion, making up the upper two-thirds of the organ
- Anterior surface is nearly flat (vesical surface - faces the bladder)
- Posterior surface is convex (intestinal surface - faces the rectum and sigmoid colon)
- Both surfaces are covered by peritoneum
- Contains the triangular uterine cavity lined by endometrium
Isthmus
- A narrow constriction ~1 cm long between the body and the cervix
- Identifiable externally as a shallow groove
- In pregnancy, it expands dramatically to form the lower uterine segment - the preferred incision site for Cesarean section
- Internally marked by the histological internal os
Inferior Parts
Cervix
- The cylindrical lower one-third of the uterus, directed posteriorly and inferiorly
- ~2.5 cm long; mostly fibrous connective tissue with less smooth muscle than the body
- Divided into:
- Supravaginal part - above the vagina; the uterosacral and cardinal ligaments attach here
- Vaginal part (portio vaginalis) - protrudes into the vaginal vault and is visible on speculum exam
- The external os opens at the tip of the portio into the vagina
- Round/circular in nulliparous women
- Slit-like / transverse after vaginal delivery
- The cervical canal runs between the internal os (above) and external os (below); it has characteristic palmate (arbor vitae) folds
- Lined by columnar epithelium; the transformation zone (junction with the squamous epithelium of the vaginal portio) is the most common site for cervical carcinoma
- Color Atlas of Human Anatomy, Vol. 2 (Internal Organs)
Anterior Relations
The peritoneum passes from the anterior abdominal wall over the superior surface of the bladder and reflects onto the anterior surface of the uterus at the cervico-body junction, forming the:
Vesicouterine pouch - a shallow peritoneal recess between the bladder and the anterior surface of the uterus. It becomes very shallow (or obliterated) when the bladder is full.
- Anteriorly: Urinary bladder
- At the cervix: The ureter passes ~1.5 cm lateral to the cervix, crossing beneath the uterine artery ("water under the bridge") - key surgical landmark in hysterectomy
Posterior Relations
The peritoneum continues over the fundus and all the way down the posterior surface of the uterus onto the posterior wall of the vagina, then reflects onto the rectum, forming the:
Rectouterine pouch (Pouch of Douglas) - the deepest point of the female peritoneal cavity; bounded laterally by the uterosacral folds containing the uterosacral ligaments and inferior hypogastric nerve plexus.
- Posteriorly: Rectum and sigmoid colon (separated by the pouch of Douglas)
- The posterior surface of the uterus and broad ligament can be felt through the rectum on rectal examination
Clinical note: Pathological fluid (blood in ectopic rupture, pus in PID, malignant ascites) collects in the pouch of Douglas - it can be drained by posterior colpotomy (needle through the posterior vaginal fornix). - Color Atlas of Human Anatomy, Vol. 2
Summary Table
| Direction | Structure / Part | Key Relations |
|---|---|---|
| Superior | Fundus, uterine horns | Uterine tubes enter here; rises into abdomen in pregnancy |
| Anterior | Vesical (anterior) surface | Bladder; vesicouterine pouch (peritoneum) |
| Posterior | Intestinal (posterior) surface | Rectum; pouch of Douglas (deepest female peritoneal space) |
| Inferior | Cervix (supravaginal + vaginal parts) | Projects into vagina; external os opens inferiorly |
| Lateral | Broad ligament, parametrium | Uterine artery, ureter, ovary, uterine tube |
| Isthmus | Junction of body and cervix | Lower uterine segment in pregnancy; Cesarean incision site |
Position
The normal uterus is:
- Anteverted - the whole uterus is tilted forward relative to the vaginal axis (~90° angle)
- Anteflexed - the body is flexed forward on the cervix
When the bladder is full, it pushes the uterus posteriorly, reducing the degree of anteversion (shown in diagram D above). When the bladder is empty, full anteversion and anteflexion are restored. - Color Atlas of Human Anatomy, Vol. 2
Broad ligament of uterus explain it to me like I'm newbie
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I have everything I need - a beautiful diagram and rich textbook content. Let me now write a beginner-friendly explanation.
The Broad Ligament of the Uterus - A Beginner's Guide
Start with a Simple Picture
Imagine you're holding a bedsheet by its two long edges - one person holds the left edge, another holds the right edge, and the sheet hangs flat between them. Now imagine the uterus is sewn along the middle of that sheet, and the sheet is stretched sideways across your pelvis.
That sheet = the broad ligament.
What Exactly Is It?
The broad ligament is not a rope-like ligament (most ligaments look like cords or straps). Instead, it is a double-layered sheet of peritoneum (the thin, smooth membrane that lines your abdominal and pelvic cavity).
Think of it like a taco shell wrapped around the uterus from both sides:
- The front layer = anterior leaf
- The back layer = posterior leaf
These two layers extend sideways from the uterus all the way to the lateral wall of the pelvis - on both the left and right sides. This is why it is called broad - it is wide and flat, not narrow. - Gray's Anatomy for Students
The Diagram
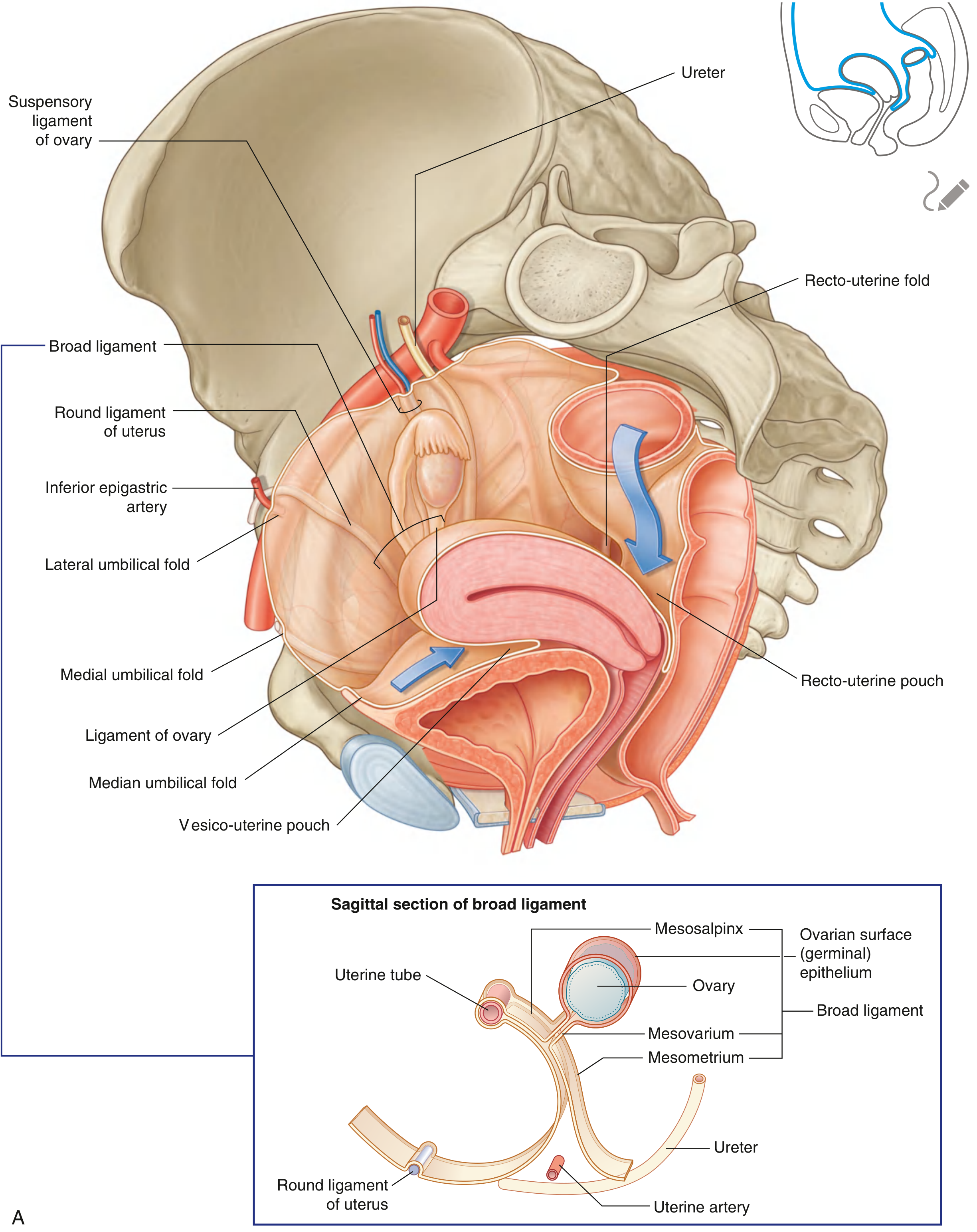
Fig. 5.60A - Gray's Anatomy for Students. The inset (bottom) is the most important - it shows the three zones of the broad ligament in cross-section.
The Three Zones - Think of a Flying Bird 🐦
Look at the inset in the bottom of the diagram above. The broad ligament has three named sections, from top to bottom:
1. Mesosalpinx (Top zone - the "wing tip")
- "Meso" = middle / connecting | "salpinx" = tube
- This is the topmost free edge of the broad ligament
- It wraps around and suspends the fallopian (uterine) tube up in the air
- Think of it as the pocket that holds the fallopian tube, keeping it floating above everything else
2. Mesovarium (Middle zone - the "bump on the wing")
- "Ovarium" = ovary
- A small, backward-pointing fold of the broad ligament that attaches to the ovary
- The ovary hangs from this like a pendant from a necklace
- Note: the ovary itself is NOT inside the broad ligament - it is attached to its back surface and sits just behind it
3. Mesometrium (Bottom zone - the "main body of the wing")
-
"Metrium" = uterus
-
The largest, biggest part of the broad ligament
-
It stretches from the body of the uterus sideways to the pelvic wall
-
Contains the most important structures (see below)
-
Gray's Anatomy for Students; Campbell-Walsh Urology
What Does the Broad Ligament Carry Inside It?
This is where it gets really interesting. The broad ligament is not just a sheet of tissue - it is like a highway tunnel carrying many important things:
| Structure Inside | What It Is | Which Zone |
|---|---|---|
| Uterine artery | Main blood supply to the uterus (branch of internal iliac artery) | Mesometrium (base) |
| Uterine vein | Drains blood from the uterus | Mesometrium (base) |
| Ureter | Tube from kidney to bladder - passes just below the uterine artery | Mesometrium (base) |
| Ovarian vessels | Blood supply to the ovary | Near mesovarium |
| Round ligament of uterus | Cord-like band that keeps the uterus tilted forward | Mesometrium (front part) |
| Ligament of the ovary | Connects the ovary to the uterus | Mesovarium area |
| Lymphatics & nerves | Drainage and nerve supply | Throughout |
| Fallopian tube | The tube connecting ovary to uterus | Mesosalpinx |
The uterine artery and ureter both travel at the base of the broad ligament. The artery crosses over the ureter here ("water under the bridge") - this is one of the most important surgical landmarks in the entire pelvis. - Campbell-Walsh Urology
What Does the Broad Ligament Actually DO?
1. It creates two separate spaces in the pelvis
By stretching from the uterus to both pelvic walls, the broad ligament divides the pelvis into:
- Vesicouterine pouch (front space) - between bladder and uterus
- Rectouterine pouch / Pouch of Douglas (back space) - between uterus and rectum
2. It keeps the uterus in place (a little)
The broad ligament provides some lateral stability to the uterus - stopping it from flopping too far left or right. However, it is NOT the main support against prolapse (that job belongs to the cardinal and uterosacral ligaments).
3. It carries the "lifelines" to the uterus and ovary
All the blood vessels, lymphatics, and nerves running to the uterus and ovary travel inside the broad ligament. Remove the broad ligament and you cut off the blood supply.
A Quick Analogy to Tie It All Together
Imagine the uterus is a person standing in the middle of a room. The broad ligament is like their coat - it hangs from their shoulders (fallopian tubes at the top), drapes over their sides (mesometrium), and the coat pockets hold their valuables (blood vessels, ureter, nerves). On each side of the room there's a wall (the pelvic sidewall), and the coat stretches all the way to both walls, keeping the person centered.
Clinical Relevance (Why Doctors Care)
- Hysterectomy (uterus removal): Surgeons must carefully open the broad ligament, identify the ureter running inside it, then clip the uterine artery - all without accidentally cutting the ureter
- Broad ligament hematoma: After trauma or difficult delivery, blood can collect inside the two layers of the broad ligament, forming a dangerous expanding mass
- Broad ligament fibroid: A uterine fibroid can grow sideways into the broad ligament, making surgery very difficult because of the vessels and ureter inside
- Endometriosis: Endometrial tissue commonly implants on the posterior leaf of the broad ligament
Summary in One Sentence
The broad ligament is a wide, flat, double-layered sheet of peritoneum that drapes over the uterus and stretches sideways to the pelvic walls on both sides, carrying the uterine tubes (top), suspending the ovaries (back), and transporting the uterine blood vessels, ureter, round ligament, and nerves inside its base.
This is a shared conversation. Sign in to Orris to start your own chat.