Ecmo for 10 marks dnb final theory exam in simple language
Reading File
Finding Sources
Searching the Web
ECMO extracorporeal membrane oxygenation DNB final exam 10 marks
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have everything needed to write a complete DNB 10-mark answer. Here it is:
ECMO (Extracorporeal Membrane Oxygenation) - DNB Final Theory Answer (10 Marks)
Definition
ECMO (also called Extracorporeal Life Support / ECLS) is a form of prolonged cardiopulmonary support where blood is drained from the patient, oxygenated and decarbonated outside the body via an artificial membrane lung, and returned to the patient. It is used when conventional therapy fails for severe, potentially reversible cardiac and/or respiratory failure.
Basic Circuit Components
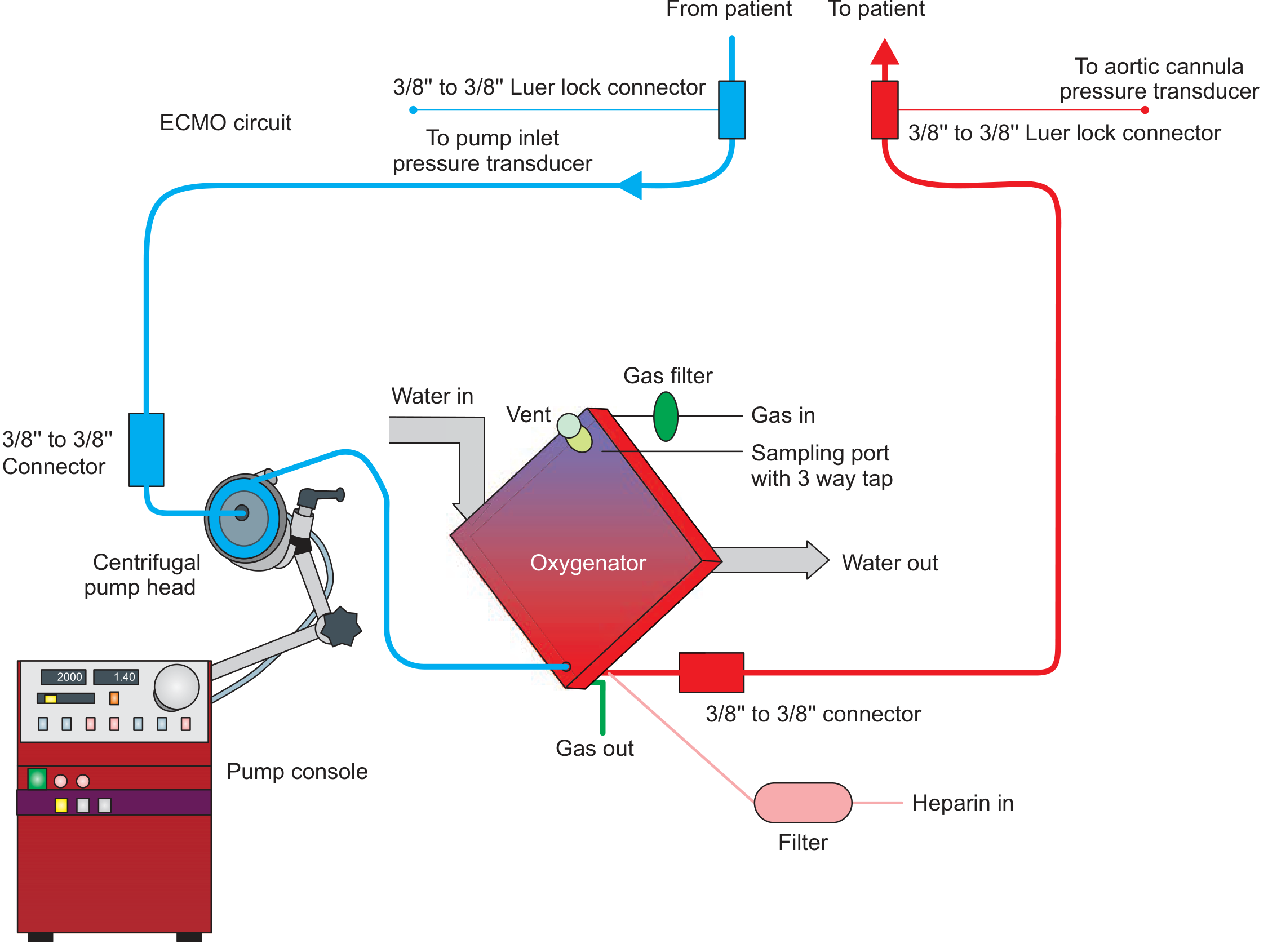
The circuit has 4 key parts:
| Component | Function |
|---|---|
| Inflow (drainage) cannula | Drains venous blood from patient into circuit |
| Centrifugal pump | Propels blood through the circuit |
| Membrane oxygenator | Adds O2 and removes CO2 (mimics lung) |
| Outflow (return) cannula | Returns blood to patient (vein or artery) |
Heparin is infused continuously into the circuit to prevent clotting.
Types of ECMO
1. Veno-Venous (VV) ECMO
- Blood drained from a vein, returned to a vein
- Provides respiratory support only - does NOT support cardiac function
- Most common configuration: right femoral vein (inflow) + right internal jugular vein (outflow)
- An alternative: dual-lumen single cannula via right IJV
- Used for: severe ARDS, refractory respiratory failure (without cardiac dysfunction)
2. Veno-Arterial (VA) ECMO
- Blood drained from a vein, returned to an artery (usually femoral artery)
- Provides both cardiac AND respiratory support - bypasses the heart and lungs
- Used for: cardiogenic shock, cardiac arrest, biventricular failure, refractory hypoxemia with cardiac dysfunction
- Risk: can cause pulmonary edema and LV distension because it does not directly unload the LV - may need additional LV unloading (IABP or Impella)
Indications
VV ECMO (Respiratory)
- Severe ARDS with PaO2/FiO2 < 80 mmHg despite optimal mechanical ventilation
- Severe hypercapnia (pH < 7.15) unresponsive to ventilation
- Life-threatening air leak syndromes
- Bridge to lung transplantation
- ECMO threshold: Murray Lung Injury Score > 3 or pH < 7.2 despite 6 hours of optimization
VA ECMO (Cardiac)
- Cardiogenic shock unresponsive to inotropes/vasopressors
- Cardiac arrest refractory to CPR (E-CPR)
- Myocarditis with acute severe cardiac failure
- Post-cardiotomy cardiogenic shock
- High-risk PCI or cardiac surgery
Contraindications
Absolute:
- Irreversible/terminal illness (no bridge goal)
- Severe, irreversible neurologic injury
- Aortic dissection (for VA ECMO)
Relative:
- Prolonged CPR without perfusion (>60 min)
- Advanced age with multiple comorbidities
- Severe peripheral vascular disease (limits femoral access)
- Active bleeding or coagulopathy (anticoagulation required)
- Immunosuppression (high infection risk)
Monitoring on ECMO
- Circuit flow: 60-80 mL/kg/min for VV; target adequate cardiac output for VA
- Sweep gas (FiO2 + flow rate): controls CO2 removal - increase sweep to reduce PaCO2
- Pre- and post-oxygenator blood gases
- ACT / anti-Xa levels for heparin titration
- Daily circuit inspection for clots, raceway tears
- SaO2 monitoring: in VV ECMO, SpO2 of 85-92% is acceptable ("permissive hypoxemia")
"Lung Rest" Strategy on ECMO
Once on VV ECMO, the ventilator is set to very low, non-injurious settings to allow the lungs to recover:
- Low tidal volume (4 mL/kg)
- Low RR (10/min)
- Low PEEP (5-10 cmH2O)
- Low FiO2 (0.3-0.4)
This prevents ventilator-induced lung injury (VILI) while the lungs heal.
Complications
| Category | Complication |
|---|---|
| Bleeding | Cannula site bleeding, intracranial hemorrhage (from anticoagulation) |
| Thrombosis | Circuit clots, stroke, limb ischemia |
| Infection | Cannula-site infection, bloodstream infection |
| Cardiac (VA) | LV distension, pulmonary edema - "North-South syndrome" |
| Limb ischemia | Distal limb ischemia from arterial cannula (VA ECMO) - needs distal perfusion cannula |
| Hemolysis | Due to shear stress across the pump |
| Recirculation | In VV ECMO - oxygenated blood re-enters the inflow cannula |
| Air embolism | Circuit breach |
Key Trials (Important for Exam)
| Trial | Year | Findings |
|---|---|---|
| CESAR | 2009 | ECMO at specialist center improved survival/disability-free survival in severe ARDS vs conventional ventilation |
| EOLIA | 2018 | No significant 60-day mortality difference (VV ECMO vs control), BUT 28% crossover to ECMO in control group - Bayesian analysis favored ECMO |
Weaning from ECMO
- VV ECMO: Gradually reduce sweep gas flow; if patient tolerates FiO2 1.0 on the circuit with sweep gas turned to near zero and SpO2 is maintained - ready to decannulate
- VA ECMO: Wean by gradually reducing flow (by 0.5-1 L/min increments); reassess cardiac function by echo at each step
Summary Table: VV vs VA ECMO
| Feature | VV ECMO | VA ECMO |
|---|---|---|
| Support provided | Lungs only | Heart + Lungs |
| Cannulation | Vein to Vein | Vein to Artery |
| Use in ARDS | Yes | No (unless + cardiac failure) |
| Cardiac output | Patient's own heart | Bypasses heart |
| LV unloading needed | No | Yes (often) |
| Risk of limb ischemia | Low | High (femoral artery) |
One-Line Summary for Last-Minute Revision
ECMO = external heart-lung machine for severe, reversible cardiac/respiratory failure. VV for lungs only, VA for heart+lungs. Core circuit = drainage cannula + centrifugal pump + membrane oxygenator + return cannula. Main complications = bleeding, clotting, infection, LV distension (VA). Key trial = CESAR (VV ECMO improved outcomes in severe ARDS).
Sources: Fishman's Pulmonary Diseases and Disorders, Fischer's Mastery of Surgery 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.