Anatomy of knee joint and common injuries to it ,signs and symptoms for differential diagnosis between them
Reading File
search_medical_text
knee joint anatomy bones ligaments menisci bursae muscles
search_medical_image
knee joint anatomy diagram ligaments meniscus
GradeResponse
GradeResponse
search_medical_text
ACL PCL MCL LCL meniscus tear knee injury signs symptoms clinical features
search_medical_image
knee ligament injury ACL tear clinical tests Lachman McMurray
GradeResponse
GradeResponse
Here is a comprehensive overview of the anatomy of the knee joint and common injuries with differential diagnosis.
Knee Joint: Anatomy, Common Injuries & Differential Diagnosis
PART 1 — ANATOMY OF THE KNEE JOINT
(Bailey & Love's Short Practice of Surgery, 28th Ed., p. 583)
Joint Type & Compartments
The knee is a synovial hinge joint — the largest and most complex joint in the body. It consists of:
- Two condyloid tibiofemoral joints (medial & lateral)
- One sellar (saddle-shaped) patellofemoral joint
- Three compartments: medial, lateral, and patellofemoral
The shape makes the joint inherently unstable; stability depends on static and dynamic stabilisers.
Bony Anatomy
| Bone | Contribution |
|---|---|
| Femur | Medial & lateral condyles; intercondylar notch |
| Tibia | Medial & lateral tibial plateaus; tibial spines |
| Patella | Largest sesamoid bone; sits in femoral trochlear groove |
| Fibula | Head articulates with lateral tibial condyle (not a true knee joint but relevant for LCL/PLC) |
Ligaments (Static Stabilisers)
| Ligament | Location | Primary Function |
|---|---|---|
| ACL (Anterior Cruciate) | Within joint, intercondylar notch | Resists anterior tibial translation; prevents internal rotation |
| PCL (Posterior Cruciate) | Within joint, intercondylar notch | Resists posterior tibial translation |
| MCL (Medial Collateral) | Medial aspect | Resists valgus stress; restrains external rotation |
| LCL (Lateral Collateral) | Lateral aspect | Resists varus stress |
| Posterolateral Corner (PLC) | Posterior-lateral capsule | Popliteus tendon, arcuate ligament, popliteofibular ligament |
| Posteromedial Corner | Posterior-medial capsule | Oblique popliteal ligament, semimembranosus attachments |
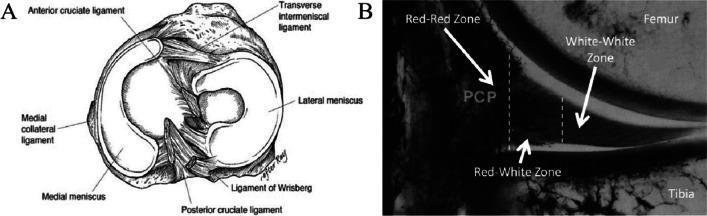
Menisci
The knee has two fibrocartilaginous menisci sitting on the tibial plateau:
| Feature | Medial Meniscus | Lateral Meniscus |
|---|---|---|
| Shape | C-shaped (larger) | O-shaped / circular (smaller) |
| Mobility | Less mobile (attached to MCL & capsule) | More mobile |
| Blood supply | Peripheral red-red zone only | Peripheral red-red zone only |
| Injury rate | More commonly torn | Less commonly torn |
Vascular zones of the meniscus (critical for repair planning):
- Red-Red Zone (peripheral): well-vascularised → heals spontaneously
- Red-White Zone (transitional): partial vascularity → may heal with repair
- White-White Zone (central): avascular → poor healing; resection often needed
Muscles (Dynamic Stabilisers)
| Group | Muscles | Action |
|---|---|---|
| Extensors | Quadriceps femoris (rectus femoris, vastus medialis/lateralis/intermedius) + patellar tendon | Knee extension; patellofemoral control |
| Flexors | Hamstrings (biceps femoris, semitendinosus, semimembranosus) | Knee flexion; ACL co-stabilisers |
| Pes anserinus | Sartorius, gracilis, semitendinosus | Medial stabilisation |
| Popliteus | Popliteus | Unlocks the knee; posterolateral stability |
| Iliotibial band | TFL + iliotibial tract | Lateral knee stability |
Bursae
Key bursae around the knee:
- Prepatellar bursa (between skin and patella)
- Infrapatellar bursa (superficial and deep)
- Pes anserinus bursa (medial, under pes anserinus tendons)
- Baker's cyst / Popliteal bursa (posterior, communicates with joint)
- Semimembranosus bursa
PART 2 — COMMON KNEE INJURIES
PART 3 — DIFFERENTIAL DIAGNOSIS: SIGNS & SYMPTOMS
1. Anterior Cruciate Ligament (ACL) Tear
Mechanism: Non-contact deceleration/pivoting, or direct blow; knee forced into valgus + internal rotation; hyperextension.
Signs & Symptoms:
- Audible/felt "pop" at time of injury (classic)
- Immediate haemarthrosis (within 1–2 hours; hallmark finding)
- Rapid, tense joint effusion
- Inability to continue activity
- Feeling of knee "giving way" (instability)
- Anterior knee pain
Clinical Tests:
- Lachman Test (most sensitive, 85%) — knee at 20–30° flexion; anterior force on tibia; positive = increased anterior translation with soft end-point

- Anterior Drawer Test — knee at 90°; anterior tibial pull; less sensitive than Lachman
- Pivot Shift Test — most specific for ACL functional instability
Investigations: MRI (gold standard for soft tissue)
2. Posterior Cruciate Ligament (PCL) Tear
Mechanism: Dashboard injury (posterior force on proximal tibia in flexed knee); hyperflexion; hyperextension.
Signs & Symptoms:
- Less dramatic presentation than ACL
- Posterior knee pain
- Haemarthrosis (less tense than ACL)
- Posterior sag of tibia (gravity sign)
- Difficulty with stairs (quadriceps overload)
- Vague instability (often underdiagnosed)
Clinical Tests:
- Posterior Drawer Test — positive (tibia pushed posteriorly)
- Posterior Sag Sign (Godfrey's) — supine, hips/knees at 90°; tibia visually sags posteriorly
- Quadriceps Active Test — contraction of quadriceps reduces posterior sag
3. Medial Collateral Ligament (MCL) Tear
Mechanism: Valgus stress (blow to lateral knee); common in contact sports.
Grading:
| Grade | Description |
|---|---|
| I | Sprain; fibres intact; point tenderness; no laxity |
| II | Partial tear; moderate laxity; pain + swelling |
| III | Complete rupture; gross laxity; may be painless |
Signs & Symptoms:
- Medial knee pain and tenderness along MCL
- Swelling (usually not haemarthrosis unless combined injury)
- Valgus deformity in severe cases
- Instability on lateral loads
Clinical Tests:
- Valgus Stress Test at 0° and 30° — laxity at 30° = isolated MCL; laxity at 0° = MCL + capsule/cruciate involvement
4. Lateral Collateral Ligament (LCL) / Posterolateral Corner (PLC) Injury
Mechanism: Varus stress; direct medial blow; hyperextension.
Signs & Symptoms:
- Lateral knee pain and tenderness over LCL (fibular head to lateral epicondyle)
- Varus deformity
- Peroneal nerve symptoms (foot drop, paraesthesia) if severe PLC injury
- Posterolateral rotatory instability
Clinical Tests:
- Varus Stress Test at 0° and 30°
- Dial Test — external tibial rotation at 30° and 90°; increased rotation at 30° alone = PLC injury; at both = PLC + PCL
- External Rotation Recurvatum Test
5. Meniscal Tear
Mechanism: Twisting on a loaded, slightly flexed knee; degenerative tears in older patients.
Signs & Symptoms:
- Joint line tenderness (medial or lateral) — most reliable sign
- Effusion (slower onset, 24–48 hours after acute injury)
- Locking (bucket-handle tear — true mechanical block to extension)
- Clicking / clicking sensation with rotation
- Pain on squatting or climbing stairs
- Delayed onset of swelling
Clinical Tests:
- McMurray's Test — knee from full flexion with varus/valgus + rotation; positive = palpable/audible click with pain at joint line
- Apley's Grind Test — prone, knee 90°; compression + rotation = pain (meniscal); distraction + rotation = pain (ligamentous)
- Thessaly Test (20° flexion, weight-bearing rotation) — sensitive for degenerative tears
- Joint line tenderness — simple but clinically significant
6. Patellar Dislocation / Patellofemoral Syndrome
Mechanism: Lateral patellar dislocation — valgus + external rotation (especially in adolescent females with trochlear dysplasia).
Signs & Symptoms:
- Visible lateral displacement of patella (acute dislocation)
- Medial peripatellar tenderness (retinaculum tear)
- Haemarthrosis
- Apprehension sign — patient resists lateral patellar glide
- Chronic patellofemoral pain: diffuse anterior knee pain, worse with stairs/squatting/prolonged sitting ("theatre sign")
7. Patellar Tendon / Quadriceps Tendon Rupture
Mechanism: Eccentric loading; more common in athletes (patellar) or elderly/systemic disease (quadriceps).
Signs & Symptoms:
- Sudden pain and inability to extend the knee
- Palpable gap in tendon
- High-riding patella (patella alta — patellar tendon rupture) or low-riding (patella baja — quadriceps rupture)
- Loss of active straight-leg raise
8. Tibial Plateau Fracture
Mechanism: Axial load + valgus/varus; "bumper fracture" from vehicular impact.
Signs & Symptoms:
- Haemarthrosis (lipohemarthrosis on X-ray = fat-fluid level)
- Severe pain and swelling
- Inability to weight-bear
- Compartment syndrome risk
- Associated neurovascular injury (popliteal artery, peroneal nerve)
PART 4 — COMPARATIVE DIFFERENTIAL DIAGNOSIS TABLE
| Feature | ACL Tear | PCL Tear | MCL Tear | LCL/PLC Tear | Meniscal Tear | Patellar Dislocation |
|---|---|---|---|---|---|---|
| Mechanism | Pivot/valgus + IR | Dashboard/hyperflexion | Valgus blow | Varus/hyperextension | Twisting on flexed knee | Valgus + ER |
| Pop at injury | ✅ Classic | Rare | Sometimes | Sometimes | Rare | Sometimes |
| Haemarthrosis timing | Immediate (1–2 hrs) | Moderate | Mild/none | Mild | Delayed (24–48 hrs) | Immediate |
| Effusion | Large, tense | Moderate | Small-moderate | Small | Moderate, delayed | Moderate |
| Pain location | Central/diffuse | Posterior | Medial | Lateral | Joint line (M or L) | Peripatellar/medial |
| Instability | Anterior, rotatory | Posterior | Valgus | Varus, posterolateral | Locking/clicking | Lateral subluxation |
| Key test | Lachman | Posterior sag/drawer | Valgus stress | Varus stress/Dial | McMurray/Apley | Apprehension sign |
| Locking | ❌ | ❌ | ❌ | ❌ | ✅ (bucket-handle) | Occasional |
| X-ray finding | Segond fracture (lateral capsule avulsion) | Reverse Segond | Normal | Normal/fibular avulsion | Normal | Lateral patellar shift |
| MRI | ACL discontinuity | PCL discontinuity | MCL edema/tear | LCL/popliteus tear | Meniscal signal change | Trochlear dysplasia |
Key Distinguishing Pearls
- Immediate haemarthrosis → think ACL tear, patellar dislocation, tibial plateau fracture (not meniscal tear, which is delayed)
- Mechanical locking (inability to fully extend) → bucket-handle meniscal tear until proven otherwise
- "Pop" + giving way + rapid swelling → ACL tear (the classic triad)
- Posterior sag in supine position → PCL injury
- Joint line tenderness → meniscal pathology
- Medial tenderness + valgus laxity → MCL injury
- Peroneal nerve deficit → suspect PLC/LCL injury
- Apprehension on lateral patellar glide → patellofemoral instability
Sources: Bailey & Love's Short Practice of Surgery, 28th Edition (pp. 511, 583); supplemented from standard orthopaedic clinical knowledge.
This is a shared conversation. Sign in to Orris to start your own chat.