Serum cortisol and serum acth are low what's the treatment sudden for over tiredness fludocprtisone pr other dose and details
Reading File
Finding Sources
Finding Sources
Searching PubMed
"adrenal insufficiency" AND "glucocorticoid replacement" AND "fludrocortisone"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a complete, well-sourced answer. Here it is:
Low Cortisol + Low ACTH = Secondary (Central) Adrenal Insufficiency
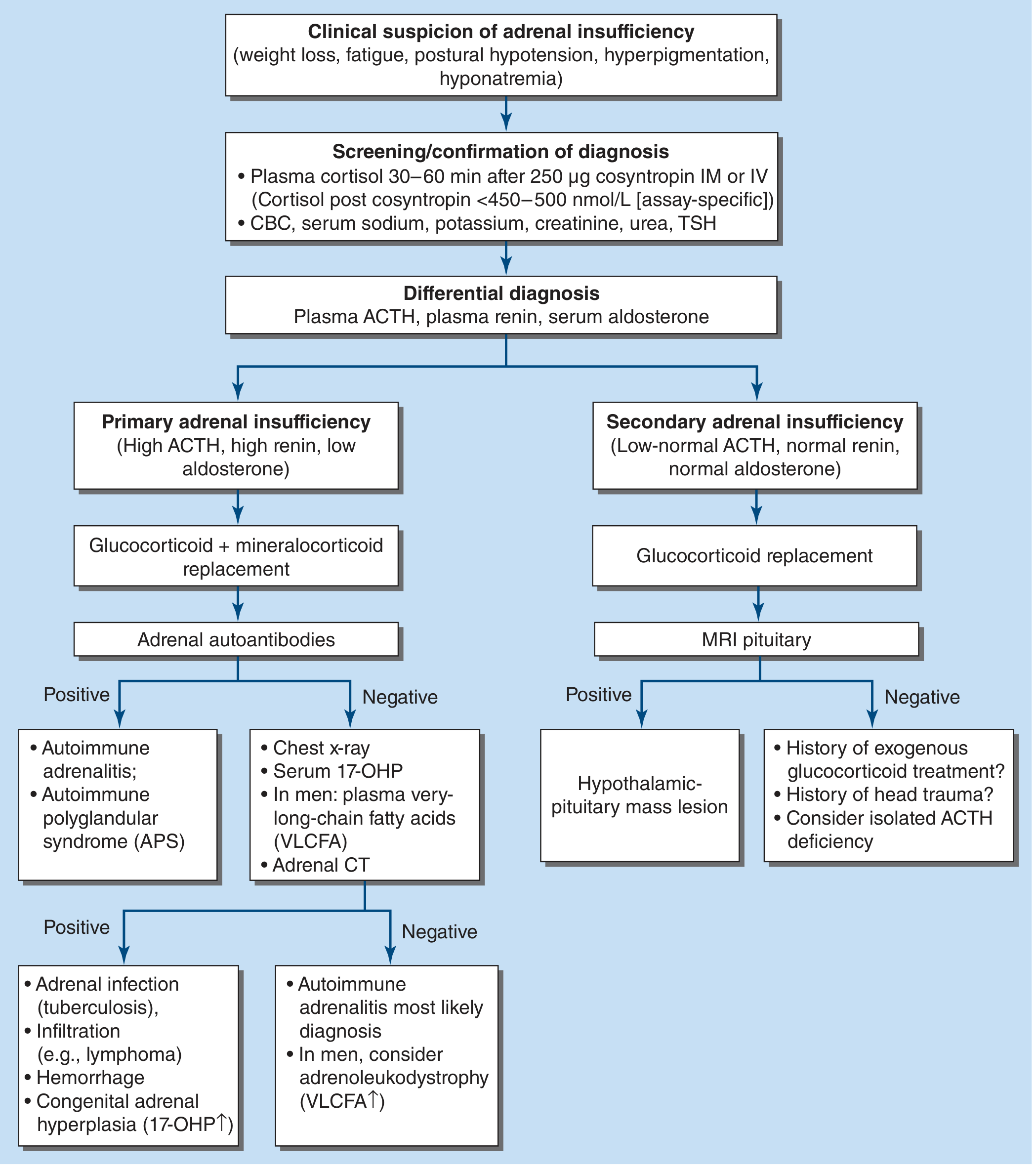
Your lab pattern - low serum cortisol + low/inappropriately low ACTH - points to secondary adrenal insufficiency (pituitary or hypothalamic origin), NOT primary (Addison's). This distinction is critical for treatment because:
- Primary AI (Addison's): ACTH is HIGH (adrenal gland fails, pituitary overdrives ACTH), low cortisol AND low aldosterone - needs both glucocorticoid + mineralocorticoid replacement
- Secondary AI: ACTH is LOW (pituitary/hypothalamic failure), low cortisol, but aldosterone is usually NORMAL - needs glucocorticoid only (mineralocorticoid axis is preserved)
The flowchart from Harrison's (2025) illustrates this:
Symptoms of Glucocorticoid Deficiency (your patient's picture)
From Harrison's Principles of Internal Medicine 22E:
| Symptom | Mechanism |
|---|---|
| Fatigue, severe tiredness | Glucocorticoid deficiency |
| Weight loss, anorexia | Glucocorticoid deficiency |
| Myalgia, joint pain | Glucocorticoid deficiency |
| Low BP, postural hypotension | Glucocorticoid deficiency |
| Hyponatremia | Loss of feedback inhibition of ADH |
| Hypoglycemia | Glucocorticoid deficiency |
| Pale/alabaster skin (NOT hyperpigmentation) | Deficiency of POMC peptides (secondary only) |
Treatment
ACUTE / Emergency (Adrenal Crisis)
If the patient is acutely unwell, hypotensive, or vomiting - treat immediately, do not wait for labs.
| Drug | Dose | Route | Notes |
|---|---|---|---|
| Hydrocortisone | 100 mg IV bolus immediately | IV | First-line; preferred over dexamethasone if cortisol assay not pending |
| Dexamethasone | 4 mg IV bolus | IV | Alternative if you still need cortisol assay (doesn't interfere with assay) |
| Then: Hydrocortisone | 200 mg/24 hours as 50 mg every 6 hrs IV | IV infusion or bolus | Continue until patient stabilises |
| IV fluids | 0.9% Normal Saline 2-3 L in first few hours | IV | Switch to D5/NS if hypoglycaemic |
- Rosen's Emergency Medicine; Harrison's Principles of Internal Medicine 22E
CHRONIC / Maintenance Replacement
1. Glucocorticoid (ALWAYS needed in both primary and secondary AI)
Hydrocortisone is the preferred replacement because it is bioidentical to cortisol.
| Regimen | Dose | Timing |
|---|---|---|
| Standard | 15-25 mg/day total, divided 2-3 doses | 2/3 in morning, 1/3 in late afternoon (mimics diurnal rhythm) |
| Common split | 10 mg on waking + 5 mg early afternoon | |
| Alternatively | Hydrocortisone 20 mg morning + 10 mg afternoon (older "30 mg" regimen) | Some centres still use this |
- Rosen's Emergency Medicine, Box 117.11; Goodman & Gilman's 13E
Other options (less preferred for chronic replacement):
- Prednisolone 5-7.5 mg/day (once daily morning)
- Dexamethasone 0.5-0.75 mg/day (no mineralocorticoid activity - see below)
2. Fludrocortisone (Mineralocorticoid) - FOR PRIMARY AI ONLY
In secondary AI (low ACTH), fludrocortisone is usually NOT needed because the aldosterone axis (renin-angiotensin) is intact.
However, if the patient has primary adrenal insufficiency (confirmed high ACTH, high renin, low aldosterone), fludrocortisone is essential:
| Setting | Fludrocortisone Dose |
|---|---|
| Standard maintenance | 50-100 mcg once daily (morning) |
| Harrison's initiation dose | 100-150 mcg/day |
| Rosen's range | 50-200 mcg/day |
| Minor illness / fever | Increase to 50-200 mcg/day |
| Hot climate / summer | Increase by 50-100 mcg |
| Maximum | 200 mcg/day |
Monitor fludrocortisone adequacy by:
- Blood pressure (sitting and standing - check for postural drop)
- Serum sodium and potassium
- Plasma renin (keep in upper-normal range)
Note: 40 mg of hydrocortisone is equivalent in mineralocorticoid effect to 100 mcg of fludrocortisone. Prednisone and prednisolone have reduced mineralocorticoid activity; dexamethasone has NONE - so if dexamethasone is used as glucocorticoid, fludrocortisone must still be given in primary AI.
- Harrison's Principles of Internal Medicine 22E; Goodman & Gilman's Pharmacological Basis of Therapeutics
3. Sick Day Rules (Stress Dosing)
| Situation | Action |
|---|---|
| Fever, minor illness | Double the daily hydrocortisone dose |
| Vomiting (can't take oral) | Hydrocortisone 100 mg IM/IV immediately |
| Major surgery / trauma | Hydrocortisone 100 mg IV before procedure, then 200 mg/24h infusion |
| Prolonged stress | Continue IV hydrocortisone 200 mg/24h until stable |
Patients should carry a hydrocortisone self-injection emergency kit and a steroid emergency card at all times.
Summary: Your Patient's Likely Regimen
| Diagnosis | Glucocorticoid | Fludrocortisone |
|---|---|---|
| Secondary AI (low ACTH, low cortisol) | Hydrocortisone 15-25 mg/day in 2-3 divided doses | Not needed (unless BP/electrolyte monitoring shows mineralocorticoid deficiency) |
| Primary AI (would show high ACTH) | Hydrocortisone 15-25 mg/day | Fludrocortisone 50-150 mcg once daily |
Since your picture shows low ACTH, investigate the pituitary (MRI pituitary) and consider whether this is from exogenous steroid use, a pituitary lesion, or isolated ACTH deficiency.
Important clinical note: Treatment should never wait for confirmatory testing if adrenal crisis is suspected. Draw cortisol/ACTH, then give hydrocortisone immediately.
This is a shared conversation. Sign in to Orris to start your own chat.