Essay answer for "Coagulation Pathway ? " Elaborate with Text book images & Flowcharts/Tables.
coagulation pathway intrinsic extrinsic common pathway clotting factors
coagulation cascade fibrin clot formation thrombin prothrombin
coagulation pathway cascade flowchart intrinsic extrinsic common
coagulation factors roles functions hemostasis secondary
clotting factors coagulation table roman numerals function
🩸 Coagulation Pathway — A Comprehensive Essay
1. Introduction
- Primary hemostasis — platelet plug formation (rapid but fragile)
- Secondary hemostasis — the coagulation cascade, which reinforces the platelet plug with a stable fibrin mesh
"The coagulation cascade is primarily initiated by vascular injury exposing tissue factor to blood components." — Harrison's Principles of Internal Medicine, 21st Edition (p. 3505)
2. Coagulation Factors — Overview Table
- Factor III (Tissue Factor) — subendothelial cells, monocytes
- Factor IV (Ca²⁺) — not a protein
- vWF — endothelium and megakaryocytes
| Factor | Name | Pathway | Nature | Vitamin K Dependent? |
|---|---|---|---|---|
| I | Fibrinogen | Common | Glycoprotein | No |
| II | Prothrombin | Common | Serine protease zymogen | ✅ Yes |
| III | Tissue Factor (TF) | Extrinsic | Glycoprotein (cofactor) | No |
| IV | Calcium (Ca²⁺) | All | Ion | No |
| V | Labile factor / Proaccelerin | Common | Cofactor | No |
| VII | Proconvertin | Extrinsic | Serine protease | ✅ Yes |
| VIII | Antihemophilic Factor A | Intrinsic | Cofactor | No |
| IX | Christmas Factor | Intrinsic | Serine protease | ✅ Yes |
| X | Stuart-Prower Factor | Common | Serine protease | ✅ Yes |
| XI | Plasma Thromboplastin Antecedent | Intrinsic | Serine protease | No |
| XII | Hageman Factor | Intrinsic (Contact) | Serine protease | No |
| XIII | Fibrin Stabilizing Factor | Common | Transglutaminase | No |
| — | Prekallikrein (PK) | Contact | Serine protease | No |
| — | HMWK | Contact | Cofactor | No |
Mnemonic for Vitamin K-dependent factors: "1972" → Factors II, VII, IX, X + Protein C & S
3. The Three Pathways
INTRINSIC PATHWAY EXTRINSIC PATHWAY
(Contact Activation) (Tissue Factor Pathway)
| |
| |
└────────────┬──────────────┘
▼
COMMON PATHWAY
|
▼
FIBRIN CLOT
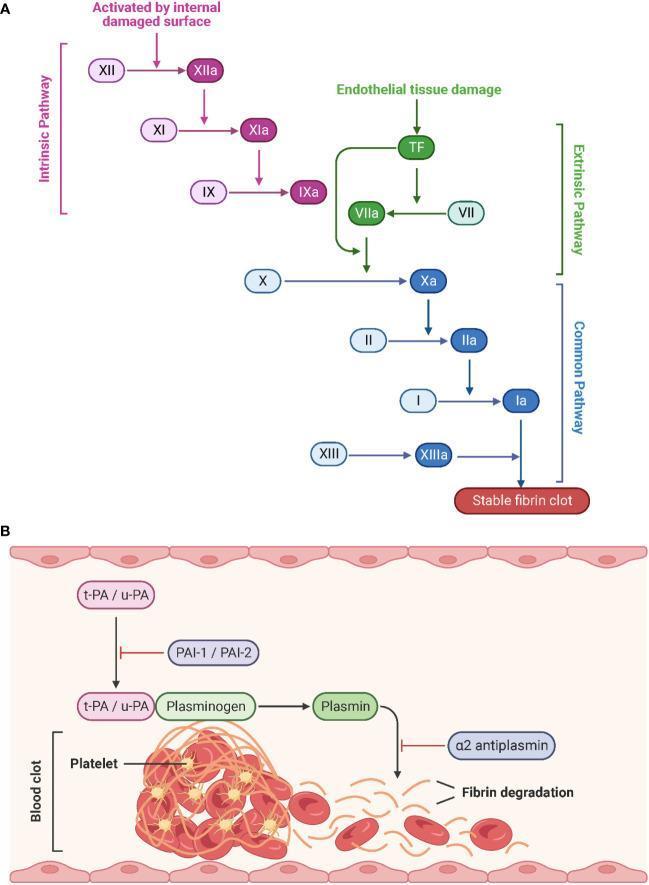
4. Extrinsic Pathway (Tissue Factor Pathway)
Step-by-Step:
Vascular Injury
↓
Tissue Factor (TF) Exposed
↓
TF + Factor VII → TF-VIIa Complex
↓
TF-VIIa activates:
├── Factor X → Xa (direct)
└── Factor IX → IXa (amplification loop)
↓
Factor Xa → enters Common Pathway
"Plasma factor VII is the ligand for and is activated by binding to tissue factor exposed at the site of vessel damage. The binding of FVII/VIIa to tissue factor activates the downstream conversion of factor X to active FX (FXa)." — Harrison's, 21st Ed. (p. 3505)
- This pathway is rapid but quickly inhibited by TFPI (Tissue Factor Pathway Inhibitor)
- Assessed by the Prothrombin Time (PT / INR)
5. Intrinsic Pathway (Contact Activation Pathway)
Step-by-Step:
Damaged Surface / Collagen
↓
Factor XII → XIIa (+ HMWK + Prekallikrein)
↓
Factor XI → XIa
↓
Factor IX → IXa
↓
IXa + VIIIa + Ca²⁺ + PL → Tenase Complex
↓
Factor X → Xa → enters Common Pathway
"The intrinsic pathway begins with the contact phase involving PK (prekallikrein), HMWK (high-molecular-weight kininogen), and FXIIa." — Harrison's, 21st Ed. (p. 3460)
- Deficiency of Factor VIII → Hemophilia A
- Deficiency of Factor IX → Hemophilia B (Christmas disease)
- Assessed by aPTT (Activated Partial Thromboplastin Time)
6. Common Pathway
Step-by-Step:
Factor Xa
↓
Xa + Va + Ca²⁺ + PL → Prothrombinase Complex
↓
Prothrombin (II) → Thrombin (IIa)
↓
Thrombin acts on:
├── Fibrinogen (I) → Fibrin monomers
├── Factor XIII → XIIIa (cross-linking)
├── Factors V, VIII (positive feedback)
└── Platelets (activation)
↓
Fibrin monomers → Polymerize → Soft clot
↓
XIIIa cross-links fibrin → STABLE CLOT
"Factor Xa with its cofactor FVa converts prothrombin to thrombin, which then converts soluble plasma fibrinogen to insoluble fibrin, leading to clot or thrombus formation. Thrombin also activates FXIII to FXIIIa, a transglutaminase that covalently cross-links and stabilizes the fibrin clot." — Harrison's, 21st Ed. (p. 3505)
7. Complete Coagulation Cascade — Visual Flowchart
8. Harrison's Coagulation Cascade with Lab Tests
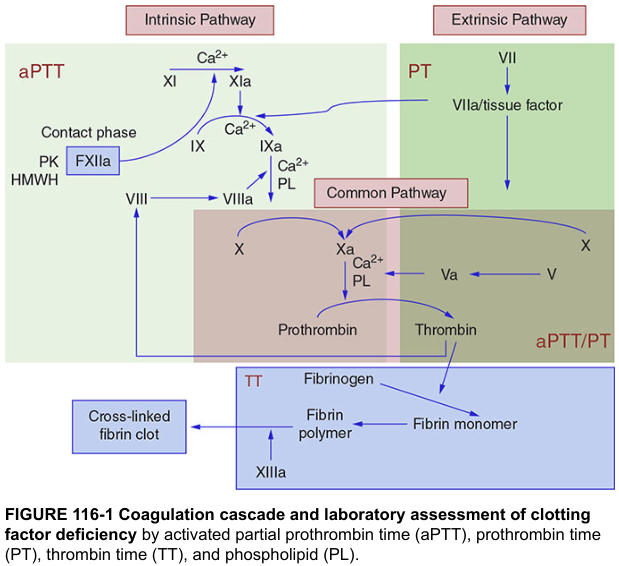
9. Laboratory Tests Correlated to Pathways
| Test | Full Name | Pathway Tested | Normal Range | Prolonged In |
|---|---|---|---|---|
| PT | Prothrombin Time | Extrinsic + Common (VII, X, V, II, I) | 11–13 sec | Warfarin, Liver disease, Factor VII deficiency |
| INR | International Normalized Ratio | Extrinsic + Common | 0.8–1.2 | Same as PT |
| aPTT | Activated Partial Thromboplastin Time | Intrinsic + Common (XII, XI, IX, VIII, X, V, II, I) | 25–35 sec | Heparin, Hemophilia A & B, vWD |
| TT | Thrombin Time | Final step: Fibrinogen → Fibrin | 14–19 sec | Hypofibrinogenemia, Heparin, Dabigatran |
| Fibrinogen | Clauss method | Final substrate | 200–400 mg/dL | DIC, Liver failure |
10. Key Enzyme Complexes Summary
| Complex | Components | Reaction Catalyzed |
|---|---|---|
| Extrinsic Tenase | TF + VIIa + Ca²⁺ | IX → IXa; X → Xa |
| Intrinsic Tenase | IXa + VIIIa + Ca²⁺ + PL | X → Xa |
| Prothrombinase | Xa + Va + Ca²⁺ + PL | Prothrombin → Thrombin |
11. Thrombin — The Central Molecule
THROMBIN (IIa)
│
┌─────────────┼─────────────────┐
▼ ▼ ▼
Fibrinogen → Fibrin XIII → XIIIa V, VIII activation
▼ ▼ ▼
Clot formation Clot Amplification
stabilization loop
▼
Platelets → activation
Protein C → anticoagulation (via thrombomodulin)
- Converts fibrinogen → fibrin
- Activates Factor XIII (fibrin cross-linking)
- Activates Factors V and VIII (amplification)
- Activates platelets
- Binds thrombomodulin on endothelium → activates Protein C → inactivates Va and VIIIa
12. Natural Anticoagulant Mechanisms
| Inhibitor | Mechanism | Factors Inhibited |
|---|---|---|
| Antithrombin III (AT-III) | Serine protease inhibitor (heparin cofactor) | Thrombin (IIa), Xa, IXa, XIa, XIIa |
| Protein C + S | Vitamin K–dependent; activated by Thrombin-Thrombomodulin | Va, VIIIa |
| TFPI | Tissue Factor Pathway Inhibitor | TF-VIIa-Xa complex |
| Prostacyclin (PGI₂) | From endothelium | Inhibits platelet aggregation |
13. Fibrinolysis (Clot Dissolution)
tPA / uPA (from endothelium)
↓
Plasminogen → PLASMIN
↓
Fibrin clot → Fibrin Degradation Products (FDPs)
↓
D-Dimers (cross-linked fibrin fragments)
"During fibrinolysis, plasminogen is converted into plasmin, which degrades the fibrin network." — Bailey & Love's Short Practice of Surgery, 28th Ed. (p. 47)
- PAI-1, PAI-2 — inhibit tPA and uPA
- α₂-antiplasmin — directly inhibits plasmin
14. Clinical Correlations
| Condition | Defect | Key Feature |
|---|---|---|
| Hemophilia A | Factor VIII deficiency | ↑ aPTT, normal PT; hemarthroses |
| Hemophilia B | Factor IX deficiency | ↑ aPTT, normal PT |
| Von Willebrand Disease | vWF deficiency/dysfunction | ↑ aPTT (VIII carrier), ↑ BT |
| DIC | Consumption of all factors | ↑ PT, ↑ aPTT, ↑ D-dimer, ↓ fibrinogen |
| Warfarin | Inhibits Vit K–dependent factors (II, VII, IX, X) | ↑ PT (VII shortest t½ → first prolonged) |
| Heparin | Potentiates AT-III | ↑ aPTT |
| Liver disease | Decreased factor synthesis | ↑ PT > ↑ aPTT |
| Factor V Leiden | Resistance to Protein C | Thrombophilia/DVT |
15. Summary Flowchart — Full Coagulation Pathway
INTRINSIC PATHWAY EXTRINSIC PATHWAY
(Contact Activation) (Tissue Factor)
───────────────────── ──────────────────
Damaged surface Vascular injury
↓ ↓
XII → XIIa TF exposed
(+HMWK, PK) ↓
↓ VII + TF → VIIa-TF
XI → XIa ↓
↓ ┌── X → Xa
IX → IXa └── IX → IXa
↓
IXa + VIIIa + Ca²⁺ + PL
(Intrinsic Tenase Complex)
↓
X → Xa ←─────────────────── (from both pathways)
\
\
COMMON PATHWAY
───────────────
Xa + Va + Ca²⁺ + PL
(Prothrombinase Complex)
↓
Prothrombin (II) → Thrombin (IIa)
↓
Fibrinogen (I) → Fibrin monomers
↓
+ Factor XIIIa (cross-linking)
↓
████ STABLE FIBRIN CLOT ████
16. Key Points to Remember (Exam Focus)
- Extrinsic pathway = TF + VII → measured by PT/INR
- Intrinsic pathway = Contact (XII, XI, IX, VIII) → measured by aPTT
- Common pathway = X → V → Prothrombin → Thrombin → Fibrin
- Vitamin K–dependent factors: II, VII, IX, X, Protein C & S
- Thrombin is the master enzyme — converts fibrinogen to fibrin AND activates XIII, V, VIII
- Prothrombinase complex: Xa + Va + Ca²⁺ + PL
- Intrinsic Tenase complex: IXa + VIIIa + Ca²⁺ + PL
- TFPI inhibits the extrinsic tenase complex (TF-VIIa-Xa)
- Antithrombin III is potentiated by heparin
- D-dimers = products of cross-linked fibrin degradation (marker of fibrinolysis/DIC)
I am a Post graduate/Junior residency student in Otorhinolaryngology preparing for University exams. Give an elaborated essay answer for a question "Physiology of Balance ?" Under 2000 words, also provide relevant & standard images/diagrams, flowcharts/tables. Take direct excerpts from standard books 1. Cummings Otorhinolaryngology, Head & Neck Surgery 7th Edition - Volume 3, section 7 2. Scott Brown's textbook of Otorhinolaryngology - 8th edition.
physiology of balance vestibular system semicircular canals otolith organs
vestibulo-ocular reflex VOR vestibulospinal reflex balance central processing
vestibular system anatomy semicircular canals utricle saccule diagram
hair cell vestibular transduction cupula endolymph kinocilium stereocilia depolarization
vestibular hair cell cupula crista ampullaris endolymph deflection
otolith organ macula utricle saccule linear acceleration gravity
vestibulo-ocular reflex VOR pathways brainstem cerebellum diagram
Physiology of Balance
Introduction
- Vestibular system (dominant)
- Visual system
- Proprioceptive system (somatosensory)
"Spatial orientation and balance result from the integration of vestibular, visual, and somatosensory inputs in the brainstem and cerebellum, culminating in coordinated motor responses." — Cummings Otolaryngology, Head & Neck Surgery, 7th Ed.
The Three Sensory Components of Balance
| Sensory Input | Detects | Pathway |
|---|---|---|
| Vestibular | Angular & linear acceleration, gravity | CN VIII → brainstem |
| Visual | Visual field motion, horizon | CN II → visual cortex → brainstem |
| Proprioception | Joint position, pressure, muscle stretch | Spinal cord → brainstem/cerebellum |
The Romberg test exploits this triad: removing vision (eyes closed) unmasks vestibular/proprioceptive deficiency.
I. The Vestibular System — Peripheral Apparatus
Anatomy of the Labyrinth
- 3 Semicircular Canals (SCCs): Lateral (horizontal), Anterior (superior), Posterior
- 2 Otolith Organs: Utricle and Saccule
| Structure | Detects | Stimulus |
|---|---|---|
| Semicircular canals | Angular acceleration (rotation) | Endolymph deflection of cupula |
| Utricle | Linear acceleration (horizontal) + head tilt | Otoconia shear on macula |
| Saccule | Linear acceleration (vertical) | Otoconia shear on macula |
"The three semicircular canals are arranged in the three planes of space at right angles to each other. In the lateral canals, the hair cells are embedded in a gelatinous cupula. Shearing forces, caused by angular movements of the head, produce hair cell movements and generate action potentials. In the utricle and saccule, the hair cells are embedded in an otoconial membrane, which contains particles of calcium carbonate. These respond to changes in linear acceleration and the pull of gravity." — Bailey & Love's Short Practice of Surgery, 28th Ed. (p. 773)
II. Sensory Transduction — The Hair Cell
Structure:
- Each hair cell bears 1 kinocilium (tallest) and 40–70 stereocilia (graded height)
- Stereocilia are connected by tip links (fine filaments)
- Arranged in a polarized bundle — the morphological polarization axis
Mechanism of Transduction:
HEAD MOVEMENT
↓
Endolymph / Otoconia moves
↓
Stereocilia deflect
↓
┌─────────────────────────────────────────────┐
│ Toward kinocilium │ Away from kinocilium │
│ → Tip links stretch │ → Tip links slacken │
│ → K⁺/Ca²⁺ channels │ → Channels close │
│ open │ │
│ → DEPOLARIZATION │ → HYPERPOLARIZATION │
│ → ↑ Firing rate │ → ↓ Firing rate │
└─────────────────────────────────────────────┘
↓
Glutamate release at afferent synapse
↓
Action potentials in vestibular nerve (CN VIII)
- Hair cell apex bathed in endolymph (high K⁺, low Na⁺) — like intracellular fluid
- Cell body bathed in perilymph (high Na⁺, low K⁺)
- Resting endocochlear potential ≈ +80 mV (produced by stria vascularis/dark cells)
- K⁺ flows into hair cell through mechanosensitive channels → depolarization
The resting tonic firing rate (~80–100 spikes/second) of vestibular afferents allows the system to signal both excitation (increased rate) and inhibition (decreased rate) — bidirectional signaling critical for detecting motion in both directions.
III. Semicircular Canals — Detection of Angular Acceleration
The Crista Ampullaris
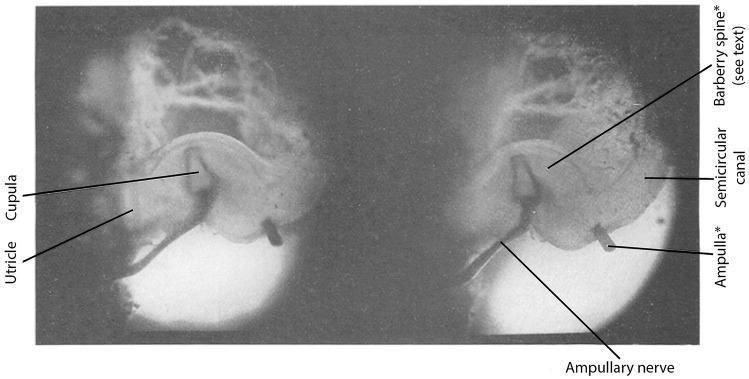
How Angular Acceleration is Detected:
HEAD ROTATION (e.g., turning left)
↓
Bony canal moves WITH head
↓
Endolymph lags behind (inertia)
↓
Relative endolymph flow OPPOSITE to head rotation
↓
Cupula deflects
↓
Hair cell stereocilia bend
↓
LEFT canal: toward kinocilium → DEPOLARIZATION → ↑ firing
RIGHT canal: away from kinocilium → HYPERPOLARIZATION → ↓ firing
Canal Pairing (Coplanar Pairs):
| Pair | Canals | Function |
|---|---|---|
| 1 | Left Lateral + Right Lateral | Yaw (horizontal rotation) |
| 2 | Left Anterior + Right Posterior | Roll (left) |
| 3 | Right Anterior + Left Posterior | Roll (right) |
Ewald's Laws:
Classically described by Ewald (1892) and remain foundational in vestibular physiology:
- Law I: Nystagmus and eye/body movement occur in the plane of the stimulated canal
- Law II (Horizontal canal): Endolymph flow toward the ampulla (ampullopetal) produces a stronger response than away from it (ampullofugal)
- Law III (Vertical canals): Ampullofugal flow produces the stronger response (opposite to horizontal)
IV. Otolith Organs — Detection of Linear Acceleration & Gravity
Structure of the Macula
- Hair cells embedded in a gelatinous otolithic membrane
- Overlying this membrane is a layer of otoconia (calcium carbonate crystals, CaCO₃)
- High density of otoconia (density ≈ 2.71 g/cm³ vs. endolymph 1.0 g/cm³) → inertia during linear movement
How Linear Acceleration / Gravity is Detected:
LINEAR HEAD MOVEMENT or TILT
↓
Otoconia slide on gelatinous membrane (due to gravity/inertia)
↓
Shear forces on hair cell stereocilia
↓
Deflection toward or away from kinocilium
↓
Depolarization or Hyperpolarization
↓
Signal via superior/inferior vestibular nerve
The Striola:
| Otolith | Plane | Detects |
|---|---|---|
| Utricle | Horizontal | Forward/backward & lateral linear acceleration; head tilt |
| Saccule | Vertical (sagittal) | Up/down linear acceleration; seismic vibration |
V. Central Vestibular Processing
Vestibular Nuclei Complex
| Nucleus | Key Projections |
|---|---|
| Superior (Bechterew) | MLF → oculomotor nuclei (VOR) |
| Medial (Schwalbe) | Bilateral MLF → neck/eye muscles; VSR |
| Lateral (Deiters) | Lateral vestibulospinal tract → postural muscles |
| Inferior (Spinal) | Cerebellum, reticular formation |
Role of the Cerebellum:
- Receives direct vestibular afferents (only cranial nerve with direct cerebellar input)
- Modulates and calibrates VOR gain
- Critical for adaptive plasticity of vestibular reflexes
VI. Motor Output — The Three Key Reflexes
1. Vestibulo-Ocular Reflex (VOR)
Head turns RIGHT
↓
Right horizontal canal excited (↑ firing)
Left horizontal canal inhibited (↓ firing)
↓
Via MLF → CN III, IV, VI nuclei
↓
Eyes deviate LEFT (compensatory)
↓
Visual image remains stable on fovea
"The most useful bedside test of peripheral vestibular function is the head impulse test, in which the vestibulo-ocular reflex is assessed with small-amplitude (~20 degrees) rapid head rotations. If the VOR is deficient, the rotation is followed by a catch-up saccade in the opposite direction." — Harrison's Principles of Internal Medicine, 21st Ed. (p. 721)
2. Vestibulospinal Reflex (VSR)
- Activates ipsilateral extensor muscles (anti-gravity)
- Inhibits ipsilateral flexors
- Maintains upright posture and prevents falls
- Example: When head tilts right → right leg extensors contract to correct balance
3. Vestibulocollic Reflex (VCR)
- Mediated via medial vestibulospinal tract → neck muscles
- Stabilizes the head relative to the body during postural perturbations
VII. Sensory Integration and Conflict
VESTIBULAR INPUT ──┐
├──► CNS Integration ──► MOTOR OUTPUT
VISUAL INPUT ──────┤ (Brainstem + (Eyes, Neck,
│ Cerebellum) Postural muscles)
PROPRIOCEPTION ────┘
According to Cummings ORL 7th Ed., when vestibular and visual inputs conflict (e.g., reading in a moving car), the CNS relies predominantly on vestibular information for spatial orientation, but persistent conflict leads to autonomic symptoms.
- Vestibular > Proprioceptive > Visual for low-frequency motion
- Visual dominates for slow, steady stimuli (vection)
VIII. Nystagmus — Physiological Expression of the VOR
Unilateral Vestibular Excitation
↓
Slow compensatory eye movement (toward opposite side) ← VOR drive
↓
Fast resetting saccade (toward excited side) ← Brainstem PPRF
↓
NYSTAGMUS: named after FAST phase
| Feature | Peripheral Nystagmus | Central Nystagmus |
|---|---|---|
| Direction | Unidirectional, horizontal-torsional | Direction-changing, purely vertical/torsional |
| Fixation | Suppressed by fixation | NOT suppressed |
| Latency (positional) | Present (3–10 sec) | Absent |
| Fatigability | Yes | No |
| Associated symptoms | Vertigo (intense) | Diplopia, dysarthria, ataxia |
IX. Summary Flowchart — Physiology of Balance
┌──────────────────────────────────────────────────────┐
│ PERIPHERAL VESTIBULAR INPUT │
│ │
│ SCCs (Angular accel.) + Otoliths (Linear accel.) │
│ ↓ Hair cell transduction ↓ │
│ Endolymph/Otoconia → Stereocilia deflection │
│ → K⁺ influx → Depolarization → Glutamate release │
│ ↓ Superior & Inferior Vestibular Nerve │
└──────────────────────────────────────────────────────┘
↓
┌──────────────────────────────────────────────────────┐
│ VESTIBULAR NUCLEI (Medulla/Pons) │
│ Superior │ Medial │ Lateral │ Inferior │
└──────────────────────────────────────────────────────┘
↓ ↓ ↓
┌──────────┐ ┌───────────┐ ┌──────────────┐
│ VOR │ │ VSR │ │ Cerebellum │
│ (CN III, │ │(Postural │ │(Calibration/ │
│ IV, VI) │ │ muscles) │ │ Adaptation) │
└──────────┘ └───────────┘ └──────────────┘
↓ ↓
Gaze stability Balance &
(Nystagmus) Upright posture
Key Points to Remember (Exam Focus)
- Balance = Vestibular + Visual + Proprioceptive integration
- SCCs → angular acceleration → cupula/crista → hair cells → CN VIII
- Utricle → horizontal linear acceleration + head tilt; Saccule → vertical linear acceleration
- Hair cell depolarization: stereocilia deflect toward kinocilium → K⁺ in → depolarization
- Tonic resting discharge (~80–100 Hz) allows bidirectional modulation
- Ewald's Laws: response in plane of canal; ampullopetal > ampullofugal (horizontal canal)
- VOR (gain ≈ 1): head right → eyes left → image stabilized — tested by Head Impulse Test
- VSR: Deiters' nucleus → lateral VST → ipsilateral extensors → prevents falls
- Vestibulocerebellum (flocculonodular lobe) — calibrates VOR, adaptive plasticity
- Sensory conflict → motion sickness; vestibular input dominates for dynamic motion