24 yers female complaining of vulvar itching since 2 years especially in night time
vulvar pruritus young women etiology management
Vulvar Pruritus in a 24-Year-Old Female - Clinical Assessment
Why Does It Worsen at Night?
- Candidiasis - yeast activity increases in warm, occluded environment under clothing at night
- Pinworm (Enterobius vermicularis) - females migrate to perianal area at night to lay eggs, causing intense perianal and sometimes vulvar/vaginal pruritus - a classic clinical pattern especially in younger patients
- Scabies - classically nocturnal, caused by mite burrowing activity at night
- Lichen sclerosus - itching often worse at night due to warmth and reduced distraction
- Atopic/contact dermatitis - nocturnal flares common
Differential Diagnosis (Most to Least Common in This Age Group)
| Cause | Frequency | Key Features |
|---|---|---|
| Unspecified dermatitis (atopic/contact) | 54% | Most common overall; from pads, contraceptives, fragrance, condoms |
| Vulvovaginal candidiasis | ~10% | Thick curd-like discharge, erythema, burning + itch; worsened by antibiotics/OCP |
| Lichen sclerosus | 13% | White, thickened skin; intense pruritus; older women more affected but can occur at any age |
| Lichen simplex chronicus | Common | Lichenified skin from chronic scratching; perpetuating itch-scratch cycle |
| Dysesthetic vulvodynia | 9% | Burning > itching; sensory neuropathy component |
| Psoriasis | 5% | Look for well-defined red plaques; check for lesions elsewhere |
| Trichomonas vaginalis | Less common | Frothy, malodorous discharge; confirmed by wet prep |
| Pubic lice (Phthirus pubis) | Possible | Intense perianal/pubic itching especially at night; look for nits |
| Scabies | Possible | Nocturnal, track marks, involves other family members |
| Pinworm | Possible | Perianal >> vulvar; nocturnal |
| Bacterial vaginosis | Uncommon as sole cause | Fishy odor, thin discharge, irritation |
- Berek & Novak's Gynecology, p. 467-469
- Andrews' Diseases of the Skin, p. 2589
History to Elicit
- Discharge - color, consistency, odor? (Candida = white curd; BV = fishy; Trichomonas = frothy yellow-green)
- Recent antibiotic or OCP use? (predisposes to candidiasis)
- Contact exposure - new soaps, sanitary pads, wipes, fabric softeners, condom brands?
- Sexual history - new partner, STI exposure, partner symptoms?
- Perianal involvement? (suggests pinworm/scabies)
- Other family members affected? (suggests scabies/pinworm)
- Skin elsewhere - eczema history, psoriasis plaques?
- Diabetes or immunosuppression? (recurrent candidiasis)
- Prior treatments tried? (self-medication with antifungals is very common but often incorrect)
- Urinary incontinence? (chronic moisture = irritant vulvitis)
Examination
- Inspect skin for: erythema, white plaques (candida), white thickened skin (lichen sclerosus), lichenification (lichen simplex), excoriations, burrows (scabies), nits
- Vaginal discharge: color, pH, KOH/wet mount
- Perianal area: look for worms at night or adhesive tape test (pinworm)
- Inguinal lymphadenopathy
Investigations
| Test | Detects |
|---|---|
| Wet mount (saline + KOH) | Candida (hyphae/pseudohyphae), Trichomonas |
| Vaginal pH | >4.5 = BV/Trichomonas; <4.5 = Candida/normal |
| Vaginal culture | Recurrent candidiasis (non-albicans species) |
| STI screen (NAAT) | Chlamydia, Gonorrhea, Trichomonas |
| Adhesive tape test (morning) | Pinworm eggs |
| Fasting blood glucose / HbA1c | Diabetes (underlying cause of recurrent candidiasis) |
| Biopsy | If lesion is atypical, persistent, or not responding to treatment - mandatory to rule out VIN or malignancy |
| Patch testing | If contact dermatitis suspected |
Management Principles
- Topical azole (clotrimazole, miconazole) or oral fluconazole 150 mg single dose
- Recurrent (≥4 episodes/year): fluconazole weekly maintenance x 6 months
- Miconazole: mycological cure ~80-95% at 1 month; pruritus can be relieved after a single application
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 3298-3305
- Identify and eliminate trigger (pads, wipes, soaps, condoms)
- Mild-moderate topical steroid (e.g., hydrocortisone 1%)
- Fragrance-free emollients; silk/cotton underwear
- High-potency topical corticosteroid (e.g., clobetasol 0.05%) in pulsed dosing - first-line
- Topical tacrolimus or pimecrolimus as steroid-sparing alternatives
- Long-term follow-up needed (increased risk of vulvar squamous cell carcinoma)
- Break the itch-scratch cycle with topical steroids ± sedating antihistamine at night
- Phototherapy (comb light device) may be effective
- Mebendazole 100 mg single dose, repeated after 2 weeks (treat household contacts)
- Permethrin 5% cream applied overnight; treat all close contacts
- Avoid soap directly on vulva; use plain water or soap-free wash
- Loose cotton underwear
- Avoid irritants (perfumed pads, douches, wet wipes with preservatives)
- Topical lidocaine or pramoxine for symptomatic relief
- Oral TCA (amitriptyline) for neuropathic/dysesthetic component
Red Flags Requiring Biopsy
- Persistent skin changes not responding to 6-8 weeks of appropriate treatment
- White, thickened lesions (lichen sclerosus - needs monitoring for malignant transformation)
- Any atypical pigmented lesion (rule out VIN, melanoma)
- Age >40 with unexplained persistent vulvar symptoms
Search for clinical images of candidiasis vs lichen sclerosus for comparison
Vulvar Candidiasis vs. Lichen Sclerosus - Clinical Image Comparison
🔴 CANDIDAL VULVITIS


- Diffuse erythema (beefy red color) of the labia and surrounding skin
- White, curdy plaques or discharge adherent to the mucosa
- Satellite lesions - small erythematous papules/pustules at the periphery (pathognomonic)
- Excoriations from intense scratching
- Skin texture is inflamed but normal anatomical architecture is preserved
- Involvement may extend to inguinal folds and perianal area
⚪ LICHEN SCLEROSUS
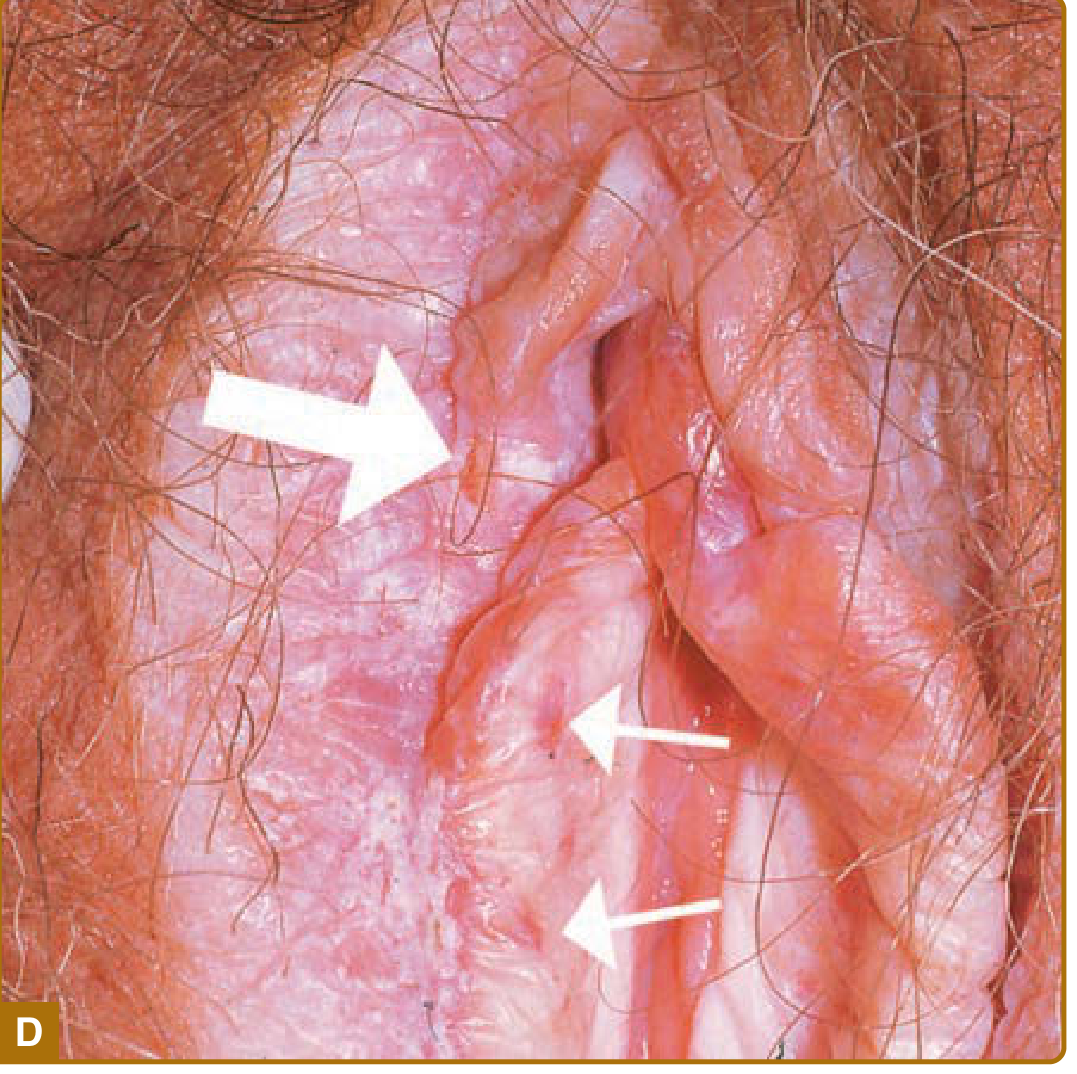
White vulvar plaque with waxy/crinkled texture, purpura (small arrows), and erosions (large arrow) - these features together are diagnostic of lichen sclerosus.
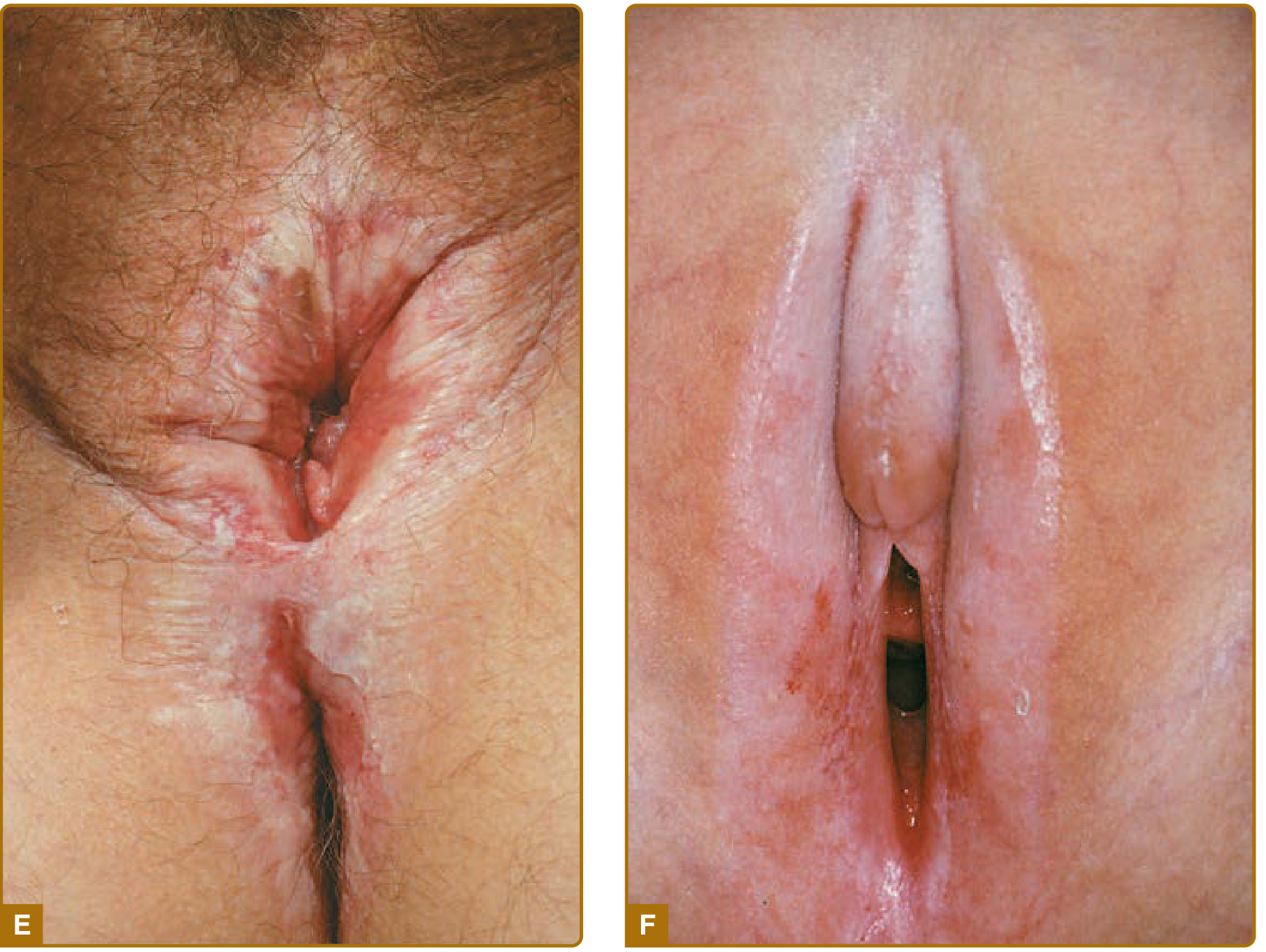
Left (E): Sclerotic vulva with disappearance of the labia minora, shrinkage of the introitus, erythema and erosions in a classic figure-8 pattern extending to the anus - severe pruritus and dyspareunia. Right (F): Lichen sclerosus in an 8-year-old girl showing the typical pale, smooth appearance.
- Porcelain-white atrophic plaques, waxy and crinkled ("cigarette paper" texture)
- Loss of anatomical landmarks - labia minora may disappear, clitoral hood may fuse
- Figure-8 pattern extending from vulva to anus (classic distribution)
- Purpura, fissures, and erosions from minor trauma/scratching
- Scarring and stenosis of the introitus in advanced disease
- Normal architecture is destroyed (key distinction from candidiasis)
🔬 Side-by-Side Comparison Table
| Feature | Candidiasis | Lichen Sclerosus |
|---|---|---|
| Color | Beefy red + white plaques | Porcelain white/pale |
| Texture | Moist, erythematous | Atrophic, waxy, crinkled |
| Architecture | Preserved | Progressively destroyed |
| Satellite lesions | Yes (pathognomonic) | No |
| Distribution | Mucosal + skin folds | Labia + perineum, figure-8 |
| Discharge | Yes - white, curd-like | None |
| Fissures | Occasional | Common |
| Associated discharge | Yes | No |
| KOH prep | Hyphae/pseudohyphae | Negative |
| Vaginal pH | <4.5 | Normal (not vaginal) |
| Age peak | Reproductive age | Postmenopausal / prepubertal |
| Cancer risk | No | Yes - SCC vulva (36x increased) |
| Treatment | Antifungal (fluconazole/azole) | Clobetasol 0.05% (high-potency steroid) |
Also Shown - Lichen Simplex Chronicus (for completeness):

Find latest guidelines for managing chronic vulvar pruritus
chronic vulvar pruritus management guidelines
chronic vulvar pruritus management guidelines 2024 2025 ISSVD ACOG
PMID: 40131720
lichen sclerosus vulva treatment guideline 2024
vulvovaginal candidiasis recurrent treatment guideline
ISSVD guidelines vulvar disease 2024 2025 pruritus diagnosis treatment
PMID: 39837649
PMID: 39956121
https://www.issvd.org/application/files/4916/7897/2719/ISSVD…
lichen sclerosus vulva clobetasol calcineurin inhibitor treatment
Latest Guidelines: Managing Chronic Vulvar Pruritus (2024-2025)
Key Guideline Sources
| Guideline | Year | Body | Scope |
|---|---|---|---|
| BASHH UK National Guideline on Vulval Conditions | 2025 (published Apr) | British Association for Sexual Health and HIV | Lichen sclerosus, lichen planus, eczema, lichen simplex, psoriasis, VIN, vulval pain |
| ISSVD Recommendations for Diagnosis & Treatment of Vaginitis | 2024 | International Society for Study of Vulvovaginal Disease | BV, candidiasis, Trichomonas, atrophic vaginitis, desquamative vaginitis |
| ECMM/ISHAM/ASM Global Candidiasis Guideline | 2025 | European/International mycology societies | Vulvovaginal + invasive candidiasis, antifungal resistance |
| 2025 Comprehensive Review - Am J Clin Dermatol (PMID: 40131720) | 2025 | Mashoudy et al. | Full spectrum of vulvovaginal itching - infections to neuropathic |
Step 1 - Accurate Diagnosis First (All Guidelines Agree)
- Vaginal pH + wet mount (saline + KOH)
- STI NAAT (Chlamydia, GC, Trichomonas)
- Fungal culture if candidiasis suspected but not confirmed on microscopy
- Biopsy - mandatory for any persistent/atypical lesion, white changes, or failure to respond to 6-8 weeks of appropriate therapy
- Patch testing if contact dermatitis suspected
- Blood glucose/HbA1c in recurrent candidiasis
Step 2 - Stepwise Management by Cause
A. Vulvovaginal Candidiasis (ISSVD 2024 + ECMM 2025 Global Guideline)
- Oral fluconazole 150 mg single dose OR topical azole (clotrimazole 1% cream, miconazole) x 7 days
- Both equally effective; oral preferred for compliance
- Induction: fluconazole 150 mg every 72 hours x 3 doses
- Maintenance: fluconazole 150 mg weekly x 6 months (reduces recurrence by ~50%)
- For non-albicans species (e.g., C. glabrata): boric acid 600 mg vaginal suppository x 14 days
- ECMM 2025 notes rising fluconazole-resistant C. parapsilosis and C. auris - culture and sensitivity testing recommended when treatment fails
B. Lichen Sclerosus (BASHH 2025 + ISSVD Practical Guide)
- Clobetasol propionate 0.05% (ultra-high potency) ointment - apply once nightly x 4 weeks, then on alternate nights x 4 weeks, then twice weekly x 4 weeks (the "3-month reducing course")
- BASHH 2025 confirms ~96% response rate with this regimen
- Repeat course if relapse
- Long-term, low-dose topical steroid 1-2x/week to prevent relapse and reduce SCC risk
- Regular follow-up every 6-12 months lifelong (cancer surveillance)
- Tacrolimus 0.1% or pimecrolimus 1% ointment - calcineurin inhibitors; use with caution long-term (FDA black box warning for theoretical malignancy risk)
- Acitretin (oral retinoid) for severe refractory cases
C. Lichen Planus / Lichen Simplex Chronicus (BASHH 2025)
- High-potency topical steroids (clobetasol) - first-line
- For erosive LP: intravaginal hydrocortisone 25 mg suppositories
- Tacrolimus, hydroxychloroquine, or systemic immunosuppressants for refractory cases
- Break the cycle: moderate-potency topical steroid + sedating antihistamine at night (hydroxyzine 10-25 mg)
- Emollients and barrier protection
- Treat any underlying cause (atopy, contact allergen)
D. Contact/Irritant Dermatitis (BASHH 2025)
- Identify and remove trigger (patch testing for allergic; common culprits: pads, wipes, fragrance, benzocaine)
- Mild-moderate topical steroid (hydrocortisone 1-2.5%)
- Soap substitutes, emollients (fragrance-free)
- Cotton underwear; avoid tight clothing
E. Vulvodynia / Neuropathic Component (BASHH 2025)
- Topical lidocaine 2-5% ointment/gel for symptom control
- Oral amitriptyline 10-25 mg nocte (titrate up) - first-line systemic
- Gabapentin 300 mg TDS (off-label)
- Pelvic floor physiotherapy
- Psychological interventions (CBT)
- Botulinum toxin injection for provoked vestibulodynia
Step 3 - General Measures (All Guidelines)
| Measure | Rationale |
|---|---|
| Soap-free vulvar washing (plain water) | Reduces irritant dermatitis |
| Fragrance-free emollient (e.g., white soft paraffin) | Restores skin barrier |
| Cotton underwear; avoid tight synthetic clothes | Reduces moisture and friction |
| Avoid sanitary pads with plastics/fragrance | Common contact allergen source |
| Avoid douching | Disrupts vaginal flora |
| Sitz baths (plain warm water) | Soothes and cleanses |
| Treat partner if Trichomonas or recurrent candidiasis | Reduces re-infection |
Step 4 - When to Refer / Biopsy
- Persistent lesion not responding to 6-8 weeks of appropriate treatment
- Any white, pigmented, or ulcerated lesion of uncertain diagnosis
- Suspected VIN (vulvar intraepithelial neoplasia)
- Complex/multifactorial vulvodynia requiring MDT (gynaecology, dermatology, pain medicine, psychology)
- All lichen sclerosus patients need annual review (SCC surveillance)
For Your 24-Year-Old Patient Specifically
- Do not empirically treat as candidiasis without confirming it - misdiagnosis rates are high (only 1/3 of self-diagnosed yeast infections are confirmed)
- Consider neuropathic/psychological components in chronic (>3 month) cases
- Multidisciplinary approach when single-cause treatment fails
- Significant gap remains in female-specific pruritus research and long-term quality-of-life data
Important note: The ECMM 2025 global candidiasis guideline carries an erratum (PMID: 41109319) - check the corrected version before applying specific drug dosing recommendations.
Can apply clotrimazole plus miconazole topically
Can Clotrimazole + Miconazole Be Applied Together Topically?
The Short Answer: No - do not combine them.
Why Not?
| Property | Clotrimazole | Miconazole |
|---|---|---|
| Class | Imidazole azole | Imidazole azole |
| Mechanism | Inhibits ergosterol synthesis (lanosterol 14α-demethylase) | Same - identical target |
| Spectrum | Candida spp., dermatophytes | Identical spectrum |
| Fungistatic/cidal | Primarily fungistatic | Primarily fungistatic |
| Efficacy (VVC) | >80% cure at 7-day regimen | ~80-95% cure at 1 month |
- No additive antifungal effect - you cannot double-inhibit the same target
- No synergy - synergy only occurs between drugs with different mechanisms (e.g., azole + echinocandin)
- No broader spectrum - both already cover C. albicans and dermatophytes equally
"All these compounds [clotrimazole, miconazole, econazole, butoconazole, tioconazole] seem to have comparable efficacy." - Jawetz Medical Microbiology, p. 269
What Combining Them DOES Cause
- Increased local irritation - adverse effects of topical azoles include burning, stinging, pruritus, erythema, and local irritation (Katzung's Basic & Clinical Pharmacology, p. 1208). Using two preparations doubles this risk
- Worsening the symptom you're treating - itching/burning from drug irritation mimics or worsens vulvar pruritus
- Potential competitive antagonism - two drugs competing for the same binding site may theoretically reduce the efficacy of each
- Maceration - applying multiple creams to the vulvar area occludes the skin and promotes moisture-related skin breakdown
The Correct Approach: Choose ONE
| Scenario | Recommended Single Agent |
|---|---|
| Patient convenience / OTC | Clotrimazole 1% cream x 7 days OR 2% cream x 3 days OR 500 mg single vaginal tablet |
| OTC with good suppository compliance | Miconazole 200 mg vaginal suppository x 3 days OR 1200 mg single dose |
| Oral preference | Fluconazole 150 mg single oral dose (requires prescription) |
| Failed topical azole | Switch to oral fluconazole - don't add a second topical azole |
| Non-albicans / recurrent | Boric acid 600 mg vaginal suppository x 14 days (after culture confirmation) |
The One Valid Antifungal Combination
- Katzung's Basic and Clinical Pharmacology, 16th ed., p. 1208: "Topical antifungal-corticosteroid fixed combinations have been introduced on the basis of providing more rapid symptomatic improvement than an antifungal agent alone."
Note of caution: Even clotrimazole-betamethasone should not be used on the vulva long-term - the high-potency steroid component can cause skin atrophy and telangiectasia in the thin vulvar skin.
Bottom Line
| Question | Answer |
|---|---|
| Can I use clotrimazole + miconazole together? | No - same mechanism, no benefit, more irritation |
| Can I use them on alternate days? | No - still redundant; pick one and complete the course |
| Should I switch if one fails? | Yes - but switch to a different class (oral fluconazole, or boric acid if non-albicans) |
| Is there any topical antifungal combination that makes sense? | Antifungal + steroid (e.g., clotrimazole + betamethasone) for inflammatory cases only |
Can apply cloteimazole plus betamethasone topically
Clotrimazole + Betamethasone Topically on the Vulva - Full Analysis
The Authoritative Answer: Generally NOT Recommended - especially on the vulva
"The combination of antifungals with potent topical steroids such as betamethasone dipropionate is not advised because of increased side effects from the steroid and decreased efficacy of the antifungal as a result of the concomitant steroid."
- Goldman-Cecil Medicine, p. 2883
"Combination products with a potent corticosteroid such as clotrimazole/betamethasone frequently produce widespread tinea and fungal folliculitis. Their use should be avoided."
- Andrews' Diseases of the Skin, p. 1957
Why the Combination is Problematic
1. Betamethasone Undermines the Antifungal
| Effect | Explanation |
|---|---|
| Immunosuppression | Betamethasone suppresses local immune response that helps clear fungal infection |
| Reduced antifungal efficacy | Steroids counteract the inflammatory response that is part of fungal clearance |
| Promotes fungal spread | Suppressed immunity allows Candida/dermatophytes to spread more widely |
| Tinea incognita | Steroid masks the clinical appearance - infection looks "cured" but is spreading underneath |
| Fungal folliculitis / Majocchi granuloma | Steroid drives infection deeper into hair follicles - very difficult to treat |
2. Betamethasone Dipropionate is HIGH Potency (Class II)
| Side Effect | Vulvar Significance |
|---|---|
| Skin atrophy | Vulvar skin becomes paper-thin, fragile, prone to fissuring |
| Telangiectasia / striae | Permanent and irreversible |
| HPA axis suppression | Systemic absorption is significantly higher at occluded genital skin |
| Secondary infection | Steroid-induced immunosuppression promotes candidal overgrowth - worsening the very condition you are treating |
| Rebound flare | When stopped, inflammation rebounds worse than before |
The combination is especially dangerous on the vulva because the occlusion effect of skin folds dramatically increases betamethasone absorption.
3. Clotrimazole Doesn't Need the Steroid
-
80% mycological cure with 7-day regimen
- Equivalent cure with 3-day or single 500 mg dose regimens
- Pruritus resolves within 1-3 days as infection clears
- (Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 3283)
When Might Clotrimazole-Betamethasone Have Any Role?
- Significant acute inflammation is present AND
- The fungal diagnosis is confirmed by KOH/culture AND
- Use is strictly short-term (maximum 1-2 weeks)
- Vulva or groin
- Face
- Any occluded / intertriginous area
- Unconfirmed fungal infection
- Children
- Long-term use anywhere
What TO Use Instead - Vulvar Candidiasis
| Goal | Correct Treatment |
|---|---|
| Treat candidiasis | Clotrimazole 1% cream alone x 7 days or Fluconazole 150 mg oral single dose |
| Relieve itch WHILE treating infection | Clotrimazole + short course of low-potency steroid separately (e.g., hydrocortisone 1% for 2-3 days only) as separate products - NOT combined betamethasone |
| Severe inflammation + confirmed candidiasis | Brief (3-5 days max) hydrocortisone 1% alongside antifungal - never betamethasone |
| Lichen sclerosus (non-infective cause) | Clobetasol 0.05% ALONE on confirmed diagnosis - but never combined with an antifungal |
Summary
| Question | Answer |
|---|---|
| Is clotrimazole + betamethasone safe on vulva? | No - high absorption, skin atrophy, suppresses antifungal efficacy |
| Does betamethasone help clear candidiasis faster? | No - it actively reduces antifungal efficacy and promotes spread |
| Is any steroid acceptable with antifungal for vulvar itch? | Only hydrocortisone 1% (low potency), briefly (2-3 days max), as a separate product |
| What is the correct first-line for vulvar candidal itch? | Clotrimazole alone or oral fluconazole |