Why sub total thyroidectomy is considered in elderly patients with multinodular goitte
Reading File
Finding Sources
Finding Sources
Searching the Web
subtotal thyroidectomy elderly multinodular goitre rationale anaesthetic risk
Reading File
Finding Sources
Reading File
I have enough information from the textbook. Let me now compile the full answer.
Why Subtotal Thyroidectomy is Considered in Elderly Patients with Multinodular Goitre
The choice of surgical procedure in multinodular goitre (MNG) is a balance between completeness of resection, operative risk, and long-term consequences. In elderly patients, subtotal thyroidectomy is considered for several interconnected reasons:
1. Reduced Operative and Anaesthetic Risk
Elderly patients frequently carry higher perioperative risk due to comorbidities (cardiovascular disease, respiratory compromise, reduced physiological reserve). A subtotal thyroidectomy - removing the bulk of the gland but leaving up to 8 g of relatively normal tissue in each remnant - is a less extensive operation than total thyroidectomy, reducing operative time and physiological stress.
2. Lower Risk of Permanent Complications
Total thyroidectomy carries a higher rate of two major permanent complications:
- Hypoparathyroidism - removing all thyroid tissue increases the risk of inadvertently devascularising or excising all four parathyroid glands, causing permanent hypocalcaemia
- Bilateral recurrent laryngeal nerve (RLN) injury - total thyroidectomy requires bilateral RLN dissection; subtotal resection reduces exposure on the less-affected side
In elderly patients, these complications are particularly poorly tolerated and harder to manage long-term.
3. Recurrence is Less Clinically Relevant in the Elderly
The main drawback of subtotal thyroidectomy is regrowth of the remnant - a significant concern in younger patients who face decades of potential recurrence and the hazards of reoperation. In the elderly, however:
- The remaining life expectancy means the goitre is unlikely to regrow to a clinically significant size within the patient's lifetime
- Reoperation for recurrent goitre is technically difficult and hazardous (scarring distorts anatomy, increasing RLN and parathyroid risk); this risk is more acceptable to accept in theory than to face in practice for an elderly patient who may never need it
As Bailey & Love states: "In young patients, total thyroidectomy should be considered... subtotal resections run the risk of later growth of the remnant and, if a second operation is required years later, this greatly increases the risk to the RLN and parathyroid glands." The implication is that this concern is attenuated in older patients.
4. Preservation of Thyroid Function (Avoiding Lifelong Thyroxine)
Total thyroidectomy mandates immediate and lifelong thyroxine replacement. In elderly patients:
- Compliance with lifelong medication may be an issue
- Thyroxine replacement in the elderly requires careful titration (risk of precipitating atrial fibrillation or angina with over-replacement)
- Subtotal thyroidectomy, by conserving sufficient functioning tissue, allows normal thyroid function to continue without replacement in many patients
5. The Dunhill Procedure as a Middle Ground
When MNG is asymmetric (one lobe more affected), total lobectomy on the more affected side is appropriate, particularly in older patients. This can be combined with subtotal resection of the contralateral lobe (the Dunhill procedure), though many surgeons now prefer no intervention on the less-affected side to avoid reoperation risk entirely.
Summary Table
| Factor | Why it favours subtotal in the elderly |
|---|---|
| Operative risk | Less extensive surgery, shorter time, less physiological stress |
| Hypoparathyroidism | Less parathyroid exposure/risk |
| RLN injury | Less bilateral nerve dissection |
| Recurrence risk | Reduced life expectancy means regrowth unlikely to cause problems |
| Reoperation hazard | Less relevant if regrowth unlikely within lifetime |
| Thyroxine dependence | Avoided if sufficient tissue preserved |
In practice, the modern trend (even in the elderly) is shifting toward total thyroidectomy when bilateral disease is diffuse, as it eliminates recurrence entirely and completion thyroidectomy after unilateral lobectomy is straightforward. But for elderly, high-risk patients with asymmetric disease or significant comorbidities, subtotal resection or lobectomy alone remains a well-justified, safer approach.
- Bailey and Love's Short Practice of Surgery, 28th Edition, pp. 879-882
Colloid goitte vs follicular adenoma
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to deliver a detailed, well-illustrated comparison. Let me compile the full answer.
Colloid Goitre vs Follicular Adenoma - A Comparison
These are two distinct thyroid lesions that can both present as a thyroid swelling, but differ fundamentally in their nature, pathology, and management.
1. Basic Nature
| Feature | Colloid Goitre | Follicular Adenoma |
|---|---|---|
| Nature | Non-neoplastic hyperplastic/involutional change | True benign neoplasm |
| Origin | Entire gland - diffuse or multinodular | Single clone of follicular epithelial cells |
| Encapsulation | No true capsule (part of gland parenchyma) | Complete, circumferential fibrous capsule |
| Malignant potential | None (but nodular goitre has low overall risk) | None - but cannot be distinguished from follicular carcinoma on FNAC alone |
2. Aetiology & Pathogenesis
Colloid Goitre
- Results from cycles of TSH-driven hyperplasia (increased demand) followed by involution (when demand falls)
- During hyperplasia: gland enlarges, follicles are small and active
- During involution (when TSH stimulation ceases): follicles become inactive, enlarge, and fill with colloid - producing a colloid goitre
- Fluctuating TSH levels over time produce alternating areas of active and inactive lobules, eventually resulting in multinodular goitre
- Causes: iodine deficiency (endemic), puberty, pregnancy, goitrogens
Follicular Adenoma
- True monoclonal neoplasm arising from follicular epithelial cells
- Not dependent on TSH cycling
- Aetiology largely unknown; radiation exposure is a risk factor
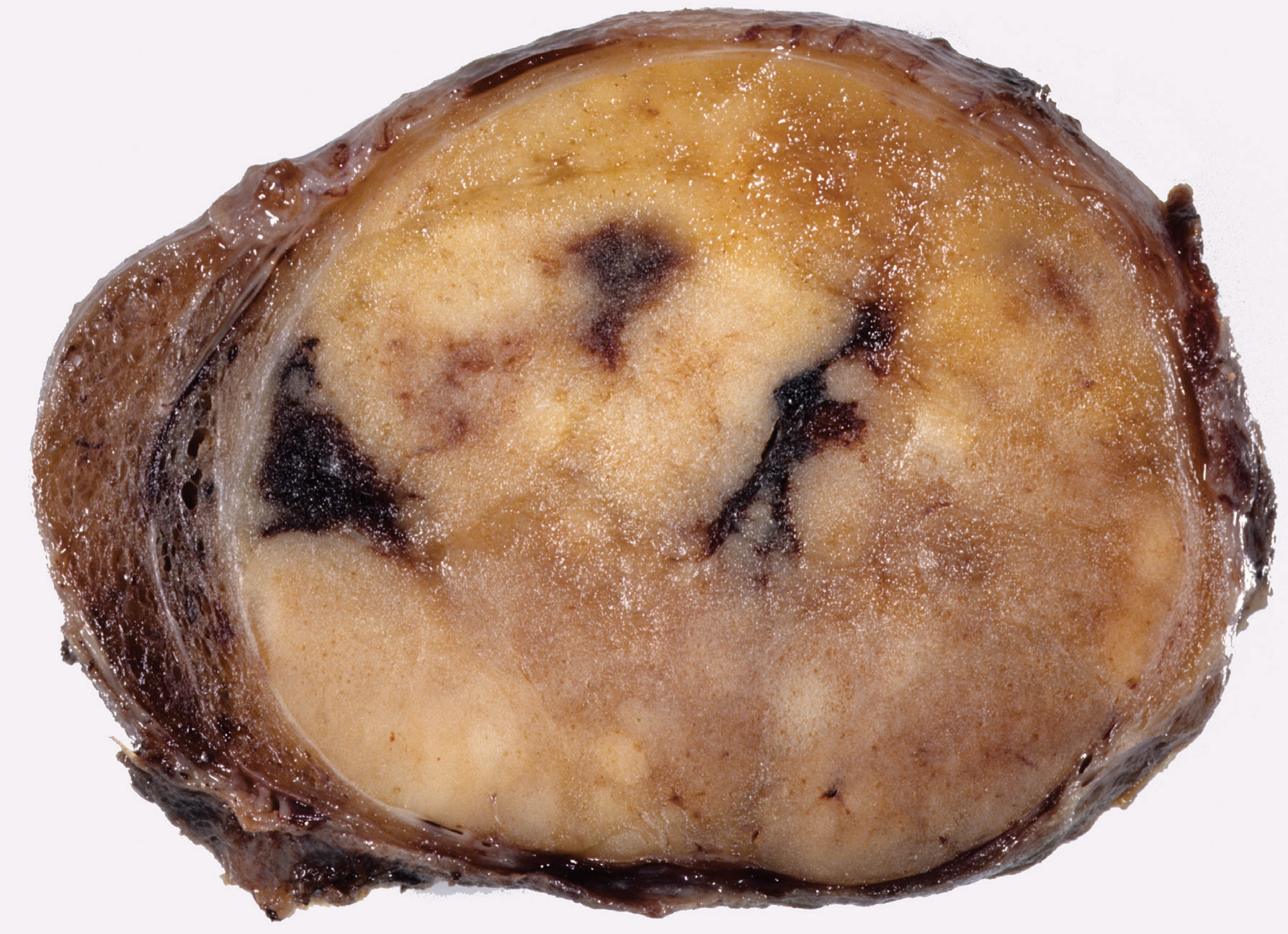
3. Gross Pathology (Macroscopy)
Colloid Goitre
- Whole gland enlarged, soft, elastic
- Cut surface: multiple nodules separated by fibrous septa, with areas of haemorrhage, necrosis, calcification, and cystic change (in multinodular form)
- Nodules contain amber/brown gelatinous colloid
- No capsule separating nodule from surrounding parenchyma
Follicular Adenoma
- Solitary, well-defined, encapsulated nodule
- Cut surface: fleshy, uniform, tan-yellow to pale, with possible localised cystic change
- Surrounded by a uniformly slender fibrous capsule - the capsule compresses the adjacent normal thyroid
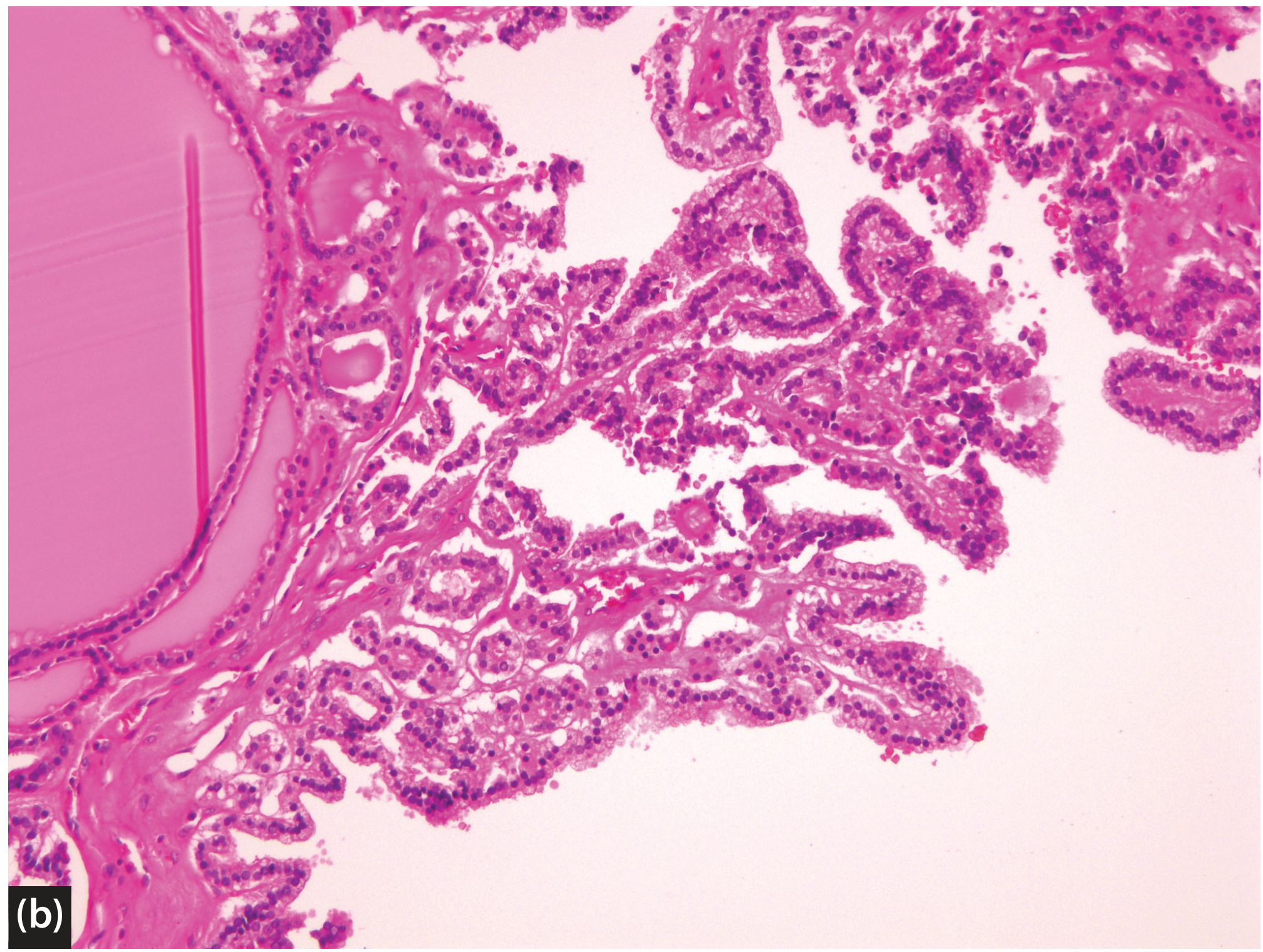
4. Histopathology (Microscopy)
Colloid Goitre
- Variably-sized follicles (macro and micro)
- Follicles distended with abundant eosinophilic colloid
- Flattened, inactive follicular epithelium
- Fibrous septa between nodules (but no true capsule)
- Areas of haemorrhage, haemosiderin deposits, cholesterol clefts, calcification
- Papillary hyperplastic nodules may form (localized papillary proliferations immersed in colloid - with simple, bland, well-polarized cells - NOT papillary carcinoma)
Follicular Adenoma
- Complete circumferential fibrous capsule (smooth, slender, uniform thickness - capsular thickening warrants search for carcinoma)
- Internal architecture may be: normofollicular, microfollicular (foetal), macrofollicular (colloid), solid, trabecular, or organoid - fairly uniform within a given tumour
- Mitoses are few
- No capsular invasion, no vascular invasion - this is the critical distinguishing feature from carcinoma
- Surrounding native thyroid tissue is compressed or atrophic
- No nuclear features of papillary thyroid carcinoma (no nuclear grooves, inclusions, or clearing)
5. Key Distinguishing Features
| Feature | Colloid Goitre | Follicular Adenoma |
|---|---|---|
| Capsule | Absent (pseudo-capsule at most) | Complete, true fibrous capsule |
| Number | Multiple nodules (or diffuse) | Solitary (usually) |
| Follicle size | Large, dilated, colloid-filled | Variable (micro/normo/macrofollicular) |
| Surrounding gland | Other nodules/abnormal gland adjacent | Compressed/atrophic normal gland |
| Haemorrhage/calcification | Common (in multinodular form) | Less common (may occur post-FNAC) |
| Architecture | Heterogeneous between nodules | Uniform within the tumour |
| Clonal origin | Polyclonal (hyperplastic) | Monoclonal (neoplastic) |
| Vascular/capsular invasion | Not applicable (no capsule) | Absent (present = carcinoma) |
6. FNAC Findings
| Colloid Goitre | Follicular Adenoma | |
|---|---|---|
| Cellularity | Low to moderate | Variable (may be high) |
| Colloid | Abundant | Variable |
| Follicular cells | Flat, monolayered, bland | May show mild atypia |
| Thy classification | Thy1 (non-diagnostic) or Thy2 (benign) | Thy3 (indeterminate - Flk/FN) |
| Diagnosis on FNAC | Can be diagnosed as benign | Cannot distinguish from follicular carcinoma - requires histology |
This is the most clinically important distinction: a colloid goitre can be confidently called benign on FNAC, while a follicular adenoma invariably returns as Thy3F (follicular neoplasm) because capsular integrity (the only criterion separating adenoma from carcinoma) cannot be assessed on cytology.
7. Clinical Presentation
| Colloid Goitre | Follicular Adenoma | |
|---|---|---|
| Age | 20-30 years (colloid stage); 30-40 years (multinodular) | Any age; usually adult |
| Sex | Females > Males (6:1 for MNG) | Females > Males |
| Number | Bilateral/multiple | Solitary |
| Function | Euthyroid (usually); secondary toxicity in ~25% over time | Usually euthyroid; may be toxic (autonomous adenoma) |
| Consistency | Soft to firm; variable | Firm, uniform |
| Complications | Haemorrhage, calcification, secondary toxicosis, malignant change (rare) | Malignancy excluded only on histology |
8. Management
Colloid Goitre
- Observe if asymptomatic and small
- Thyroxine supplementation (suppresses TSH, may reduce size in early stages)
- Surgery (thyroidectomy) for: pressure symptoms, cosmesis, suspicion of malignancy, secondary toxicosis
- Iodine supplementation in endemic areas (prevents, not treats)
Follicular Adenoma
- Thy3F on FNAC mandates surgery (hemithyroidectomy/lobectomy) - cannot exclude carcinoma pre-operatively
- Definitive diagnosis only on histology (requires complete capsular assessment)
- If histology confirms adenoma (no capsular/vascular invasion) - no further treatment needed
- If capsular/vascular invasion found - completion thyroidectomy +/- radioiodine
Summary
A colloid goitre is a non-neoplastic, polyclonal, involutional change in the whole gland - characterised by inactive follicles distended with colloid, no true capsule, and a benign FNAC result. A follicular adenoma is a true neoplasm - monoclonal, completely encapsulated, solitary - whose benign nature can only be confirmed on histology by the absence of capsular and vascular invasion.
- S Das - A Manual on Clinical Surgery, 13th Edition, pp. 393-396
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, pp. 712-713
- Bailey and Love's Short Practice of Surgery, 28th Edition
Symptoms of sympathetic stimulation
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
I now have all the information needed for a thorough answer. Here is the complete response:
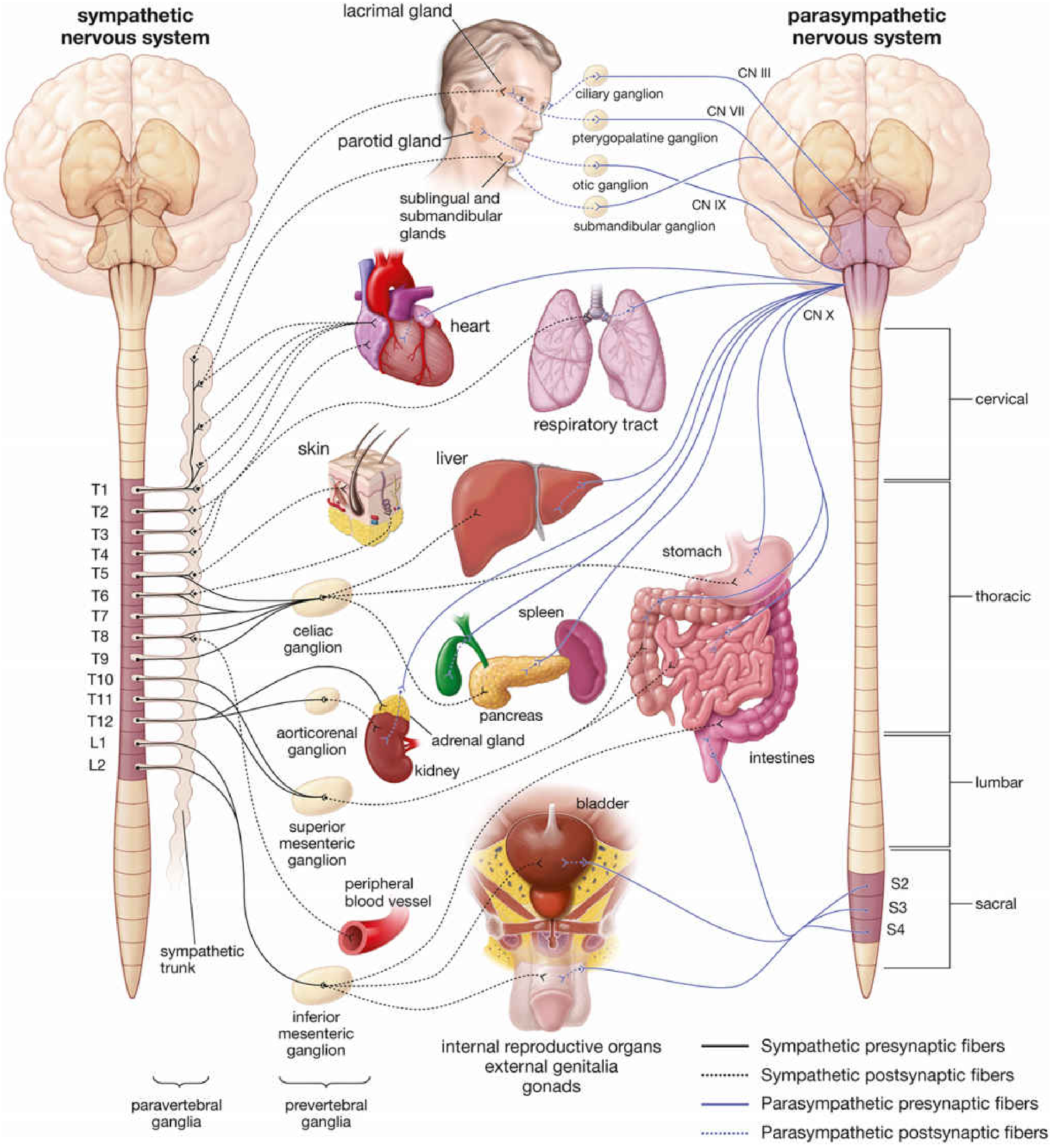
Symptoms of Sympathetic Stimulation ("Fight or Flight")
The sympathetic nervous system (SNS) originates from the thoracolumbar outflow (T1-L2). Its postganglionic neurons release norepinephrine (NE), while the adrenal medulla (a modified ganglion) releases mostly epinephrine (adrenaline) into the blood. Effects are mediated via α1, α2, β1, and β2 adrenergic receptors.
System-by-System Effects
1. Cardiovascular
| Effect | Receptor | Mechanism |
|---|---|---|
| Tachycardia (↑ heart rate) | β1 | SA node firing rate increased |
| ↑ Myocardial contractility | β1 | Positive inotropic effect |
| ↑ Conduction velocity (AV node) | β1 | Faster impulse propagation |
| Vasoconstriction (skin, viscera, mucosae) | α1 | Smooth muscle contraction |
| Vasodilation (skeletal muscle) | β2 | Smooth muscle relaxation |
| ↑ Blood pressure | α1 + β1 | Combined ↑ cardiac output + peripheral resistance |
2. Respiratory
| Effect | Receptor |
|---|---|
| Bronchodilation | β2 - smooth muscle relaxation |
| ↑ Respiratory rate | Central + β2 |
| Reduced bronchial secretions | α1 |
3. Eyes
| Effect | Receptor |
|---|---|
| Mydriasis (pupil dilation) | α1 - radial (dilator) muscle contraction |
| Retraction of upper eyelid (lid lag) | α1 - superior tarsal muscle (Müller's) |
| Decreased aqueous humor production | β2 |
4. Gastrointestinal
| Effect | Receptor |
|---|---|
| ↓ GI motility and peristalsis | α1, β2 - smooth muscle relaxation |
| Contraction of GI sphincters | α1 |
| ↓ GI secretions | α1, α2 |
| Inhibition of defecation | α1 sphincter contraction |
5. Urinary Tract
| Effect | Receptor |
|---|---|
| Relaxation of detrusor muscle (bladder wall) | β2 - urine retention |
| Contraction of internal urethral sphincter | α1 - inhibits micturition |
6. Skin / Glands
| Effect | Receptor |
|---|---|
| Sweating (diaphoresis) | Muscarinic (cholinergic sympathetic - exception!) |
| Piloerection ("goosebumps") | α1 - arrector pili muscle contraction |
| Vasoconstriction of skin vessels → pallor | α1 |
| ↓ Salivary secretion (thick, viscid saliva) | α1 |
| ↓ Lacrimal secretion | α1 |
7. Metabolic Effects
| Effect | Receptor | Purpose |
|---|---|---|
| Glycogenolysis (liver + muscle) | β2, α1 | ↑ Blood glucose |
| Gluconeogenesis (liver) | β2 | Further raise blood glucose |
| Lipolysis (adipose tissue) | β3 | Release free fatty acids |
| ↓ Insulin secretion | α2 (pancreatic β cells) | Prevent glucose uptake, keep blood glucose high |
| ↑ Glucagon secretion | β2 | Promotes glucose release |
| ↑ Basal metabolic rate | β2 | Heat generation |
8. Adrenal Medulla
- Sympathetic preganglionic fibres directly innervate chromaffin cells
- Release epinephrine (80%) + norepinephrine (20%) into bloodstream
- Amplifies and prolongs all sympathetic effects systemically
9. Reproductive System
| Effect | Receptor |
|---|---|
| Ejaculation (male) | α1 - smooth muscle of vas deferens, seminal vesicles |
| Uterine relaxation (pregnant) | β2 |
| Vasoconstriction of genital vessels | α1 |
Memory Aid: The "Fight or Flight" Mnemonics
"The body prepares to fight or flee"
- Heart: beats faster and harder
- Lungs: open up (bronchodilation)
- Muscles: get more blood (vasodilation)
- Skin/Gut: blood diverted away (vasoconstriction)
- Eyes: open wide (mydriasis, lid retraction)
- Fuel: glucose and fats mobilised
- Bladder/Gut: activities stopped (sphincters close, motility ↓)
- Sweat: produced to cool the working body
Receptor Summary
| Receptor | Location | Sympathetic Effect |
|---|---|---|
| α1 | Smooth muscle (vessels, GI sphincters, bladder neck, pupil, piloerection) | Contraction (vasoconstriction, sphincter closure, mydriasis) |
| α2 | Presynaptic terminals, pancreas | ↓ NE release (autoreceptor), ↓ insulin |
| β1 | Heart, kidney (JGA) | ↑ HR, ↑ contractility, ↑ renin |
| β2 | Bronchi, blood vessels (skeletal), uterus, liver | Relaxation, bronchodilation, glycogenolysis |
| β3 | Adipose tissue | Lipolysis |
Clinical Correlates
These effects explain the symptoms seen when the SNS is pathologically overactivated:
-
Phaeochromocytoma: hypertension, tachycardia, sweating, pallor, headache
-
Hyperthyroidism: mimics SNS activation (β-receptors upregulated by T3)
-
Panic attacks: same fight-or-flight response triggered inappropriately
-
β-blockers selectively block β1/β2 to treat hypertension, tachyarrhythmias, and anxiety
-
Histology: A Text and Atlas with Correlated Cell and Molecular Biology, pp. 988-990
-
Medical Physiology (Boron & Boulpaep)
-
Goldman-Cecil Medicine - Adrenal Medulla and Catecholamines
This is a shared conversation. Sign in to Orris to start your own chat.