Give me a brief account on musculoskeletal imaging… spine and extremities
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have rich, comprehensive content from the textbooks. Let me compile the full answer.
Musculoskeletal Imaging: Spine and Extremities
A broad account drawn from Grainger & Allison's Diagnostic Radiology, Imaging Anatomy: Bones, Joints, Vessels and Nerves (THIEME Atlas Vol. 3), Goldman-Cecil Medicine, and Tintinalli's Emergency Medicine.
Imaging Modalities - General Principles
Musculoskeletal imaging relies on a combination of modalities selected based on the tissue type and clinical question:
| Modality | Best For |
|---|---|
| Plain radiograph (X-ray) | Bony alignment, fractures, hardware follow-up, scoliosis assessment in upright position |
| CT | Precise cortical detail, fracture characterization, implant integrity, bony tumour extent |
| MRI | Soft tissue (cartilage, ligaments, tendons, labrum, disc, cord), marrow pathology, infection |
| Ultrasound (US) | Peripheral tendons, ligaments, bursae, guided injections, dynamic assessment |
| Nuclear medicine / PET | Metabolic bone disease, occult fractures, infection, tumour staging |
MRI and US complement plain radiography and CT in the detailed assessment of tendons, ligaments, cartilage, and fibrocartilaginous structures - allowing prognosis for conservative management and planning for surgical decision-making. - Grainger & Allison's Diagnostic Radiology
Part I: SPINE IMAGING
Bony Anatomy Background
The vertebrae are composed of roughly one-third cortical bone and two-thirds trabecular bone. The trabecular component provides the major mechanical support in the vertebral bodies. The skeleton overall includes 74 bones in the axial skeleton (which encompasses the spine). - Imaging Anatomy: Bones, Joints, Vessels and Nerves
Initial Evaluation
In awake, alert patients with possible cervical spine injury, clinical decision rules (e.g., the Canadian C-Spine Rule) can reduce unnecessary imaging without adverse outcomes. The general radiological evaluation approach is:
- Plain radiographs first - anteroposterior, lateral, and odontoid views for cervical spine; AP and lateral for thoracic/lumbar
- CT for bony abnormalities identified on plain film, or in obtunded patients where a high-quality CT effectively excludes cervical injury
- MRI when ligamentous injury, disc herniation, cord injury, or paravertebral soft tissue pathology is suspected
After blunt trauma, if plain films and CT of the cervical spine are normal but neck pain persists, ligamentous injury must be considered. The patient should remain in a rigid cervical collar until one of these criteria is met: (1) pain resolves, (2) dynamic flexion/extension radiographs are normal, or (3) MRI within 48 hours is normal. - Goldman-Cecil Medicine
A chest radiograph is useful to evaluate the lower cervical and thoracic vertebrae; a pleural effusion in the context of possible thoracic spine injury suggests hemothorax.
Cervical Spine
Imaging order: Plain films → CT → MRI
- CT is preferred in high-energy trauma and obtunded patients
- Dynamic flexion/extension views are used to assess instability
- MRI is the modality of choice for cord compression, disc herniation, epidural haematoma, and ligamentous injury
Thoracic and Lumbar Spine
- Plain films assess alignment, vertebral height, and pedicle integrity
- CT better characterises burst fractures, retropulsed fragments, and posterior element injuries
- MRI adds information on cord/conus, disc, and posterior ligamentous complex integrity
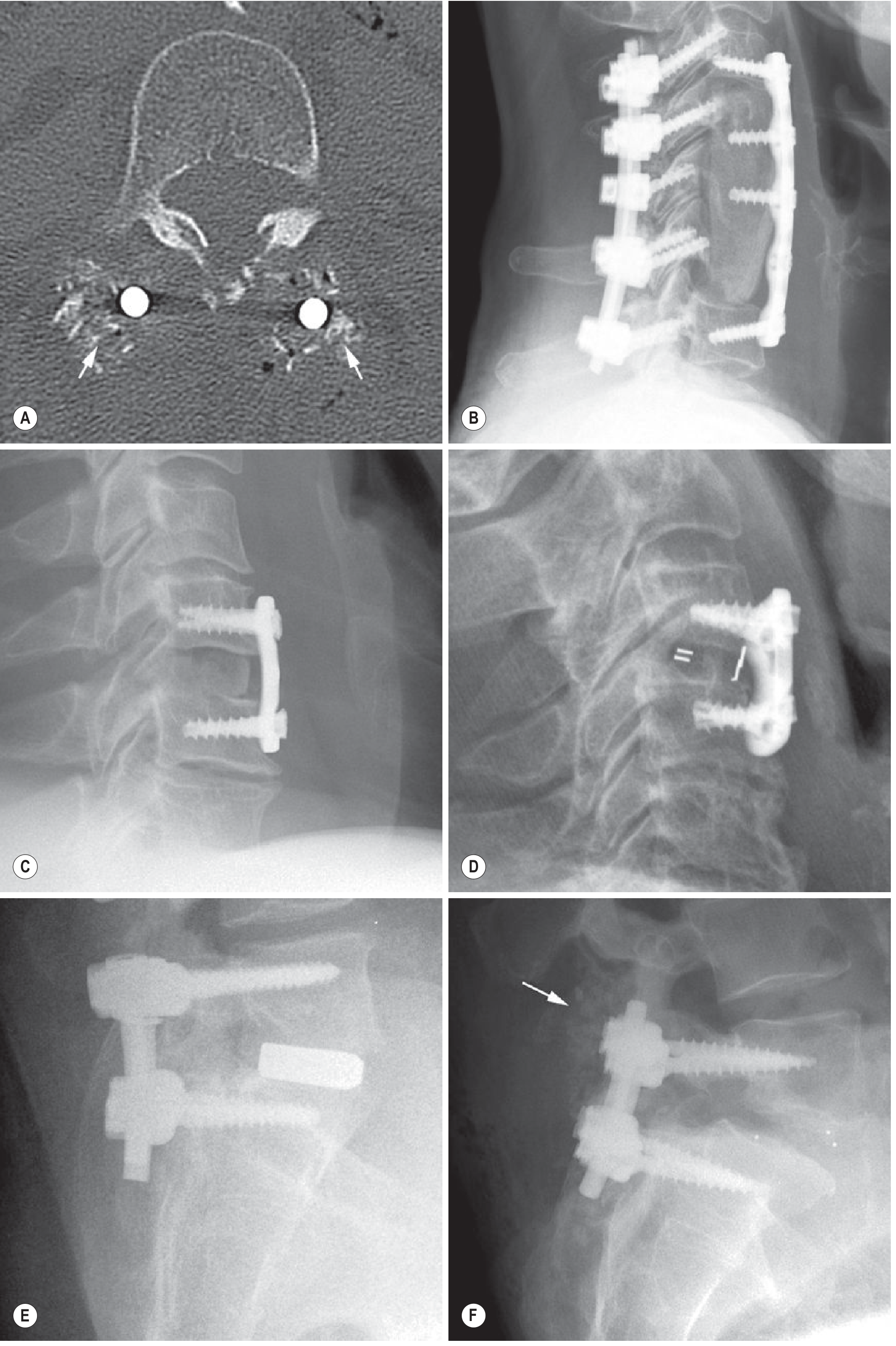
Postoperative Spine
Plain radiographs are the first-line follow-up tool for instrumented spines. They are inexpensive, fast, and the only modality that can image the patient upright. AP and lateral views can be supplemented with flexion/extension projections to evaluate for motion at the fusion site (pseudoarthrosis) and adjacent segment instability.
CT provides precise evaluation of implant position, alignment, integrity, and fusion status. Because most implants are made of titanium or cobalt-chromium, CT has lower beam-hardening artefact compared with steel hardware.
MRI remains the technique of choice to assess soft tissues and neural structures postoperatively, with metal artefact reduction sequences (MARS) significantly improving image quality around hardware.
Spine in Axial Spondyloarthritis
MRI of the spine is the gold standard for detection of active inflammatory lesions (bone marrow oedema in Romanus lesions, disco-vertebral lesions) before structural damage becomes apparent on X-ray. STIR and T1-weighted sequences are routinely used.
Part II: EXTREMITY IMAGING
Bone Anatomy and Imaging Basics
The appendicular skeleton contains 126 bones. Long bones (femur, metacarpals, phalanges) have a tubular diaphysis, metaphyses, epiphyses, and a growth plate. The cortex comprises 80% of skeletal mass. Trabecular (cancellous) bone fills the metaphyses and epiphyses in a honeycomb meshwork and is the major site of haematopoiesis. - Imaging Anatomy: Bones, Joints, Vessels and Nerves
Bone marrow imaging: MRI is uniquely suited to assess marrow composition. Red (haematopoietic) marrow converts to yellow (fatty) marrow in a predictable pattern from peripheral to central; reconversion (yellow → red) occurs in states of increased haematopoietic demand. Signal characteristics on T1 and STIR sequences distinguish normal conversion from infiltrative pathology.
The Shoulder
The shoulder is the most mobile joint in the body. The glenohumeral joint (GHJ) provides a shallow cup (glenoid) articulating with the large humeral head - likened to a "golf ball on a golf tee" - and is inherently unstable. Stability is provided by:
- Rotator cuff: subscapularis, supraspinatus, infraspinatus, teres minor
- Labrum: fibrocartilaginous ring deepening the glenoid cavity
- Ligaments: glenohumeral ligaments reinforcing the capsule
- Bursae: subacromial, subdeltoid, and subscapularis bursae
Imaging approach:
- Plain X-ray: first-line for trauma, alignment, calcific tendinopathy, and AC/SC joint assessment
- MRI: modality of choice for rotator cuff pathology (tears, tendinopathy), labral tears, instability, and osteochondral injury
- MR arthrography: intra-articular gadolinium improves detection of partial-thickness undersurface cuff tears and subtle labral pathology
- US: dynamic real-time assessment of supraspinatus and biceps tendons; guided injections
Common pathology on MRI:
- Rotator cuff tears: fluid signal within/through tendon fibres, typically in the critical zone of supraspinatus
- Subacromial impingement: bursitis, supraspinatus tendinopathy, and bone changes at the coracoacromial arch
- Bankart lesion (inferior glenohumeral ligament-labral complex tear) in anterior instability
- SLAP tears at the superior labrum-biceps anchor
The Hip
The hip is a deep ball-and-socket joint offering stability via the deep acetabulum, fibrocartilaginous labrum, iliofemoral/ischiofemoral/pubofemoral ligaments, and hyaline articular cartilage. The blood supply of the femoral head in adults comes primarily from the circumflex femoral arteries; disruption causes avascular necrosis (AVN).
Imaging approach:
- Plain X-ray: AP pelvis and frog-leg lateral views; first-line for OA, fractures, cam/pincer deformity
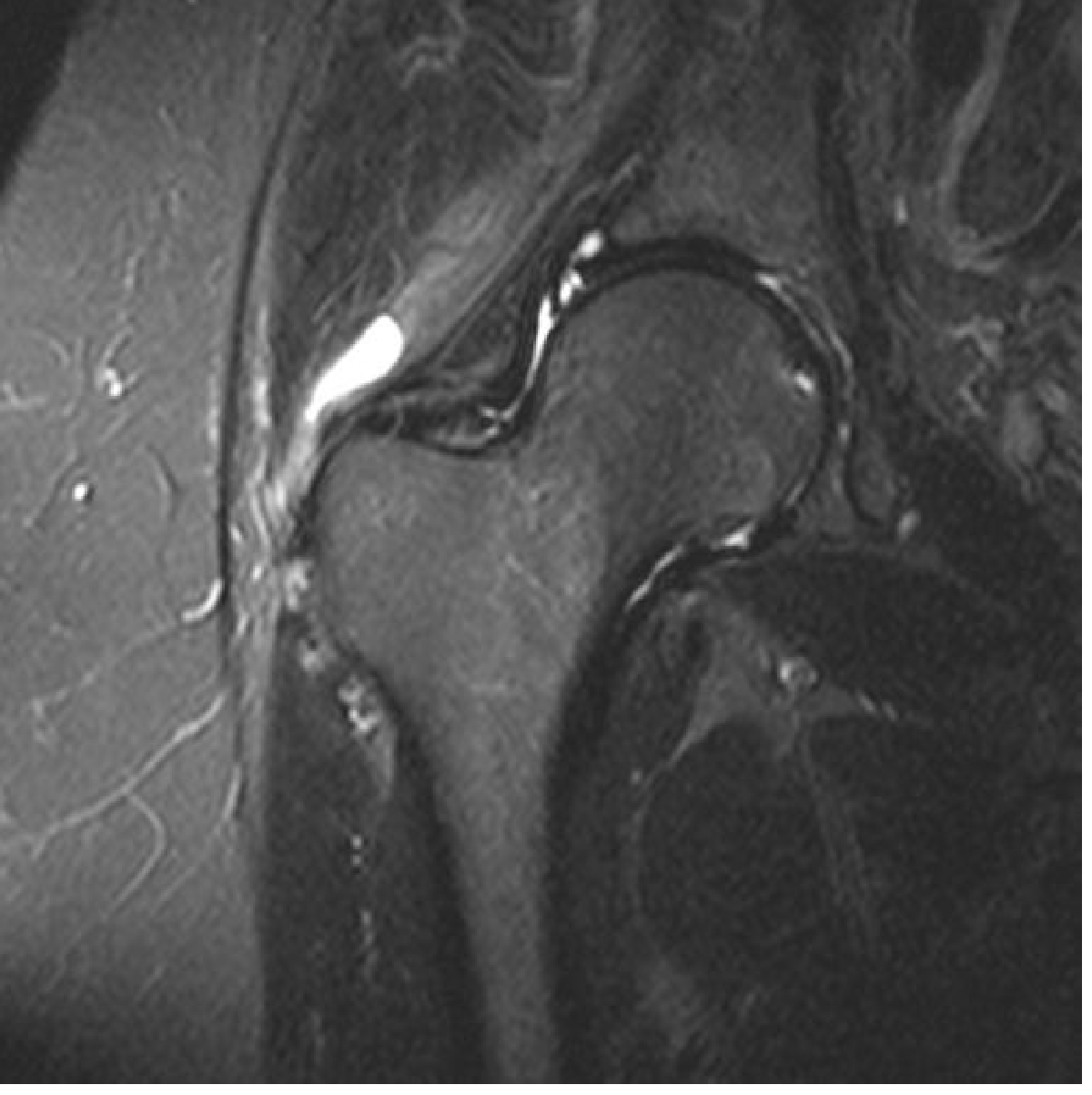
- MRI: gold standard for labral tears, AVN, femoroacetabular impingement (FAI), cartilage assessment, and stress fractures
- High-field (3T) MRI with small FOV (16-18 cm) and surface coil is standard
- MR arthrography (intra-articular gadolinium) improves detection of subtle cartilage lesions
- Radial imaging planes visualise the labrum in cross-section around the entire acetabular rim
- US: for bursitis, tendinopathy, guided injections
Key findings:
- Labral tears appear as fluid signal undercutting or extending into the labrum; anterosuperior portion most commonly affected; paralabral cysts are a secondary sign
- Cam deformity (non-spherical femoral head bump) causes abutment → labral and cartilage damage
- AVN appears on MRI as a "double-line sign" on T2: outer low signal (sclerosis) and inner high signal (granulation tissue)
- Greater trochanteric pain syndrome: fluid in trochanteric bursae + gluteus medius/minimus tendinopathy on coronal fat-saturated T2
The Knee
The knee is the largest joint in the body, comprising three compartments: medial tibiofemoral, lateral tibiofemoral, and patellofemoral. Bony articular surfaces alone are unstable; the supporting soft-tissue structures (menisci, cruciate and collateral ligaments) are inherently prone to injury.
MRI is the imaging modality of choice for internal derangements of the knee. It is well suited for demonstrating menisci, tendons, and ligaments. US demonstrates peripheral structures (MCL/LCL, extensor mechanism) well. - Grainger & Allison's Diagnostic Radiology
Menisci
- Two semilunar fibrocartilaginous structures between femoral and tibial condyles
- Normal MRI appearance: uniform low signal on all sequences ("bow-tie" on sagittal peripheral sections)
- Short TE sequences (T1-weighted or proton density PD-weighted) are most sensitive for tears
- Tear types: radial, horizontal, longitudinal, bucket-handle; bucket-handle tears cause the "double PCL" sign
- Discoid lateral meniscus (5% of population): increased risk of degeneration from a young age
Cruciate Ligaments
- ACL: best assessed on sagittal and coronal MRI; tear causes oedema, discontinuity, abnormal signal; associated with bone bruising of the lateral femoral condyle/posterior tibial plateau
- PCL: tears less common; sagittal MRI preferred
Collateral Ligaments and Bursae
- MCL/LCL well visualised on coronal MRI and US
- Semimembranosus-gastrocnemius bursa (Baker's cyst): T2 bright popliteal fossa structure
Extensor Mechanism and Patellofemoral
- Patellar tendinopathy at the patellar apex (jumper's knee): MRI shows signal change and thickening
- Trochlear dysplasia and patellar tilt/subluxation assessed on axial MRI/CT
The Elbow and Wrist
- Common flexor and extensor origin tendinopathy (lateral and medial epicondylitis): MRI and US show thickening and intratendinous signal change; US-guided injection/needling used for refractory cases
- Wrist: falls on outstretched hand cause scaphoid fractures (MRI most sensitive in first 10 days), TFCC tears, and carpal instability
- Scaphoid fractures may be occult on plain film; MRI within 24-48 hours avoids missed injury and prolonged immobilisation
- CT arthrography or MR arthrography used for TFCC assessment
Summary of Imaging Modality Selection
| Region | First-Line | Advanced |
|---|---|---|
| Cervical spine - trauma | X-ray / CT | MRI (cord, ligaments) |
| Lumbar spine - disc/nerve | X-ray | MRI |
| Postoperative spine | X-ray (upright) | CT (hardware) / MRI (neural) |
| Shoulder soft tissue | X-ray | MRI or MR arthrography |
| Hip labrum/cartilage | X-ray | 3T MRI / MR arthrography |
| Hip AVN | X-ray | MRI (double-line sign) |
| Knee ligaments/menisci | X-ray | MRI (PD/T2 sequences) |
| Elbow/wrist tendons | X-ray | US / MRI |
| Occult fractures | X-ray (often negative) | MRI (most sensitive) |
Sources: Grainger & Allison's Diagnostic Radiology (Elsevier, 2022) • Imaging Anatomy: Bones, Joints, Vessels and Nerves (THIEME Atlas Vol. 3) • Goldman-Cecil Medicine (2022) • Tintinalli's Emergency Medicine (9th Ed.)
This is a shared conversation. Sign in to Orris to start your own chat.